Prediabetes refers to a state where blood glucose levels are higher than usual but have not yet reached the diagnostic threshold for diabetes. It is a high-risk stage for developing diabetes and is also considered the only reversible “golden period” [1, 2]. According to the International Diabetes Federation (IDF) 2019 report, approximately 374 million people worldwide have prediabetes, accounting for 7.5% of the adult population [3]. This number is projected to rise to 548 million, or 8.6%, by 20453. Without timely management, about 5–10% of individuals with prediabetes will progress to type 2 diabetes (T2D) each year, and approximately 70% will eventually develop T2D [3, 4]. The high prevalence and conversion rates of prediabetes present a significant burden on public health and healthcare expenditure [5]. Therefore, timely intervention and effective management strategies for prediabetes are crucial for preventing the onset of diabetes and its complications.
Lifestyle changes, particularly increasing physical activity levels, are more effective than medication alone in reversing prediabetes and preventing its progression to diabetes [6]. However, such interventions face many obstacles in real-world settings. Many patients struggle to adhere to regular moderate-intensity aerobic exercises (such as jogging or brisk walking) due to sedentary habits, physical limitations, and other factors [7,8,9]. For patients unable to follow lifestyle recommendations, pharmacological and dietary therapy provide an alternative option. However, while plant-based dietary therapies, such as okra consumption, may improve fasting blood glucose (FBG), their effects on longer-term indicators, such as glycated hemoglobin (HbA1c) [14], remain limited. Similarly, the long-term use of pharmacological treatments is constrained by such problems as adverse side effects [10], diminished efficacy upon discontinuation [11], weight regain [12], and recurrence of prediabetes [13], rendering these treatments less appropriate as sustainable strategies for long-term management of prediabetes. These limitations underscore the urgent need for more effective and sustainable approaches to address the multifaceted challenges of prediabetes management.
Under the “Exercise is Medicine” (EIM) concept, TCEs such as Tai Chi, Baduanjin, and Yijinjing have been widely adopted globally as effective disease prevention and management tools [15]. These practices, rooted in traditional Chinese medicine, are characterized by their low intensity, non-competitive nature, and high adherence. They emphasize the combination of breathwork, meditation, and physical movement, making them particularly suitable for middle-aged and elderly individuals with prediabetes, especially those with a weakened constitution [16]. In addition, TCEs are easy to learn, represent low-risk interventions with favorable outcomes, and do not require professional guidance or expensive resources, thus reducing implementation difficulty [17, 18]. This makes TCEs a more feasible and cost-effective intervention, especially in resource-limited communities or healthcare systems.
In recent years, TCEs have demonstrated significant potential in preventing and managing prediabetes, becoming an effective lifestyle intervention strategy. A previous meta-analysis [19] has only proven that TCEs positively affect blood glucose control in individuals with prediabetes. However, systematic assessments regarding the impact of exercise dosage on blood glucose and lipid profiles still need to be done. Moreover, prediabetes is often associated with metabolic disturbances, such as dyslipidemia, in addition to abnormal glucose metabolism. This may increase the risk of progression to T2D and cardiovascular diseases [20]. Although current guidelines emphasize enhanced lipid management for diabetes patients, there are few specific recommendations for addressing dyslipidemia in individuals with prediabetes [21]. Therefore, this meta-analysis aims to (1) comprehensively assess the effectiveness of TCEs in controlling blood glucose and lipid levels in individuals with prediabetes, (2) explore the optimal exercise prescription to improve glucose and lipid metabolism in prediabetes patients.
