
Remember me

This is a single-centre randomised controlled trial, coordinated and implemented at Faculdade de Medicina, Universidade de Lisboa (FMUL), Gulbenkian Institute for Molecular Medicine (GIMM) and Unidade Local de Saúde (ULS) Santa Maria, Centro Académico de Medicina de Lisboa (CAML), Lisbon, Portugal. This trial is registered in ClinicalTrials.gov (NCT06758817; date of registry: January 6th 2025). This trial was approved by the ethics committee of CAML (Ref. Nº114/22).
We aim to investigate whether a nutritional intervention based on a MedDiet enriched with fermented foods (MedDiet +) may influence disease activity, functional status, quality of life, intestinal permeability, endotoxemia, inflammatory biomarkers, intestinal and oral microbiota, serum proteomics and serum glycome.
The first participant was enrolled in July 2023, and data collection is anticipated to conclude by the end of 2025. Currently, the effect of the MedDiet on the Disease Activity Score in 28 joints (DAS28) of RA patients is not yet known, making it unfeasible to conduct a formal sample size calculation. Considering the number of potentially eligible RA patients treated at the Rheumatology Department at ULS Santa Maria, our recruitment capacity, available funding, and the size of recent published studies in this area, a convenience sample of 100 participants will be recruited.
Patients meeting eligibility criteria are randomly assigned to the intervention MedDiet + (n = 50) or control (n = 50) groups through an online block randomisation generator. Due to the nature of the trial, the participants and the registered dietitians responsible for implementing the study are not blinded. However, the clinicians evaluating the clinical outcome measures and the researchers performing the laboratory tests are blinded.
Primary endpointSecondary endpointsProportion of patients achieving:
Change in DAS28-CRP (Disease Activity Score in 28 joints calculated with C-reactive protein)
Change on ultrasound score (32 joints scored 0-3 for grey scale and power Doppler)
Proportion of patients who had a 10% improvement in ultrasound score
Change in Short Form 36 Health Survey Questionnaire (SF36) results
Change in Health Assessment Questionnaire (HAQ) results
Changes in α- and β- diversity of the gut and oral microbiota
Changes in the relative abundance of Lactobacillus/Limosilactobacillus and Bifidobacterium species in the gut
Changes in butyrate-producing species in the gut microbiota
Changes in H2S-producing species in the gut microbiota
Change in the lactulose/mannitol ratio
Change in Endotoxemia measured by TLR4 activation in reporter cells
Change in inflammatory biomarkers (C-Reactive Protein, CPR; Erythrocyte sedimentation rate, ESR, faecal calprotectin)
Change in serum soluble CD14 (CD14s), lipopolysaccharide-binding protein (LBP), and intestinal fatty acid binding protein levels (IFABP)
Change in lipid profile (Triglycerides, Total Cholesterol, HDL and LDL Cholesterol)
Change in body composition (Fat Mass, Fat-Free Mass, Total Body Water and Body Cell Mass)
Change in anthropometric measurements (body mass index, BMI, and waist circumference)
We will also analyse zonulin levels, serum proteomics, and serum glycomics.
