The epidemiological profile of IE has shifted towards older patients, driven by emerging risk factors [12, 13]. In developed countries, the mean age of IE ranges between 60 and 75 years [5, 13, 14]. Approximately 20 years ago, studies conducted in Türkiye reported a mean patient age of 36 years [15]; however, over the last decade, this has increased to a range of 48.5 to 58.3 years [16, 17, 18, 19]. In the largest previous case series by Şimşek-Yavuz et al. [9], the median age was reported as 47 years, whereas in the current study, it has risen to 57 years, reflecting a consistent upward pattern over the past decade.
The increase in patient age likely reflects changes in IE risk factors. Notably, in the 21st century, rheumatic fever has declined as a predisposing factor, while there has been a significant rise in the number of patients with prosthetic valves, ICDs, and degenerative valvular disease [6]. Similarly, in this study, the most frequently identified risk factors were prosthetic valves, ICDs, and degenerative valve disease. The increasing life expectancy and prevalence of degenerative heart diseases have led to a rise in interventional cardiac procedures, such as ICDs, contributing to the resurgence of CIED-IE [5]. This study demonstrates a statistically significant increase in CIED-IE over the past decade. Conversely, a significant decrease was observed in the prevalence of rheumatic fever and CHD. In the previous largest national case series, rheumatic fever accounted for 33.9% of IE cases [9], while in the present study, this proportion has notably declined to 8.3%. This substantial decrease is highly significant and underscores the changing epidemiology of IE, contributing valuable insights to national data.
Another predisposing risk factor, IVDU, was reported to be 0.9% in previous studies conducted in Türkiye [9], whereas this study found the frequency to be 4.5%. In different studies, the reported frequency has been documented to range between 2.6% and 7.8% [5, 20, 21]. It is well-documented that the rate of IVDU in Türkiye has been increasing annually. According to the Turkey Drug Report 2023, the number of applications to inpatient addiction treatment centers increased from 9,824 in 2020 to 14,042 in 2022 [22, 23]. The rising prevalence of IVDU highlights a significant public health concern and suggests that IVDU may emerge as a critical risk factor for IE in our country as well.