Protocol and registration
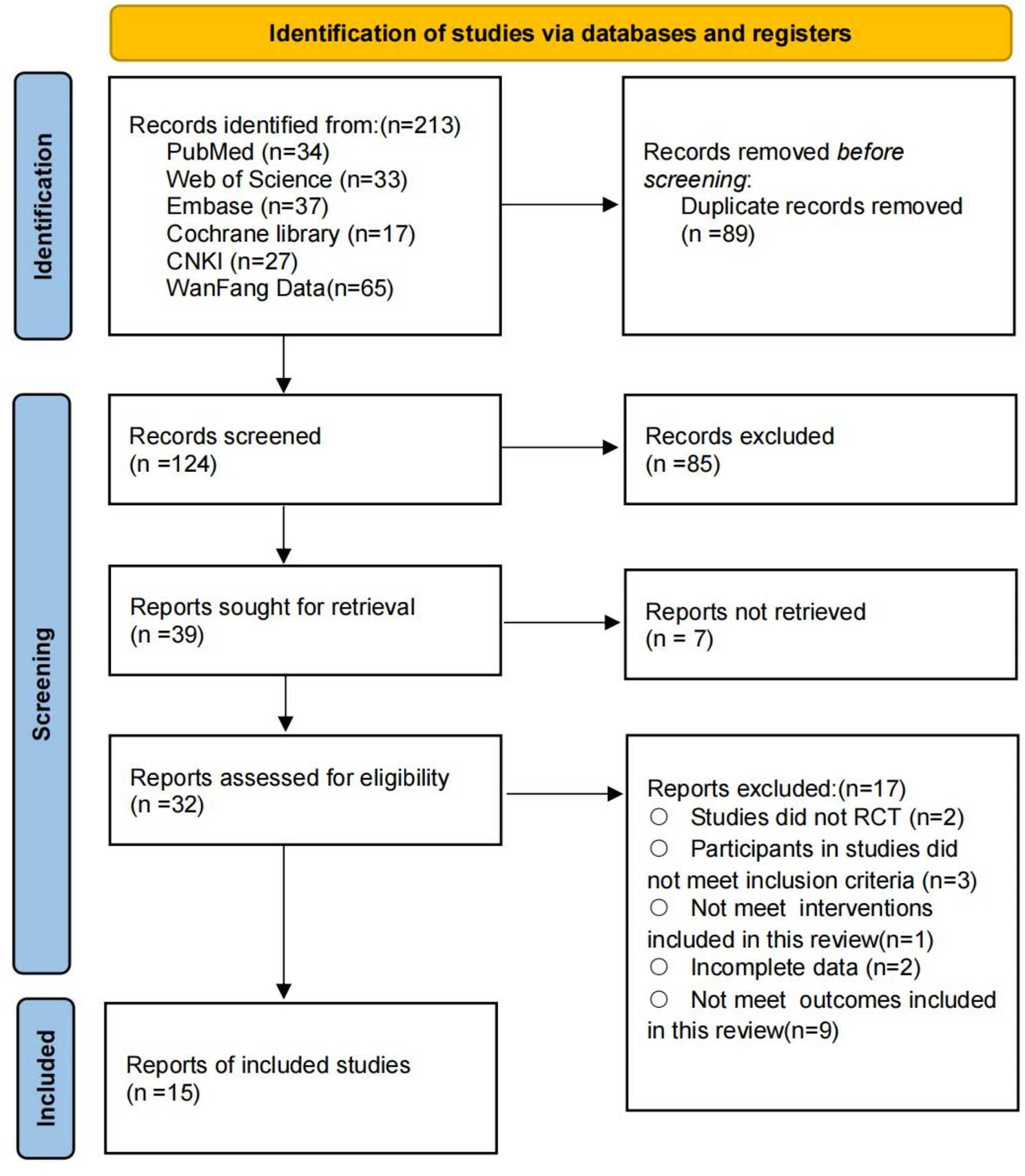
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22] conducted this systematic review and meta-analysis. The protocol for this systematic review and meta-analysis has been registered in PROSPERO (CRD42024615150).
Search strategy and study selection
We conducted a comprehensive literature search in six databases: PubMed, Web of Science, Cochrane Library, Embase, CNKI, and WangFang Data, to identify randomized controlled trials (RCTs) on the effects of TCEs on individuals with prediabetes. The search was conducted from establishing each database until November 10, 2024. Three independent reviewers (RX, LD, and BW) performed the search and screened the eligible studies, with any disagreements resolved through consultation with a fourth reviewer (GS). Additionally, the reference lists of the included studies and relevant systematic reviews were checked for further potential eligible trials. A complete list of the search strategies can be found in Appendix 1.
Eligibility criteria
The studies were evaluated using the PICOS framework (Population, Intervention, Comparison, Outcome, and Study Design) [23]. Studies were included in the review if they met al.l of the following criteria:
Population
This study included research recruiting participants aged ≥ 18 years with prediabetes, excluding those with diagnosed diabetes, severe comorbidities, children, adolescents, and pregnant women. The diagnosis of prediabetes was based on the American Diabetes Association (ADA) criteria [24], which include any of the following conditions: fasting blood glucose levels between 5.6 and 6.9 mmol/L; HbA1c levels between 39 and 47 mmol/mol (5.7-6.4%); or a 2-hour plasma glucose level between 7.8 and 11.0 mmol/L in an oral glucose tolerance test (OGTT) (Table 1).
Table 1 Diagnostic criteria for prediabetesIntervention
The interventions included TCEs such as Tai Chi, Yijinjing, Baduanjin, and Shaolin Neigong, with detailed definitions of TCEs provided in Appendix 2.
Comparator
The control groups included health education, routine care, and waiting lists.
Outcome
The included studies were required to report at least one of the following outcomes:
Blood glucose control: HbA1c, FBG, postprandial 2-hour blood glucose (2hPG);
Blood lipid control: Total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL).
Study design
The study design was restricted to RCTs.