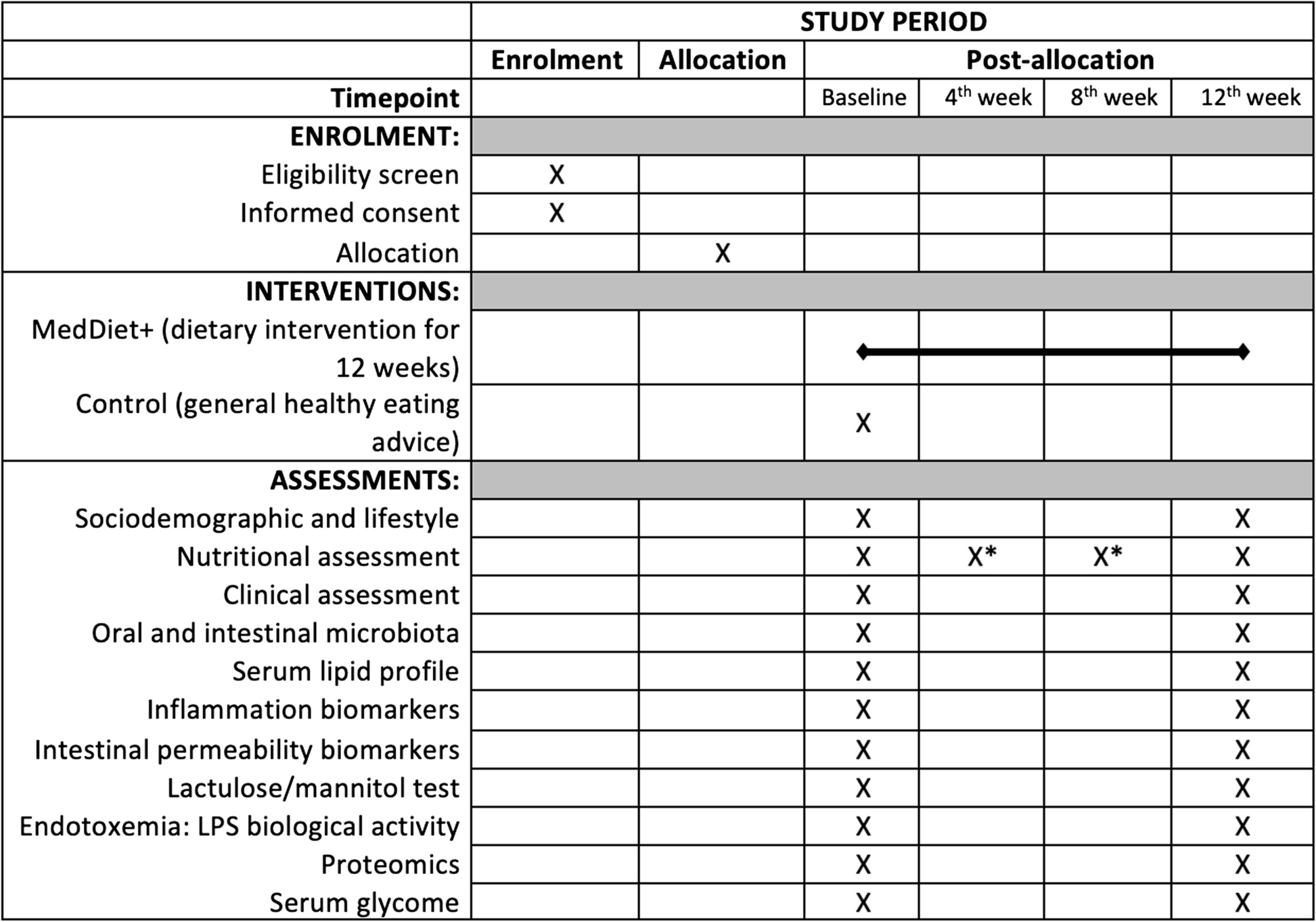
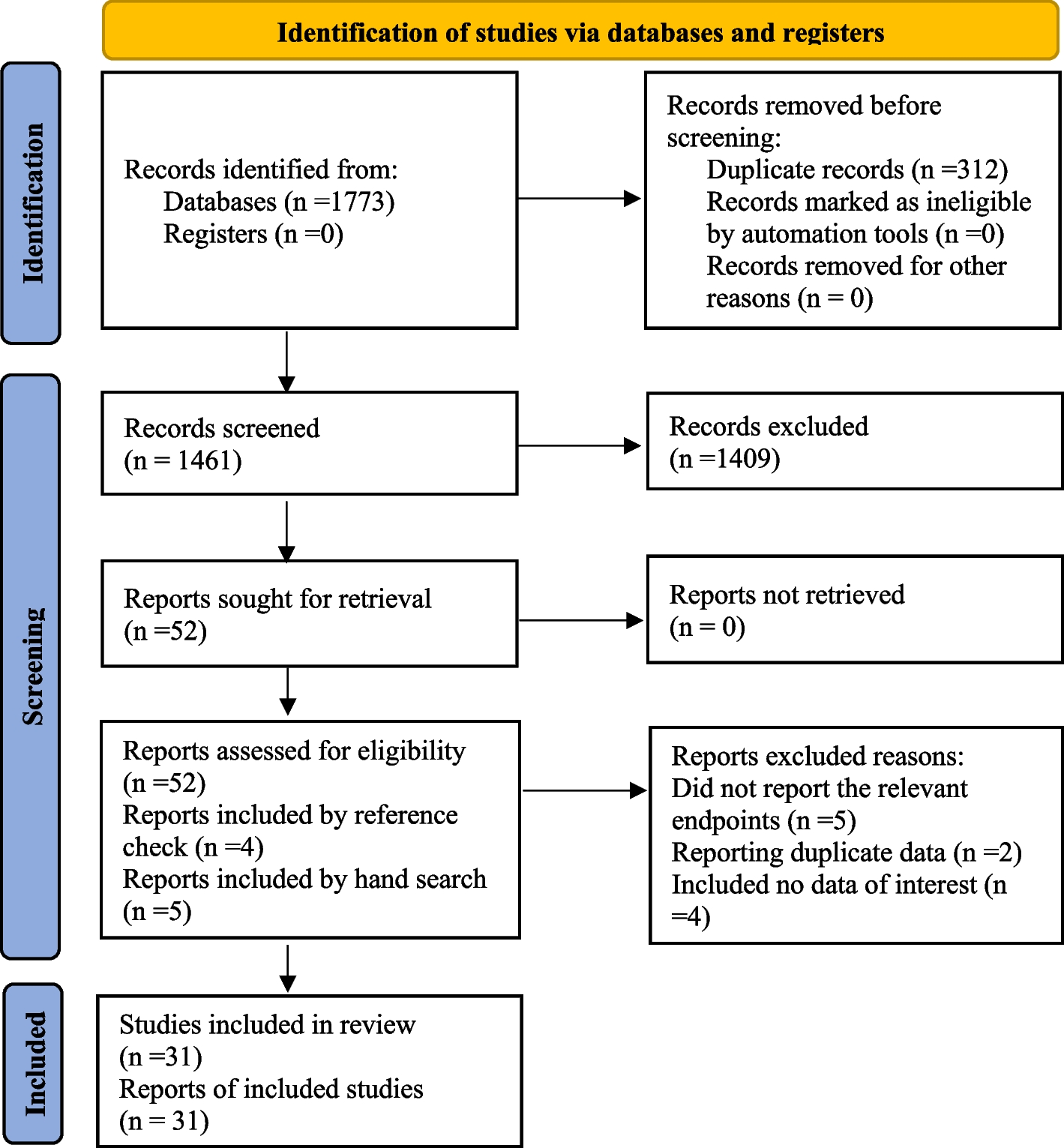
Recruitment and eligibility criteriaRA patients diagnosed according to the ACR/EULAR2010 criteria [23], aged 18 years old or older, are invited to participate in this study if eligibility criteria are met at their regular follow-up RA consultations. All participants sign a written informed consent form before any study procedures. Our inclusion criteria are diagnosis duration of at least one year, active disease (DAS28-ESR ≥ 2.6 units), stable medication for at least 12 weeks prior to the baseline assessment (including intra-articular steroid injections), and a low or medium adherence to the MedDiet (defined as a score of < 10 points in the 14-item tool by the PREvención com DIeta MEDiterránea trial, PREDIMED). Patients requiring therapeutic adjustments and/or intra-articular steroid injections during the trial are excluded. Our exclusion criteria are: antibiotic therapy within 4 weeks before enrolment; prednisolone dose > 7.5 mg/day; persistent use of non-steroidal anti-inflammatory drugs: diagnosis of inflammatory or irritable bowel disease, celiac disease, chronic diarrhoea; diagnosis of other immune-mediated or inflammatory diseases; major organ dysfunction; cancer diagnosed in the last five years; presence of health conditions which may impair the ability to consent to study participation (cognitive impairment/psychiatric disease). Regarding the use of antibiotics, although a general recommendation for a washout period is challenging to define, according to literature, a minimum of 4 weeks since cessation of antibiotics is recommended [24] and is considered in this trial. The overall diagram flow of the study is shown in the SPIRIT figure illustrated in Fig. 1. The SPIRIT checklist is provided as supplementary material.
