
Remember me

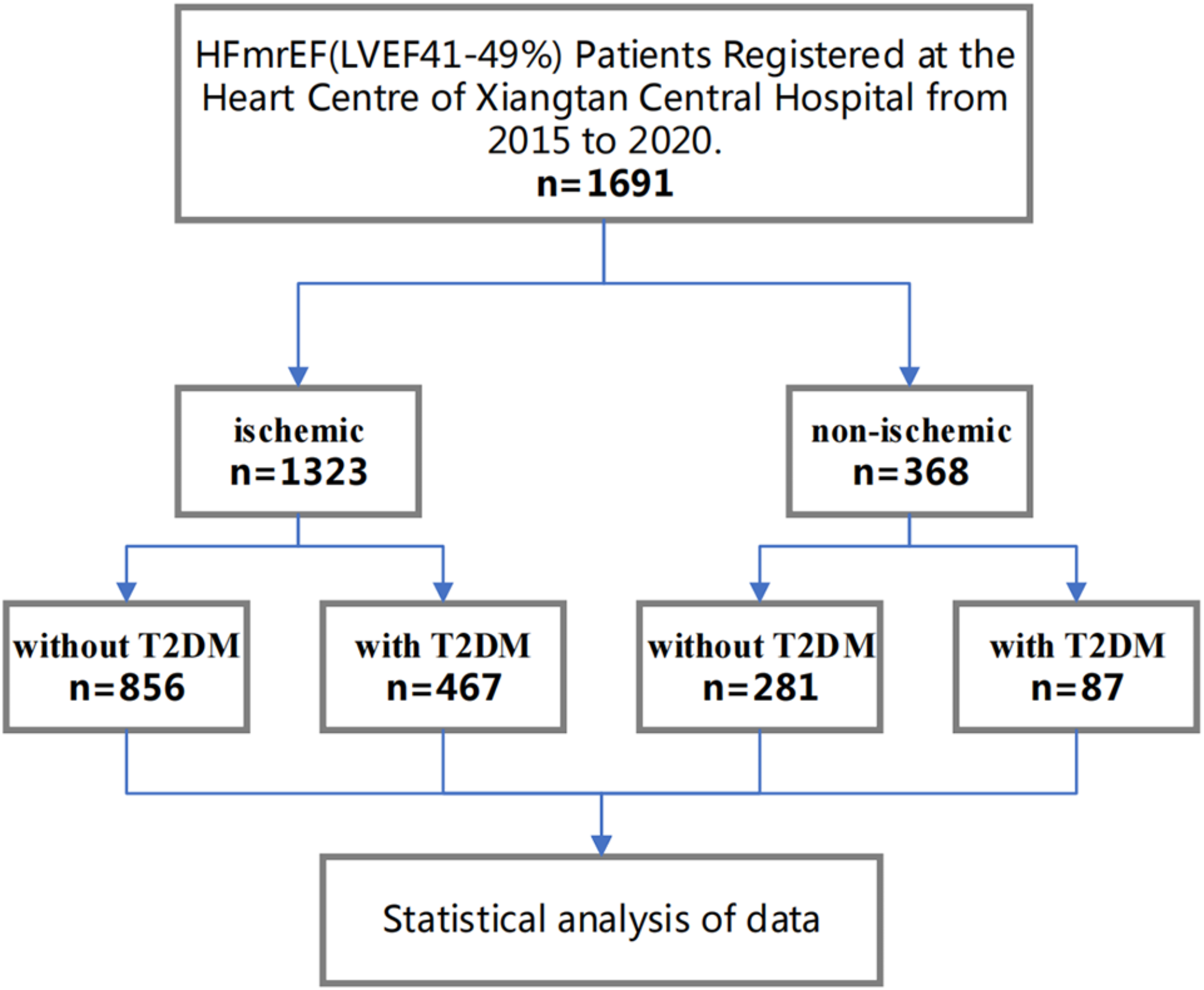





Table 1 outlines the baseline characteristics of ischemic and non-ischemic HFmrEF patients, stratified by the presence or absence of T2DM. Among the 1,691 participants, 467 had both ischemia and T2DM, 856 had ischemia without T2DM, 87 had T2DM without ischemia, and 281 had neither ischemia nor T2DM. In the ischemic group, the non-T2DM subgroup had an average age of 70.2 years, with 68.1% being male. In contrast, the T2DM subgroup had an average age of 68.3 years, with 62.5% being male. The non-ischemic group was younger: the non-T2DM subgroup had an average age of 63.8 years, with 58.7% being male, while the T2DM subgroup had an average age of 62.1 years, with 63.2% being male.
Table 1 Baseline characteristics of ischemic/non-ischemic HFmrEF patients stratified by the presence of T2DMClinically, there were notable differences in parameters such as blood pressure, heart rate, and prevalent comorbidities—obesity, smoking habits, hypertension, anemia, and renal dysfunction—across the stratified cohorts. Each clinical metric showed significant variations between the subgroups with and without T2DM. For instance, in the ischemic cohort, the prevalence of hypertension was higher in patients with T2DM (78.2%) compared to those without T2DM (66.5%). Similarly, in the non-ischemic cohort, hypertension rates were 56.2% in the non-T2DM subgroup and 80.5% in the T2DM subgroup.
