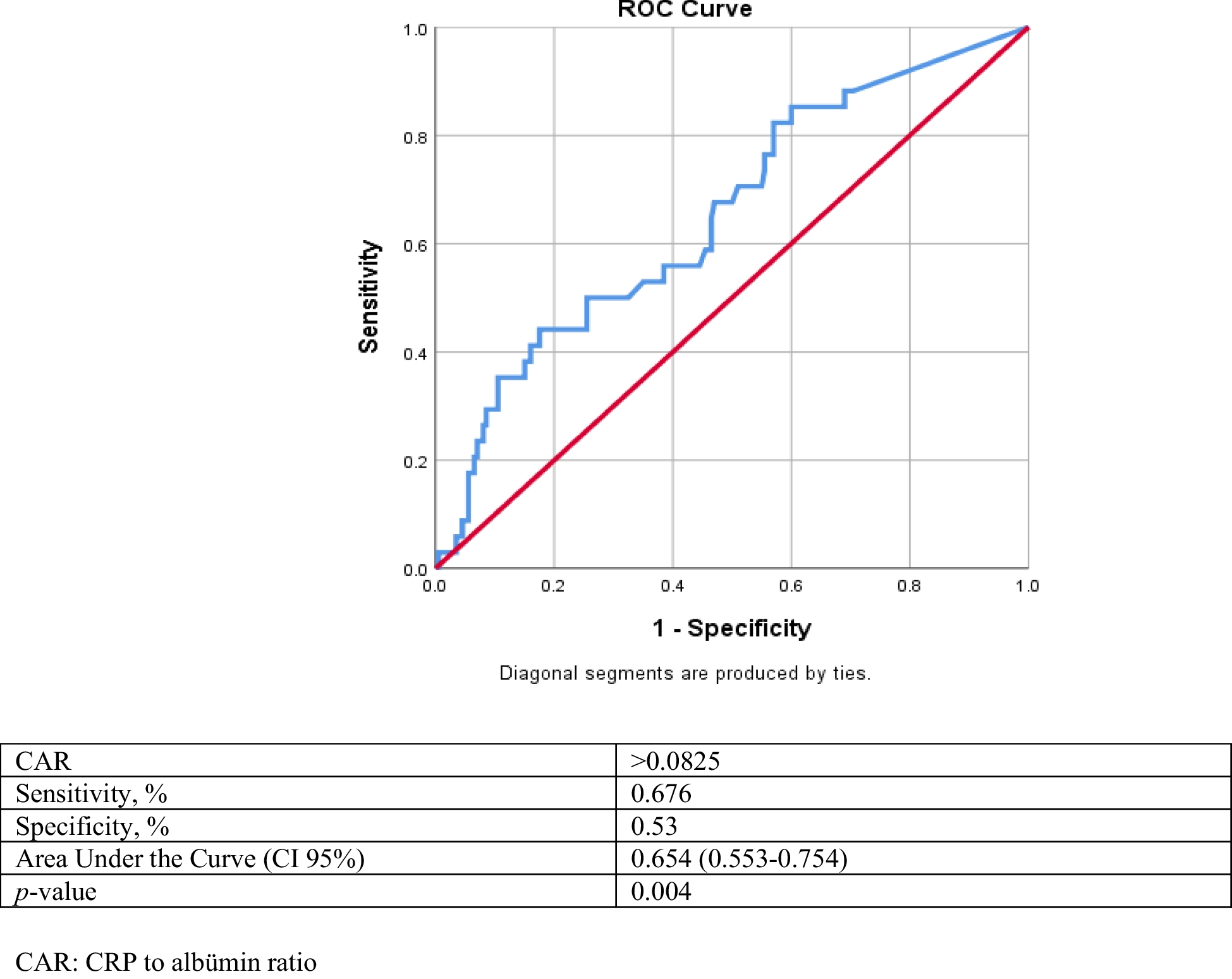
The development of scrotal involvement in patients with IgA vasculitis is important as it may alter disease management. In the present study, scrotal involvement was shown to develop in approximately 14.5% of male patients with IgA vasculitis. Patients with scrotal involvement had more widespread skin involvement, local edema, penile involvement and hematuria than those without scrotal involvement. PVAS > 2 was found to be a predictor of scrotal involvement. However, an increase in systemic inflammatory markers such as NLR and PLR was not associated with scrotal involvement. On the other hand, CAR, the ratio of CRP to albumin, had higher specificity and sensitivity than the other two markers in predicting scrotal involvement.
Scrotal involvement develops rarely in patients with IgA vasculitis [5,6,7]. As found in our study, unilateral scrotum pain, tenderness and swelling are the most common clinical findings. While scrotal involvement is usually observed during the follow-up of the disease, it may occur as the first manifestation of the disease in only one fourth of patients [5, 6, 17, 18].
Imaging abnormalities such as enlargement of the epididymis, thickening of the scrotal skin, hydrocele with normal testicular blood flow may be detected [5, 19]. Scrotal US can both confirm scrotal involvement and reveal a critical complication such as testicular torsion. In our study, the most common US findings were epididymal swelling, increased testicular vascularity, scrotal fluid collection, scrotal edema, and scrotal wall thickening. Bilateral epididymal swelling and increased testicular vascularity were more common than unilateral. Fortunately, none of the patients had US findings of testicular torsion. However, it should be kept in mind that repeat US should be performed in patients with suspected testicular torsion during follow-up.