Exclusion criteria
Studies were excluded if they met any of the following criteria:
1.
Non-randomized controlled trials.
2.
Interventions involving pharmacological treatments or dietary control.
3.
Studies that were not peer-reviewed, including theses, research protocols, conference abstracts, and other forms of gray literature.
4.
Studies that did not provide appropriate data for analysis.
5.
Studies whose full text could not be obtained through public databases or other sources.
Data extraction
We independently extracted the following information from each eligible study using a pre-designed data extraction form: study characteristics (first author, publication year), population characteristics (age, gender, sample size), intervention characteristics (type, duration, frequency, cycles), and outcome measures. If data were missing, we emailed the corresponding author up to three times within 3 weeks to obtain the relevant data. Two reviewers (GS and BW) performed data extraction independently, verified and adjudicated by a third reviewer (LD). Any disagreements were resolved through discussion and consensus.
Measures of treatment effect
This meta-analysis assessed the intervention effect using the Mean Difference (MD) and its standard deviation (SD) change. If the original studies did not directly report the SD, we estimated it based on standard error (SE), 95% confidence interval (95%CI), p-value, or t-statistics [25]. For studies that did not report the SD of pre-post changes, the following formula was used to estimate it:
$$\:_=\sqrt_^+_^-2\times\:r\times\:_\times\:_}$$
The SD of the differences before and after the intervention was calculated, assuming a correlation coefficient of 0.5. This assumption, widely used in the literature, represents moderate measurement consistency, aiming to balance potential variability before and after the intervention and ensure the robustness and reliability of the analysis results [25].
Quality and GRADING of evidence assessment
The risk of bias was assessed using the Cochrane Risk of Bias tool (version 2.0), covering domains such as random sequence generation, allocation concealment, blinding, incomplete outcome data, and selective reporting of outcomes [26]. The overall risk of bias for each study was categorized as follows: Low risk of bias: All domains assessed as low risk; High risk of bias: At least one domain evaluated as high risk; Some concerns: If the study did not meet the above standards. Two independent reviewers performed the risk of bias assessment, and any disagreements were resolved through consultation and consensus.
The quality of the evidence was evaluated using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach, completed through the GRADEpro GDT online tool (www.gradepro.org). According to the GRADE framework, evidence quality was systematically assessed based on five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. The quality of evidence for each outcome was classified as “high,” “moderate,” “low,” or “very low,” based on a comprehensive evaluation of the credibility of effect estimates [27]. Independent reviewers carried out all assessments, with disagreements resolved through discussion.
Statistical analysis
A meta-analysis was performed when two or more relatively homogeneous studies reported the same outcome measure [28]. The intervention effect was assessed using the MD and its 95% CI. The MD was calculated as the change in the intervention group before and after the intervention relative to the change in the control group and standardized based on the SD after the intervention to improve comparability between studies. To address possible variations between studies, a random-effects model was utilized, incorporating variations in study populations, interventions, and measurement methods [29]. Heterogeneity was assessed using the I² statistic and interpreted as follows: <25% indicating low heterogeneity, 25–75% indicating moderate heterogeneity, and > 75% indicating high heterogeneity [30]. Publication bias was evaluated using funnel plots and Egger’s test, with p < 0.05 considered indicative of significant bias [31]. When publication bias was detected, the trim and fill method was applied to adjust the pooled effect size and estimate the impact of missing studies [32].
To explore potential factors contributing to heterogeneity, we conducted subgroup analyses and evaluated the effects of different doses of TCEs on individuals with prediabetes. The subgroup analyses were based on the following pre-defined variables: intervention duration (short-term: ≤3 months; medium-term: 3–12 months; long-term: ≥12 months), exercise frequency (≤ 3 times/week; >3 times/week), duration of each exercise session (≤ 30 min; 30–60 min; ≥60 min), TCE type (e.g., Baduanjin, Yijinjing, Shaolin Neigong, Tai Chi), and whether the intervention was supervised. For outcomes with high heterogeneity, sensitivity analysis was conducted by excluding one study at a time to assess the robustness of the results and identify potential sources of heterogeneity. When subgroup analysis could not sufficiently explain heterogeneity, we performed meta-regression analysis to quantify the impact of possible confounding factors on the effect size and explore the sources of heterogeneity. According to the requirements of regression analysis, each covariate should include at least ten studies [25]. In this study, the pre-defined covariates included publication year, baseline BMI, sample size, and the proportion of males to systematically assess these variables’ impact on the effect size and supplement the unexplained sources of heterogeneity from the subgroup analysis.
All statistical analyses were performed using Stata software (version 17.0; StataCorp, College Station, TX, USA), and forest plots were used to visually present the combined effect size and its confidence intervals. The statistical significance level was set at p < 0.05.







Comments (0)