Echocardiographic metrics, including left ventricular ejection fraction (LVEF), left atrial dimensions (LAs), and left ventricular diameter (LVd), also showed intergroup differences. Regarding heart failure pharmacotherapy, there were variations in the use of ACE inhibitors (ACEi), angiotensin II receptor blockers (ARB), β-blockers, and diuretics across the cohorts. Notably, compared to the non-T2DM subgroup, there was a significant increase in calcium channel blocker (CCB) use in the T2DM subgroup, as detailed in Table 1.
Key findingsIn patients with ischemic HFmrEF, the all-cause mortality for those without T2DM was observed to be 201 out of 856 (23.5%). In contrast, the T2DM cohort registered a mortality rate of 145 out of 467 (31.0%). Regarding cardiovascular events, 562 out of 856 (65.7%) events were noted in the non-T2DM group, whereas the T2DM group documented 338 out of 467 events (72.4%).
In the ischemic HFmrEF population, those diagnosed with T2DM displayed a significantly higher risk for all-cause mortality compared to their non-T2DM counterparts(Fig. 2A). An unadjusted model yielded a hazard ratio (HR) of 1.4 (95% CI: 1.1–1.8, P = 0.001), indicating a 40% increased risk of death in the T2DM group. When adjusted for age and gender, this HR increased to 1.7 (95% CI: 1.4–2.1, P < 0.001), reflecting a 70% increased risk. After full adjustment for confounders, the HR stabilized at 1.5 (95% CI: 1.2–1.9, P = 0.001), suggesting that T2DM continues to confer a clinically meaningful 50% increased risk of all-cause mortality in ischemic HFmrEF patients, independent of other factors. Regarding cardiovascular events, the risk was also higher in ischemic patients with T2DM(Fig. 2A), as evidenced by an HR of 1.2 (95% CI: 1.1–1.4, P = 0.002) in the crude model, and 1.3 (95% CI: 1.1–1.5, P < 0.001) after adjusting for age and gender. This remained consistent at an HR of 1.3 (95% CI: 1.1–1.5, P = 0.001) after comprehensive adjustment for confounders, indicating a clinically significant 30% increased risk of cardiovascular events in ischemic patients with T2DM.
Of the 1,323 ischemic HFmrEF patients assessed, propensity scores were assigned based on T2DM status. Following the alignment of all adjustment variables, baseline propensity scores were 0.35 ± 0.13 for non-T2DM individuals and 0.35 ± 0.14 for those with T2DM. A P-value of 0.5692 indicated no statistical difference, validating intergroup comparisons (for an in-depth post-PSM baseline, refer to Supplementary Table 1). Within the ischemic HFmrEF demographic, compared to non-diabetic individuals, those with T2DM had a significantly higher mortality risk, indicated by an HR of 1.40 (95% CI: 1.19–1.63, P < 0.0001). The risk increase also extended to cardiovascular events for T2DM individuals, marked by an HR of 1.13 (95% CI: 1.03–1.25, P = 0.0125) (detailed findings in Supplementary Table 2). These data align with the results from the multivariate Cox hazard model, supporting the robustness of the statistical conclusions.
Conversely, within non-ischemic HFmrEF patients, no significant associations between T2DM and the risks of all-cause mortality (HR 1.0, 95% CI: 0.6–1.7, P = 0.957) or cardiovascular events (HR 1.3, 95% CI: 0.9–1.9, P = 0.113) were observed (refer to Table 2 for specifics).
Table 2 Association between T2DM and clinical outcomes (all-cause death and cardiovascular events) in ischemic and non-ischemic HFmrEF patients: Cox regression modelsIndependent risk factors in ischemic HFmrEF patientsWe employed a multivariate Cox regression analysis to identify risk factors independently associated with adverse outcomes in ischemic HFmrEF patients (refer to Table 3). Variables with a significance level of P < 0.05 in the univariate Cox regression were included in the multivariate model.
Table 3 Cox proportional hazards regression model analysis for outcome risks in ischemic HFmrEF patientsOur results identified several factors independently linked to all-cause mortality: advanced age (HR 1.05, 95% CI 1.03–1.06, P < 0.0001), the presence of T2DM (HR 1.50, 95% CI 1.18–1.91, P = 0.0009), anemia (HR 1.65, 95% CI 1.28–2.12, P < 0.0001), undergoing PCI (HR 0.48, 95% CI 0.36–0.64, P < 0.0001), hyperuricemia (HR 1.37, 95% CI 1.07–1.75, P = 0.0137), prior stroke (HR 1.76, 95% CI 1.33–2.33, P < 0.0001), and elevated Log NT-proBNP levels (HR 1.16, 95% CI 1.06–1.26, P = 0.0013). These factors indicate a significant increase in the risk of mortality, particularly in patients with T2DM and those with elevated NT-proBNP levels.