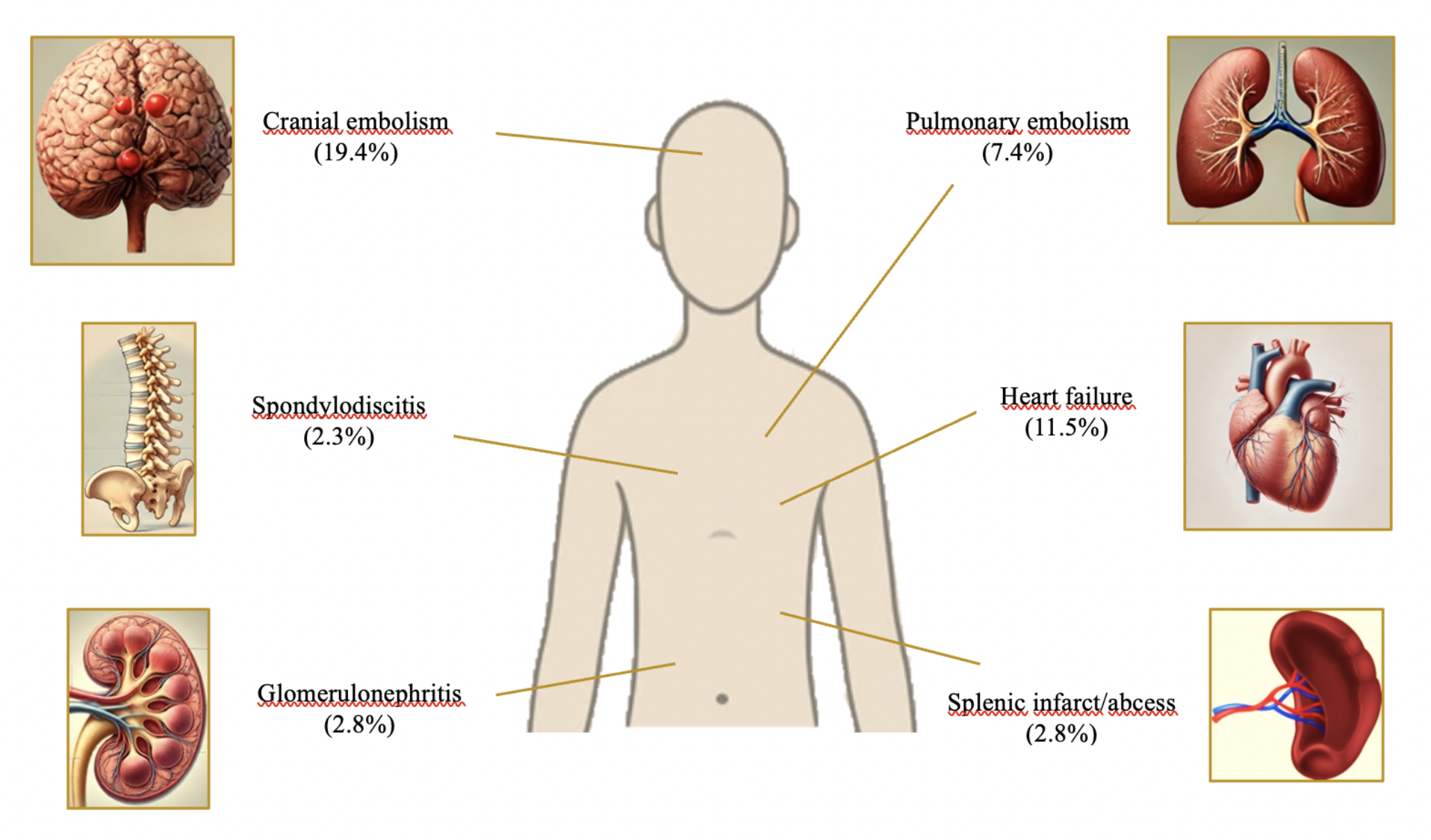
Right-sided IE accounts for approximately 5–10% of all cases, with its lower incidence compared to left-sided IE attributed to fewer pathological conditions affecting right-sided valves, anatomical-vascular differences and lower pressure gradients. The presence of ICDs, IVDU, and central venous catheters can increase the likelihood of right-sided IE, often involving the tricuspid valve [24, 25, 26]. The increase in tricuspid valve involvement to 12.9% during the study period, along with the rise in lead involvement to 9.8% and the prevalence of ICDs to 13.8%, reflects a significant pattern in the Türkiye cohort, highlighting the growing incidence of CIED-IE cases. Additionally, the increasing incidence of pulmonary embolism, one of the most common complication of right-sided IE [24], in this cohort may be associated with the rising prevalence of tricuspid valve involvement and CIED-IE.
In this study, a statistically significant decline in surgical intervention rates was observed, which may be attributed to the changing epidemiological characteristics of the patient cohort. Advanced age, comorbidities, and prior procedures often lead to hesitancy toward surgery among clinicians and patients. Compared to younger patients, it is a well-known fact that surgical intervention is less frequently performed, and mortality rates are higher in elderly infective endocarditis patients [1]. The EURO-ENDO registry demonstrated that surgery was less frequently performed in patients over 80 years of age [27]. A Swedish analysis reported that surgery was underutilized in elderly IE patients, resulting in significantly higher 1-year mortality rates for those who did not undergo surgical intervention [28].
Despite advances in medical care, the increasing complexity of patients has contributed to the persistently high mortality rates of IE in recent decades [5]. The literature reports hospital mortality rates for IE ranging from 15 to 30% [6, 22, 30]. Previous studies conducted in Türkiye have reported higher hospital mortality rates, ranging from 27.8 to 36% [9, 17, 19]. In this study, the hospital mortality rate was 22.8%, reflecting a decline compared to earlier national studies; however, it remains alarmingly high.