Fig. 1
SPIRIT figure with standard protocol items of the TASTY trial. The SPRIT figure illustrates key components of the TASTY trial protocol and data collection time points from enrolment to the end of the 12 weeks. Abbreviations: Lipopolysaccharides (LPS). *Only in the MedDiet + Group
Interventions and comparatorsMedDiet + groupThe intervention is carried out for 12 weeks at ULS Santa Maria and includes an educational-based nutritional intervention with a structured nutrition plan prescribed by registered dietitians, educational food baskets, educational digital content, and clinical culinary workshops.
At baseline, a personalised nutritional plan is elaborated for each participant, and its implementation is closely monitored through weekly follow-up calls and monthly face-to-face appointments to fully involve participants and minimise dropout rates. To define an adjusted nutritional plan, nutritional requirements are individually assessed considering the patients' nutritional status and physical activity level. Energy, as well as protein, carbohydrate, and lipid requirements are calculated in agreement with the European Food Safety Authority (EFSA) dietary reference values [25]. The nutritional plan includes the number of food portions of each food group that participants must consume, in agreement with the MedDiet recommendations for the adult population [26]. To complement the traditional MedDiet, additional advice is provided to promote the consumption of specific fermented foods that potentially contain probiotic microorganisms, vitamins and bioactive compounds, such as fermented beverages, including kefir (provided for daily consumption) and kombucha (provided for consumption 2x/week). Foods with anti-inflammatory properties are also recommended, including sources of n-3 polyunsaturated fatty acids (PUFAs), such as oily fish, nuts and seeds, and a high amount of extra-virgin olive oil. The intake of vitamins, carotenoids, and phenolic compounds is promoted by the consumption of a wide variety of fruits, vegetables, legumes, whole grains, nuts and seeds, tea and infusions, herbs and spices, and extra-virgin olive oil. The nutritional plan can be adjusted if patients report issues with the consumption of specific foods.
Educational food baskets are delivered weekly with different typical ingredients of the MedDiet + pattern to encourage their inclusion in the patients' daily meals. This strategy ensures that every participant receives the same resources to meet the nutritional recommendations. We have secured a partnership agreement with a supermarket chain to overtake logistic aspects. Ingredients such as extra virgin olive oil, whole grains (whole grain bread, rice and pasta, oats), fresh fruits and vegetables, legumes, nuts and seeds, canned sardines and mackerels, herbs and spices, plain yoghurt, kefir, and kombucha are being provided.
Educational content consists of video recordings and two recipe books to share new ideas for cooking recipes, as well as educational and useful content to help participants meet the nutritional recommendations. It intends to empower patients with knowledge of different dishes and cooking methods to promote the inclusion of the foods provided in the food baskets. Recipes for other fermented foods, such as sauerkraut and sourdough bread are also included in the educational content. Finally, access to an online clinical culinary workshop is provided. The clinical culinary workshop allows for the application of the provided nutritional knowledge into culinary preparations through the demonstration of recipes and culinary methods.
Control groupAt baseline, the control group receives a flyer with general recommendations on a healthy diet, based on the Portuguese brief guidance for healthy eating in primary health care [27]. No food baskets or any of the nutritional education strategies are implemented. To promote study adherence, a shopping voucher is given to each participant at the end of the trial. This comparator was chosen to reflect the standard care that could be given by clinicians.