Regarding cardiovascular events, advanced age (HR 1.01, 95% CI 1.00–1.02, P = 0.0026), T2DM (HR 1.29, 95% CI 1.11–1.49, P = 0.0009), anemia (HR 1.19, 95% CI 1.02–1.39, P = 0.0293), hyperuricemia (HR 1.34, 95% CI 1.14–1.58, P = 0.0004), atrial fibrillation (HR 1.32, 95% CI 1.09–1.59, P = 0.0042), hypertension (HR 1.19, 95% CI 1.01–1.40, P = 0.0403), and elevated Log NT-proBNP levels (HR 1.13, 95% CI 1.08–1.19, P < 0.0001) were independently associated with an increased risk of cardiovascular events. These findings corroborate our previous results, confirming that T2DM and elevated NT-proBNP levels are significant predictors of both all-cause mortality and cardiovascular events in ischemic HFmrEF patients.
Stratified evaluation in ischemic HFmrEF patientsUsing the CHAID algorithm for decision trees, we identified NT-proBNP levels of ≤ 441, 441 to 9401.22, and > 9401.22 pg/ml as potential prognostic benchmarks for all-cause mortality among diabetic individuals (see Fig. 3A). Similarly, NT-proBNP levels of ≤ 441, 441 to 2573, and > 2573 pg/ml were identified as potential prognostic indicators for cardiovascular events (Fig. 3B). For non-diabetic subjects, the relevant thresholds are delineated in Fig. 3.
Fig. 3
For ischemic HFmrEF patients, a classification tree using the CHAID algorithm was adopted to ensure the accuracy of the model. Potential risk factors related to the outcome event are: T2DM and NT-proBNP. (A) Categorization with T2DM and NT-proBNP based on all-cause mortality. (B) Categorization with T2DM and NT-proBNP based on cardiovascular event
Given that the decision tree identified NT-proBNP ≤ 441 pg/ml as a consistent benchmark for both endpoints in diabetic individuals, this stratified assessment considered NT-proBNP = 441 pg/ml as the pivotal threshold.
All-Cause Mortality Risk in Ischemic HFmrEF Patients with Concomitant Diabetes Mellitus:
Ischemic HFmrEF patients with concurrent diabetes mellitus displayed a heightened risk of all-cause mortality, irrespective of gender, age, NT-proBNP concentrations, atrial fibrillation status, hyperlipidemia, hypertension, hyperuricemia, anemia, or NYHA class III + IV designation. This elevated risk persisted in non-smoking, non-obese individuals, even in the absence of renal insufficiency, previous stroke, COPD, or prior PCI interventions (Fig. 4A).
Fig. 4
Forest plot of stratified analysis for ischemic HFmrEF patients based on the presence/absence of T2DM. (A) Outcome event: all-cause mortality. (B) Outcome event: cardiovascular event
Cardiovascular Event Risk in Ischemic HFmrEF Patients with Diabetes Mellitus:
Female ischemic HFmrEF patients aged above 70 years, with NT-proBNP concentrations surpassing 441 pg/ml, and those with NYHA class III + IV, hypertension, hyperuricemia, or anemia, demonstrated an increased risk for cardiovascular events. This observation held true regardless of their obesity status or the presence of atrial fibrillation. Furthermore, non-smokers and patients without hyperlipidemia, prior stroke, COPD, or a history of PCI also demonstrated this increased risk (Fig. 4B).
Therapeutic implications on outcomes for ischemic HFmrEF patients with T2DMUpon adjusting for age, gender, and heart failure medication usage, ischemic HFmrEF patients treated with two or more oral hypoglycemic drugs (HR 0.4, 95% CI 0.2–0.8, P = 0.007) or insulin therapy (HR 0.7, 95% CI 0.5–0.9, P = 0.020) showed a notably reduced all-cause mortality risk compared to their counterparts not on these regimens. After similar adjustments, ischemic HFmrEF patients receiving one (HR 0.7, 95% CI 0.6–0.9, P = 0.016) or more (HR 0.7, 95% CI 0.5–1.0, P = 0.039) oral hypoglycemic agents had a lower risk of cardiovascular events. Notably, insulin therapy (HR 0.9, 95% CI 0.7–1.1, P = 0.354) was not significantly associated with cardiovascular event rates (Table 4). No significant difference was noted in glycated hemoglobin levels between patients on oral hypoglycemic therapy and those not on it (Fig. 5A, P > 0.05). Conversely, those on insulin therapy showed reduced glycated hemoglobin levels compared to those not on the regimen (Fig. 5B, P < 0.05).
Table 4 Association between diabetes treatment and clinical outcomes in ischemic HFmrEF patientsFig. 5
Effects of glucose-lowering treatment on glycated hemoglobin (HbA1c) in ischemic HFmrEF patients with T2DM. (A) Impact of the number of oral hypoglycemic agents on glycated hemoglobin. (B) Influence of insulin use on glycated hemoglobin
Comments (0)