
Remember me
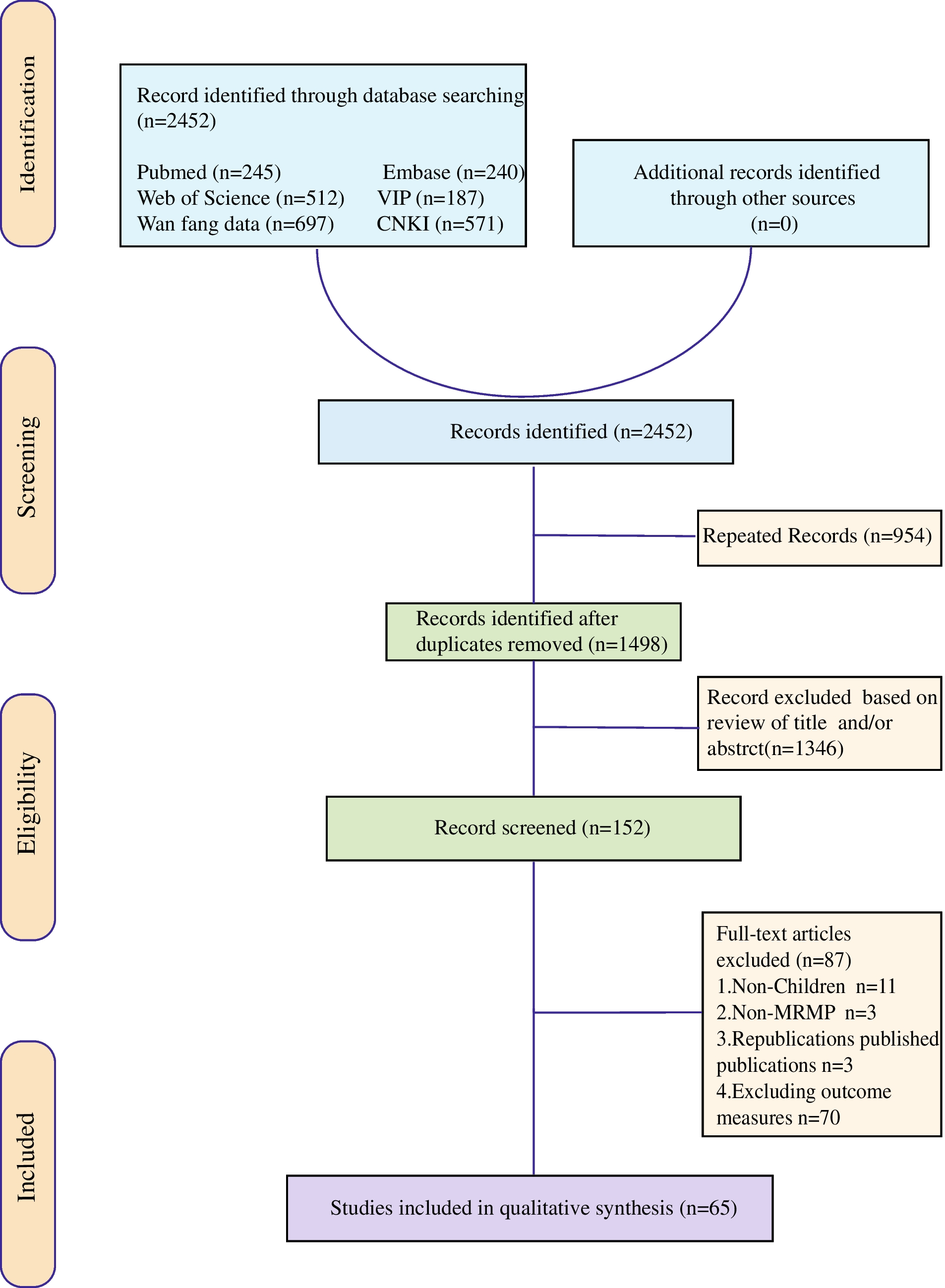
The patient disposition is shown in Fig. 1. Of 314 screened patients in the EAP, 261 patients were eligible for inclusion in the primary analysis. Most of the exclusions from the study occurred due to lack of verified information on the baseline Gram-negative bacteria and treatment duration of < 72 h. A total of 13 patients were treated with cefiderocol for > 28 days, thus, excluded from the primary analysis. A total of 50 centres, mostly tertiary hospitals, participated in the study across Spain.