Data collectionSociodemographic and lifestyle dataThe participants' relevant clinical history is collected from their electronic hospital records (disease duration, current medication, and comorbidities). A structured questionnaire was developed to collect patients' age, sex, educational level, menopausal status, smoking status, and family history of rheumatic diseases.
Nutritional assessmentNutritional assessment encompasses four components: nutritional intake, dietary pattern characterisation, body composition analysis, and anthropometric measurements. Nutritional intake is assessed by a 24-h dietary recall (24 h Recall), one of the most widely used tools in nutrition surveys to obtain detailed information about all food and beverages consumed in the past 24 h. A quantitative assessment with portion size quantification is included to provide a more comprehensive and detailed report. Adherence to the MedDiet is assessed with the Portuguese version [28] of the 14-Item Mediterranean Diet Assessment Tool developed by PREDIMED study authors [29, 30], in which a maximum score of 14 points can be achieved, being a strong adherence defined by a score ≥ 10 points. Anthropometric measurements (height, weight, and waist circumference) are performed by registered dietitians. BMI is calculated as weight/height squared (kg/m2) and bioelectrical impedance analysis (BIA) is performed to analyse body composition (Fat Mass, Fat-Free Mass, Total Body Water and Body Cell Mass). Nutritional assessment is performed at baseline and at the end of the trial for both groups and every month (baseline, 4th, 8th and 12th weeks) for the intervention group.
Clinical outcome measuresThe DAS28-ESR and articular ultrasound examination of 28 joints are performed to assess disease activity. The DAS28 is the most widely used scoring system to determine disease activity in patients with RA [31, 32] considering the following items: number of tender and swollen joints in 28 joints (shoulders, elbows, wrists, metacarpophalangeal joints, hand proximal interphalangeal joints and knees); ESR (mm/hr), and a patient global health assessment based on a visual analogue scale (VAS-GH, range, 0–100). The DAS28-CRP is also being assessed as a secondary outcome measure. It encompasses the same items as the DAS28-ESR but substitutes the ESR with CRP in the formula.
Articular ultrasound examination is performed using a GE Logiq E9 equipment with a 6–15 MHz matrix linear probe. Doppler ultrasound (DUS) is used to assess the vascularisation of the synovial tissue. Ultrasound procedures and grey scale ultrasound (GSUS) and DUS grading are based on EULAR-OMERACT consensus [33,34,35]. The Doppler parameters are adjusted at the maximum sensitivity for slow flow (pulse repetition frequency of 0.4 kHz, lowest wall filter on 45 Hz, and 7.5 MHz Doppler frequency) with Doppler gain just below the noise level. In all patients, the wrists, metacarpophalangeal joints, and proximal interphalangeal joints are examined with ultrasound. Examinations are performed using a standardised dorsal and dorso-lateral scans. Erosions are also evaluated by GSUS as defined by the OMERACT consensus [36] and a semiquantitative score is used to evaluate ultrasound detected erosions [37].
As for patient-reported outcomes, functional status and quality of life are evaluated using the HAQ [38] and SF-36 short form [39] questionnaires, respectively. The HAQ assesses functional status through a disability index, and patient global and pain visual analogue scales [38]. The SF-36 includes a multi-item scale that assesses various health concepts such as limitations in physical activities related to health problems, limitations in social activities related to physical/emotional problems, limitations in day-to-day activities due to physical health problems, pain, mental health, limitations in the day-to-day activities because of emotional problems, vitality, and general health perceptions [39]. Clinical assessments are performed at baseline and after 12 weeks in both groups.
Oral and Intestinal MicrobiotaSaliva samples are collected with a saliva collection kit while the faeces are self-collected by the participants with the OMNIgene GUT kit. Samples are processed according to the standard operating procedure, which defines biological samples' handling, processing, and freezing protocols to be preserved at the Biobank-GIMM, CAML.