Given the need to adjust treatment in the presence of scrotal involvement, it is important to differentiate between patients with and without scrotal involvement. Thus, the clinician can closely follow patients who are likely to develop scrotal involvement. Ha et al. found that localized edema and central nervous system involvement were more common in patients with scrotal involvement [6]. Recently, it was shown that the frequency of scrotal involvement increased with renal involvement [8]. On the other hand, Buscatti et al. found no difference in terms of organ or system involvement in IgA vasculitis patients with or without scrotal involvement [5]. In our study, GI tract involvement, renal involvement and arthritis were similar in patients with and without scrotal involvement. However, widespread skin involvement and local edema were more frequent in patients with scrotal involvement compared to those without.
The PVAS, the pediatric version of the Birmingham Vasculitis Activity Score (BVAS), provides outcome scores for vasculitis. With PVAS, it may be possible to determine the activity and severity of vasculitis, provide a standardized management, and even predict some system involvement that may develop during the course of vasculitis. However, given the rarity of childhood vasculitis, there are very few studies presenting PVAS results in childhood vasculitis such as IgA vasculitis, Takayasu arteritis, and polyarteritis nodosa [20]. Feng et al. reported that PVAS is effective in assessing disease activity in Takayasu arteritis and its use is recommended in patients with renal damage [21]. Avci et al. showed that PVAS score was higher in IgA vasculitis with nephritis and also independent predictor for development of nephritis in patients with IgA vasculitis [22]. In previous studies, a threshold value of 2 was used to determine low and/or high disease activity in pediatric patients with vasculitis [15]. In our study, PVAS > 2 had 41% sensitivity, and 78% specificity for predicting scrotal involvement in patients with IgA vasculitis. PVAS > 2 also was independent predictor for scrotal involvement in patients with IgA vasculitis. Validation of the threshold value of the PVAS in larger scale studies and determination of different PVAS threshold values for the mild to severe spectrum of IgA vasculitis will enable more reliable and widespread use of this tool.
It was reported that markers such as NLR and PLR using the results obtained from complete blood count may reflect systemic inflammation and may even be prognostic indicators in some vasculitis [10,11,12]. Several studies have reported that NLR is a potential predictive marker of gastrointestinal bleeding in children with IgA vasculitis [23, 24]. The use of indices to predict renal involvement in IgA vasculitis has proven to be effective and it has even been emphasized that several indices can be appropriately combined to improve diagnostic efficiency [10,11,12]. It was found that these two markers may predict intravenous immunoglobulin resistance in Kawasaki disease. On the other hand, Liu et al. reported that these two markers were inadequate in Kawasaki disease [25]. Because of these contradictory results, the search for more useful markers such as CAR rate is ongoing in many diseases including vasculitis [26,27,28]. CRP, an acute phase protein, increases with systemic inflammation in vasculitis. Moreover, an expected decrease develops in albumin, which is considered a negative acute phase reactant. Changes in these two parameters result in a significant increase in the CAR. As a result, it is quite logical that CAR is more important than NLR and PLR. In our study, we investigated the predictability of CAR for scrotal involvement in patients with IgA vasculitis; and CAR > 0.0825 had 67.6% sensitivity, and 53% specificity after ROC analysis. However, in multivariate logistic regression analysis, CAR was not an independent predictor of scrotal involvement. Larger-scale studies are required for CAR for predicting important organ involvement.
The main approaches in the management of IgA vasculitis include supportive therapies such as hydration, bed rest and symptom relief [29]. Corticosteroids, azathioprine, cyclophosphamide and plasmapheresis are used in major organ or system involvement such as GI tract, renal or central nervous system [7, 18]. The severity of the disease, the affected organ or system and the presence or absence of life-threatening vasculitis determine the intensity of treatment. Ma et al. reviewed case reports published over a 35-year period and presented the treatment approach for 21 patients with IgA vasculitis with scrotal involvement. They reported that 16 patients received conservative treatment and steroids, 5 patients received only conservative treatment and 2 patients underwent surgical intervention. All patients had a good prognosis [18]. Treatment approaches for scrotal involvement vary from conservative to immunosuppressive therapy, and individualization of treatment is important. On the other hand, there are strong recommendations in support of steroid use. The European consensus-based recommendations for the diagnosis and treatment of IgA vasculitis in children-SHARE initiative recommend the use of steroids in orchitis [7]. In fact, steroid use has been reported in 93% of children with IgA vasculitis with scrotal involvement [5]. Ben-Chaim et al. reported relief of scrotal symptoms immediately after initiating steroid therapy [30]. In our center, patients with scrotal involvement were treated with a combination of conservative therapies and steroids.
The main limitations of this study are its retrospective design and single center. Due to the retrospective design of the study and the exclusion of patients with less than six months of follow-up and missing data, our results may reflect the findings of more severe or better documented cases. Prospective, multicenter studies may provide more accurate and generalizable results about the scrotal involvement of IgA vasculitis. In addition, the frequency of scrotal involvement in IgA vasculitis could not be given accurately since all patients did not have the same follow-up time. The lack of data on the use of PVAS in vasculitis is another limitation. On the other hand, the presentation of data on the use of PVAS in patients with scrotal involvement in IgA vasculitis is also a strength of this study. It is clear that there is a need for tools to measure the outcomes of vasculitis and in this present study, a cut off value was proposed for the predictive value of PVAS for scrotal involvement.
In conclusion, scrotal involvement may develop in IgA vasculitis and most patients are treated with steroids in addition to conservative therapies. Widespread purpura, local edema, penile involvement and hematuria are more common in patients with scrotal involvement than those without. PVAS and some systemic inflammatory markers may be helpful in predicting scrotal involvement.



Comments (0)