Fig. 1
Patient enrolment and flow through the study; aVerification between the infection site and the biospecimen was absent
Patient characteristics, comorbidities and baseline Gram-negative bacterial infectionsThe median age was 61.0 years and 77.4% were male (Table 1). At least one comorbid condition was present in 76.2% of patients, most frequently cancer, diabetes mellitus, chronic kidney disease and chronic obstructive pulmonary disease (Table S1). Cefiderocol was initiated in the ICU for > 60% of patients. At the time of cefiderocol initiation, the median SOFA score was 8.0, 47.1% of patients received mechanical ventilation, while septic shock (28.0%), renal replacement therapy (27.2%), creatinine clearance < 60 mL/min (30.5%), immunosuppression (30.3%) and symptomatic COVID-19 infection (24.1%) were common (Table 1).
Table 1 Patients’ baseline demographics and clinical characteristics, and resistance profile of baseline Gram-negative pathogens in the overall primary analysis population (N = 261) and in patients with P. aeruginosa (N = 174)P. aeruginosa was the most frequent Gram-negative pathogen (174/261; 66.7%) (Table 1). The current manuscript reports on patients with P. aeruginosa (N = 174), Pseudomonas spp. (N = 15), K. pneumoniae (N = 26) and other Enterobacterales (N = 12). Further demographic, baseline characteristics and other data for patients infected by S. maltophilia (N = 20), Burkholderia cepacia complex (N = 8), Achromobacter spp. (N = 5) and Ralstonia mannitolilytica (N = 1) are summarised in the accompanying paper.
Baseline demographics and clinical characteristics for patients infected by P. aeruginosa were similar to those in the overall population (Table 1, Table S1, Table S2). There were some numerical differences in baseline demographics and clinical characteristics among patients infected by Pseudomonas spp., K. pneumoniae and other Enterobacterales (Table S1, Table S3).
The most frequent infection site was the respiratory tract overall, and among patients with P. aeruginosa and K. pneumoniae infections (Table 1, Table S3). While > 50% of the population were previously colonised with the same pathogen, particularly among patients with Enterobacterales and K. pneumoniae, secondary bloodstream infection and polymicrobial infections were less frequent (Table 1, Table S3).
Based on susceptibility data reported in the medical charts, > 90% of isolates with confirmed susceptibility status were resistant to meropenem, 83.8% were resistant to ceftazidime-avibactam and 76.2% were resistant to ceftolozane-tazobactam (Table 1). The mechanisms of β-lactam resistance were reported for 48.7% of isolates overall (n = 127) and 46.0% of P. aeruginosa isolates (n = 80); metallo-β-lactamases, mainly imipenemase and Verona integron-encoded carbapenemases, were most frequent enzymes (overall: n = 98; P. aeruginosa: n = 73) (Table S2).
Patient characteristics by infection site are shown in Table S4. Patients with urinary tract infection were older (median age 66.5 years) than patients with any other infection site (median age range 54.5–62 years). The Charlson Comorbidity Index was highest (4.0) among patients with intra-abdominal infection, urinary tract infection, and bone and joint infection. Polymicrobial infections were most frequent in patients with respiratory tract infections (24.0%) and other infection site (25.0%) (Table S4).