For cell lysis, three bead beating cycles, in a total of 3 min of bead beating are included. We use the Ruptor Elite (OMNI International) with the following conditions: 1 min on at 6 m/s followed by 5 min rest. The bacterial DNA is extracted with the QIAamp PowerFecal Pro DNA Kit (Qiagen). Shotgun metagenomics sequencing will be performed, generating > 3 million reads per sample. The sequencing data resulting from the feces samples will be processed using the bioinformatics pipeline from the Microbiome in Health and Disease Translational Laboratory (GIMM), which includes quality filtering to remove low-quality reads and sequencing artefacts, removal of host DNA reads by mapping to the human genome (GRCh38), and elimination of optical duplicates. To perform taxonomic classification, a combination of k-mer and mapping approaches to a custom-developed reference database will be used, which includes a curated collection of bacterial and fungal genomes from publicly available databases (GTDB, UHGG). Similarly, for functional classification, a combination of k-mer and mapping approaches to publicly available functional databases such as Uniprot, KEGG, CAZy, and others will be used.
Lipid profile, inflammation and intestinal permeability biomarkersBlood tests are performed to determine the serum levels of the lipid profile biomarkers (Triglycerides, Total Cholesterol, HDL and LDL Cholesterol) by standard operating procedures, as well as the serum levels of inflammatory and disease activity biomarkers (CRP and ESR). Although this study protocol encompasses the DAS28-ESR as a primary outcome, the serum CRP levels are also evaluated due to its high sensitivity for evaluating short-term inflammation [40]. Faecal calprotectin, an established marker of gut inflammation, is being analysed by a particle-enhanced turbidimetric immunoassay (CALiaGold© test).
Serum IFABP, lipopolysaccharide-binding protein (LBP) and sCD14 will be evaluated by Enzyme-Linked Immunosorbent Assay (ELISA), once data collection is completed. IFABP actively participates in dietary lipid metabolism by mediating fat absorption through binding and intracellular trafficking of free long-chain fatty acids [41]. Increased serum levels of IFABP, which is also a specific biomarker of gut epithelial integrity, have been shown in RA patients [42]. LBP, an acute-phase protein that carries the ability to bind to LPS [43], has been recognised as a sensitive serum biomarker for RA disease activity, as it significantly correlated with ESR, CRP, tender joint counts, swollen joint counts and DAS28 [44]. CD14s is also an acute phase protein whose hepatic production is increased in response to interleukin (IL)−6 in the setting of inflammation. CD14 stimulates the production of other pro-inflammatory cytokines, including IL-6, in an amplification loop that participates in RA pathogenesis [45]. Furthermore, CD14s has been shown to be increased in RA patients and correlate with DAS28 score and response to treatment [46]. These biomarkers, IFABP (serum diluted 1:4), LBP (serum diluted 1:500), and CD14s (serum diluted 1:15), will be measured from patient serum by sandwich ELISA (LBP cat. DY870; FABP2 cat. DY3078; CD14 cat. DY883; R&D Systems, USA), following the manufacturer instructions. Horseradish peroxidase conjugate will be detected with enhanced chemiluminescence substrate (cat. 32,106, Pierce, USA) and measured with a microplate reader (BMG Pherastar FS, BMG LABTECH, Germany).
Zonulin, a strong modulator of intestinal intercellular tight junctions, is recognised to play a role in the translocation of macromolecules and, consequently, in the tolerance/immune response balance [47]. Higher serum zonulin levels were shown to be accompanied by increased intestinal permeability and, in turn, the disruption of the intestinal barrier function has been proven to occur before the onset of the inflammatory phase of murine and human arthritis [48]. Zonulin (serum diluted 1:10) will be measured from patient serum by sandwich enzyme-linked immunosorbent assay (ELISA) (cat. E-EL-H5560, Elabscience, USA), according to the manufacturer instructions. Optical density will be measured with the microplate reader (BMG Pherastar FS, BMG LABTECH, Germany) set to read the absorbance at 450 nm with a wavelength correction set at 540 nm.