Numerous studies have identified key risk factors associated with in-hospital mortality in IE, including ≥ 65 age, S. aureus or fungal etiology, prosthetic valve, dual-valve involvement, neurological complications, and CKD requiring HD [29, 30, 31, 32]. In particular, HCA-IE infections in prosthetic valve endocarditis have been recognized as a significant contributor to increased mortality [10]. Consistent with the literature, this study identified older age, CKD, nosocomial infection, candidal etiology, prosthetic valve involvement and CNS embolism as significant risk factors associated with increased mortality in IE. Previous studies have demonstrated that a vegetation size greater than 10 mm is associated with an increased risk of embolic complications and mortality [33]. However, in this study, the threshold value was identified as 15 mm. Similarly, studies conducted by Erbay et al. [34] and Thurny et al. [35] also reported that vegetations larger than 15 mm were significant risk factors for mortality.
Changes in the at-risk population for IE have significantly influenced its microbiological profile [31]. Chronological increases in the frequency of S. aureus IE over recent decades are well-documented in the literature [7]. Consistent with these findings, our study identified Staphylococcus spp. as the most frequently observed pathogens in all type IE, with a particularly notable rise in S. aureus cases over the study period. This predominance of S. aureus is likely associated with increasing patient age, the rising prevalence of CIED-IE, HCA-IE, and IVDU. These changes in the etiological microorganism profile can influence the clinical presentation and complication patterns of IE. Spondylodiscitis is the most common osteoarticular complication of IE [10], and its increasing incidence has been documented in this study. S. aureus is well recognized as the predominant causative pathogen of spondylodiscitis [36], and its increasing prevalence in this cohort is likely linked to the rising incidence of this complication observed in this study.
The decreasing prevalence of culture-negative IE in our country is very important. The establishment of proper blood culture collection practices before initiating antibiotics, along with the diagnostic algorithms outlined in the Turkey Consensus Report [37], have contributed to a reduction in the rate of culture-negative endocarditis. In 0.9% of culture-negative endocarditis cases, Coxiella was identified as the causative agent, while Brucella accounted for 0.7% and Bartonella for 0.1%. One of the focal complications of brucellosis, which is endemic in our country, is endocarditis [38, 39]. In a study conducted by Şimşek et al. in our country [9], brucellosis was identified as the cause of infective endocarditis in 4.6% of cases, whereas in our study, this rate was found to be 0.7%, which is surprising.
The limitations of this study can be summarized as follows. Firstly, this was a retrospective study. Although the primary centers for the diagnosis and treatment of infective endocarditis remained constant throughout the study period, the incorporation of additional centers over time may have introduced potential bias. The cases in this study were classified as possible or definite IE according to the 2015 ESC criteria, which were valid at the time. However, as diagnostic criteria continue to evolve, the potential for overdiagnosis or missed cases remains a limitation of this study. While a significant part of the culture-negative endocarditis cases is attributed to antibiotic use, this information could not presented in this study. Furthermore, due to insufficient data, the effects of endocarditis prophylaxis on epidemiological outcomes could not be investigated. The lack of the examination of treatment modalities and surgery-related data in detail is another limitation of the study. The decline in case numbers during the third time period may be attributed to the impact of the COVID-19 pandemic on case reporting processes, as data reporting from major cardiac centers remained consistent, while some centers experienced disruptions in data flow, potentially introducing a source of bias. Generalisability is limited despite its large sample size and country-wide-distributed setting. Providing a nationwide perspective on infective endocarditis, addressing certain knowledge gaps in this field, and integrating clinical and microbiological findings to interpret national data constitute major strengths of this study.
The epidemiology of IE is evolving due to several factors leading to changes in its microbiological characteristics and clinical presentation. Patients are now generally older and have a greater burden of comorbidities. Prosthetic valves, ICDs, and HD have emerged as the risk factors, replacing rheumatic disease and CHD. Staphylococcus spp. has become the most commonly isolated pathogen. The management of IE patients should be guided by clinical guidelines, with consideration of up-to-date epidemiological data to ensure comprehensive and evidence-based care.

Comments (0)