Treatment patternsPrior Gram-negative antibiotics were administered to 81.2% of patients (missing: n = 7). The median number of prior courses of antibiotic treatments was 2.0 and the median duration of prior antibiotic treatment was 6.0 days (Table 2). Patients most frequently received colistin (36.4%), ceftazidime-avibactam (31.0%), meropenem (30.7%); prior antibiotics varied by baseline Gram-negative pathogen (Table S5).
Table 2 Pattern of cefiderocol use, and prior and concomitant antibiotic use in the overall primary analysis population (N = 261) and in patients with P. aeruginosa (N = 174)Physicians most frequently administered cefiderocol due to resistance to all other tested antibiotics (64.8%) and/or failure of prior treatment (44.4%) (Table 2). Cefiderocol was administered as first-line treatment for 16.1% of patients overall (n = 42) and 14.4% of patients with P. aeruginosa (N = 25), while the median duration of cefiderocol treatment was 10.0 days and 11.0 days, respectively. The median duration of cefiderocol treatment by infection site was longer in patients with skin and skin structure infections (12.5 days), bone and joint infections (16.5 days), and other infection sites (18.0 days) (Table S4). Among patients with respiratory tract infections, nearly half (46.4%) of patients received cefiderocol combination therapy and 53.0% of patients received cefiderocol following administration of ≥ 3 prior courses of antibiotic treatments (Table S4). Cefiderocol was administered every 8 h to 213 (81.6%) patients overall. Only one patient, infected by K. oxytoca, discontinued cefiderocol treatment due to development of on-therapy resistance. Cefiderocol was given in combination therapy with antibiotics with Gram-negative coverage to approximately one-third of patients overall and of those with P. aeruginosa. Colistin was the antibiotic most frequently co-administered with cefiderocol in 19.5% of the patients (Table S6).
Outcomes overall and by baseline infection variablesIn the primary analysis population, 80.5% of patients (210/261) had clinical cure at end of treatment and 28-day all-cause mortality was 21.5% (56/261) (Fig. 2). In the subset of patients with P. aeruginosa, the clinical cure rate was 84.5% (147/174), and the 28-day mortality rate was 17.2% (30/174) (Fig. 2). All-cause mortality at day 14 was 14.2% (37/261) in the overall primary analysis population and 10.3% (18/174) for patients with P. aeruginosa infections. The overall clinical success rate was 84.3% (220/261) and 89.1% (155/174) in patients with P. aeruginosa.
Fig. 2
Rates of clinical cure at end of treatment and all-cause mortality at Day 28, in the overall primary analysis population (N = 261) and by baseline Gram-negative pathogen. NF-GN, non-fermenter Gram-negative; Other Enterobacterales (n): S. marcescens (5), E. cloacae (3), K. oxytoca (2), C. freundii (1), Serratia spp. (1); Pseudomonas spp. (n): P. putida (12), Pseudomonas fluorescens/putida group (1), P. fluorescens (1), P. nitroreducens (1); Other NF-GN (n): Burkholderia cepacia complex (8), Achromobacter spp. (5), Ralstonia mannitolilytica (1)
Clinical cure rates varied by infection site; thus, the highest clinical cure rates were found among patients with infections of the urinary tract, skin and soft tissue, bone and joint, and other sites (Fig. 3). Rates of clinical cure and 28-day all-cause mortality were similar for patients with respiratory tract infections, intra-abdominal infections, and bloodstream infections overall (Fig. 3).
Fig. 3
Rates of clinical cure at end of treatment and all-cause mortality at Day 28 by infection site in the overall primary analysis population (N = 261). BSI, bloodstream infection; IAI, intra-abdominal infection; UTI, urinary tract infection; aIncludes central nervous system infection (n = 2) and mediastinitis (n = 2)
Similar trends were observed among patients with P. aeruginosa infections (Fig. 4).