All ELISA assays will be performed in High-Throughput Screening (HTS) mode with reagent and liquid dispensing by the dispenser (CERTUS FLEX Fritz Gyger AG, Germany), serum sample dispensing by dispenser (ECHO 650, Labcyte, US) or manually, and washes by plater washer (EL406, Agilent BioTek, USA). These assays will be performed at the Finnish Institute for Molecular Medicine Finland (FIMM) High Throughput Biomedicine unit.
Intestinal permeability: lactulose/mannitol testIntestinal Permeability is assessed through the lactulose/mannitol (Lac/Man) test, a gold standard for functional measurement of intestinal permeability in humans. Specific dietary recommendations for the 24 h before the test are provided to standardise conditions across participants and reduce variability in results. Although there is no consensus for dietary restrictions in this test, patients are advised to avoid some foods and beverages potentially containing lactulose and/or mannitol [49,50,51], such as dairy products, sweet potato, mushrooms, cauliflower, butternut squash, celery, peas, green beans, chicory, fennel, kimchi, sauerkraut, peach, watermelon, gelatin, gummies, candies, chewing gum, sauces, ‘diet’ and ‘light’ food products, artificial sweeteners, dietary supplements, soft drinks, and flavoured and alcoholic beverages.
After an overnight fast (≥ 8 h), patients are given a solution containing 5 g of lactulose and 1 g of mannitol and are encouraged to drink 1.5 L of water for 4 h and collect all the urine produced during that time. Lactulose and mannitol concentrations are determined by ultra-performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS). The lactulose and mannitol quantification is performed at Instituto Nacional de Saúde Dr. Ricardo Jorge in Lisbon, Portugal. UPLC-MS/MS and mass spectrometer conditions are further detailed in the supplementary material.
Endotoxemia: LPS biological activityToll-like receptor 4 (TLR 4) activation reflecting LPS bioactivity will be measured, when recruitment has finished and all samples have been collected, with HEK-Blue hTLR4 reporter cells (InvivoGen) engineered to produce secreted alkaline phosphatase in response to TLR4 stimulation. The method has been established and validated for cell-based High Throughput Screening, making it appropriate for population cohort sample screening [52]. Briefly, 70,000 cells/well will be seeded on a 384-well plate with 25 μl of cell culture media. Serum samples (2.5ul) will be added in duplicates to wells to obtain a final working concentration of 1% (v/v) per well. To determine whether TLR4 activation is due to LPS, we will add another set of sample duplicates with 0.1 mg/ml of polymyxin B (InvivoGen), an LPS inhibitor. Human AB serum 1% (v/v, Sigma-Aldrich) will serve as a negative control. A set of standard dilutions will be created with LPS-B5 Ultrapure from Eschericia coli O55:B5 (InvivoGen) diluted in endotoxin-free water with 1% Human AB serum. After incubation at 37° C for 24 h, we will add 10ul/well SEAP substrate QUANTI-BlueTM Solution (InvivoGen). Following a 6 h incubation at 37 °C, absorbance will be measured with a microplate reader (BMG Pherastar FS, BMG LABTECH, Germany). TLR4 activation due to LPS will be then determined by subtracting the activity remaining in the presence of polymyxin B from the total TLR4 activation measured. A linear standard curve will be plotted. The LPS biological activity will be performed at the Helsinki University (Finland).
ProteomicsNowadays, various proteomic techniques are being applied to different biological samples, from both RA patients and experimental animal models, showing promise in identifying novel biomarkers and treatment targets [53]. In our trial, once all samples have been collected, blood serum samples will be studied through micro-liquid chromatography-mass spectrometry (micro-LC–MS/MS) using a hybrid quadrupole TripleTOF 6600 (Sciex, CA, USA). The proteomes will be identified through the qualitative shotgun data-dependent acquisition (DDA) method [54, 55], and protein levels will be measured through the quantitative sequential window acquisition of all theoretical mass spectra (SWATH) methods. A 5% false discovery rate (FDR) and a p-value ≤ 0.05 will be used to filter the dataset. FunRich software 3.1.3 will be used to determine proteome enrichment.