Fig. 4
Rates of clinical cure at end of treatment and all-cause mortality at Day 28 by infection site in patients with Pseudomonas aeruginosa (N = 174). BSI, bloodstream infection; IAI, intra-abdominal infection; UTI, urinary tract infection; aIncludes central nervous system infection (n = 2) and mediastinitis (n = 1)
The presence or absence of immunosuppression, COVID-19, colonisation with the same multidrug-resistant pathogen, mono- or polymicrobial infection had no effect on clinical cure and 28-day mortality rates (Table S7). However, presence of septic shock, ICU admission, renal replacement therapy and mechanical ventilation at baseline resulted in lower clinical cure rates and higher all-cause mortality rates than in patients without these features (Table S7). Rates of clinical cure and 28-day all-cause mortality by pathogen and infection site are shown in Table S8.
Outcomes by antibiotic resistance, prior antibiotic use and Cefiderocol useClinical cure and 28-day all-cause mortality rates were similar between subgroups of infections caused by pathogens resistant to meropenem, ceftolozane-tazobactam and/or ceftazidime-avibactam, or colistin (Table 3, Table S7).
Table 3 Clinical cure, all-cause mortality at day 28, and composite clinical success rates overall, by antibiotic resistance and antibiotic use in the overall primary analysis populationAmong patients who received colistin, meropenem, ceftazidime-avibactam, or ceftolozane-tazobactam prior to cefiderocol, the clinical cure rates ranged between 72.5% and 77.9% overall, and between 78.2% and 81.5% for patients with P. aeruginosa infections (Table S7). Corresponding 28-day all-cause mortality rates ranged between 16.7% and 28.8%, and between 11.1% and 21.8% by prior antibiotic treatment, respectively (Table S7).
Cefiderocol administered as first-line therapy resulted in numerically higher clinical cure rates compared with patients who received it later (Table 3). Patients with cefiderocol combination therapy had numerically lower rate of clinical cure compared with monotherapy (Table 3, Table S7).
Univariate and multivariate regression analysis and Kaplan-Meier survival analysisAmong the risk factors identified in the univariate and multivariate stepwise logistic regression analyses for clinical cure, duration of prior antibiotic treatment before cefiderocol initiation (i.e. >7 days vs. 0 day [categorical variable]) (OR 0.19, 95% CI 0.05–0.56) and receipt of mechanical ventilation at baseline (OR 0.32, 95% CI 0.15–0.67) were significantly associated with a reduced probability of achieving clinical cure (Table 4). The only variable included in the final model showing a trend towards better outcome was infection by P. aeruginosa (OR 1.97, 95% CI 0.97–4.00). Among patients with P. aeruginosa, presence of septic shock (OR 0.22, 95% CI 0.08–0.58), receipt of mechanical ventilation at baseline (OR 0.35, 95% CI 0.11–0.98), duration of prior antibiotic treatment (OR 0.93, 95% CI 0.87–0.98 [continuous variable]) and age (OR 0.94, 95% CI 0.90–0.99) showed significant effect on clinical cure (Table S9).
Table 4 Univariate and multivariate logistic regression analysis for clinical cure at EOT in the overall primary analysis population (N = 261)To evaluate the impact of duration of prior antibiotic treatment on survival from initiation of cefiderocol treatment for up to 28 days, an unadjusted Kaplan-Meier survival analysis was performed. The analysis showed that the probability of survival was significantly lower when patients received prior antibiotic treatment for longer than 7 days compared with patients who received no prior antibiotic treatment (Fig. 5).
Fig. 5
Kaplan–Meier analysis of probability of survival from initiation of cefiderocol treatment for up to 28 days in the overall primary analysis population (N = 261; missing n = 7)
*This category includes three patients who did not receive at least one full calendar day of prior antibiotic treatment but received one or two doses
Adverse drug reactionsSeven patients (2.2%) experienced adverse drug reactions, three of which were serious and resulted in discontinuation of treatment (Table 5). Six patients recovered and one patient died with a serious event (i.e. toxic epidermal necrolysis).
Table 5 Adverse drug reactions in all screened patients
Comments (0)