Serum Glycome characterisationWhen patient recruitment has been concluded, serum will be processed and ultra high performance liquid chromatography (UHPLC) analysis will be performed using hydrophilic interaction liquid chromatography (HILIC) chromatography coupled with fluorescence detection and online electrospray MS for total serum glycome characterisation. From this analysis we will be able to identify unique signatures related with plasma proteins N-glycans alterations that can be associated with dietary intervention. Then, and given the fact that Fc glycosylation of IgG/IgA is a key factor for the definition of effector (inflammatory) function of IgG/IgA, we will characterise the antibody specific Fc glycosylation of IgG/IgA at the different time points before and after dietary intervention, by advanced glycoproteomics nano-liquid chromatography-electrospray ionization-tandem mass spectrometry (nanoLC-ESI–MS). The structural characterisation of the IgG Fc-N-glycans in terms of composition and abundance will be performed by advanced liquid chromatography coupled to mass spectrometry), that enables high-throughput analysis of IgG Fc-glycans in a subclass-specific manner.
Figure 2 resumes all variables collected during the study timeframe.
Fig. 2
– Overview of the data collection throughout the trial. Visual representation of the specific variables to be collected in each phase of the study, which are identical at baseline and at the end of the trial (12th week) for both groups. Only the intervention group (MedDiet +) has in-person follow-up consultations with nutritional assessment at 4th and 8th weeks. *Sociodemographic and lifestyle data are also collected at baseline. Abbreviations: CRP: C-reactive protein; DAS28: Disease Activity Score using 28 joint counts; ESR: Erythrocyte sedimentation rate; HAQ: Health Assessment Questionnaire; I-FABP: Intestinal-fatty acid binding protein; LPS: Lipopolysaccharides; PREDIMED: Prevención con Dieta Mediterránea; SF36: 36-Item Short Form Health Survey
Data management and statistical analysisCollected data files in paper format are being securely stored in locked filing cabinets within the Nutrition Lab, FMUL, CAML, accessible only to authorized team members. All recorded data and collected samples are coded, and analysis will be performed anonymously. Only members of the research team will have access to data and samples. FMUL has the property of the resulting data and the right to disclose the results as merged data analysis. The Nutrition Lab of FMUL will have access to the final trial dataset and will be responsible for storing conserved data for five years after the last publication.
Statistical analysis will be conducted using SPSS (SPSS® Inc., Chicago, IL) version 28.0 or a subsequent updated version. The Normal data distribution will be verified using the Kolmogorov–Smirnov tests, considering the sample size. Depending on the normality of the data, parametric or non-parametric tests will be used. A p-value of less than 0.05 will be considered statistically significant. Descriptive statistics will be used to describe all variables, both by groups (intervention vs. control) and by timing (baseline and final visits). Characteristics between groups at baseline will be compared to identify significant differences that may confound results. To access differences between the baseline and the end of the intervention (paired sample test) as well as between groups (independent samples test), the student's T-Test or its non-parametric equivalent will be used. Multiple regression analysis will be conducted to address the influence of baseline characteristics. An analysis of covariance (ANCOVA) will be carried out when baseline differences need to be controlled, being the group (intervention/control) the independent variable, and the covariates the baseline characteristics and demographic data. To test how the MedDiet + pattern influences the study endpoints, a multivariate analysis of covariance (MANCOVA) will be conducted to assess group differences with multiple dependent variables and adjusting for confounding factors. The existence of a control group allows for statistical comparisons between groups and ensures the true effectiveness of the MedDiet + when adjusting for potential confounders.
Comments (0)