
Remember me
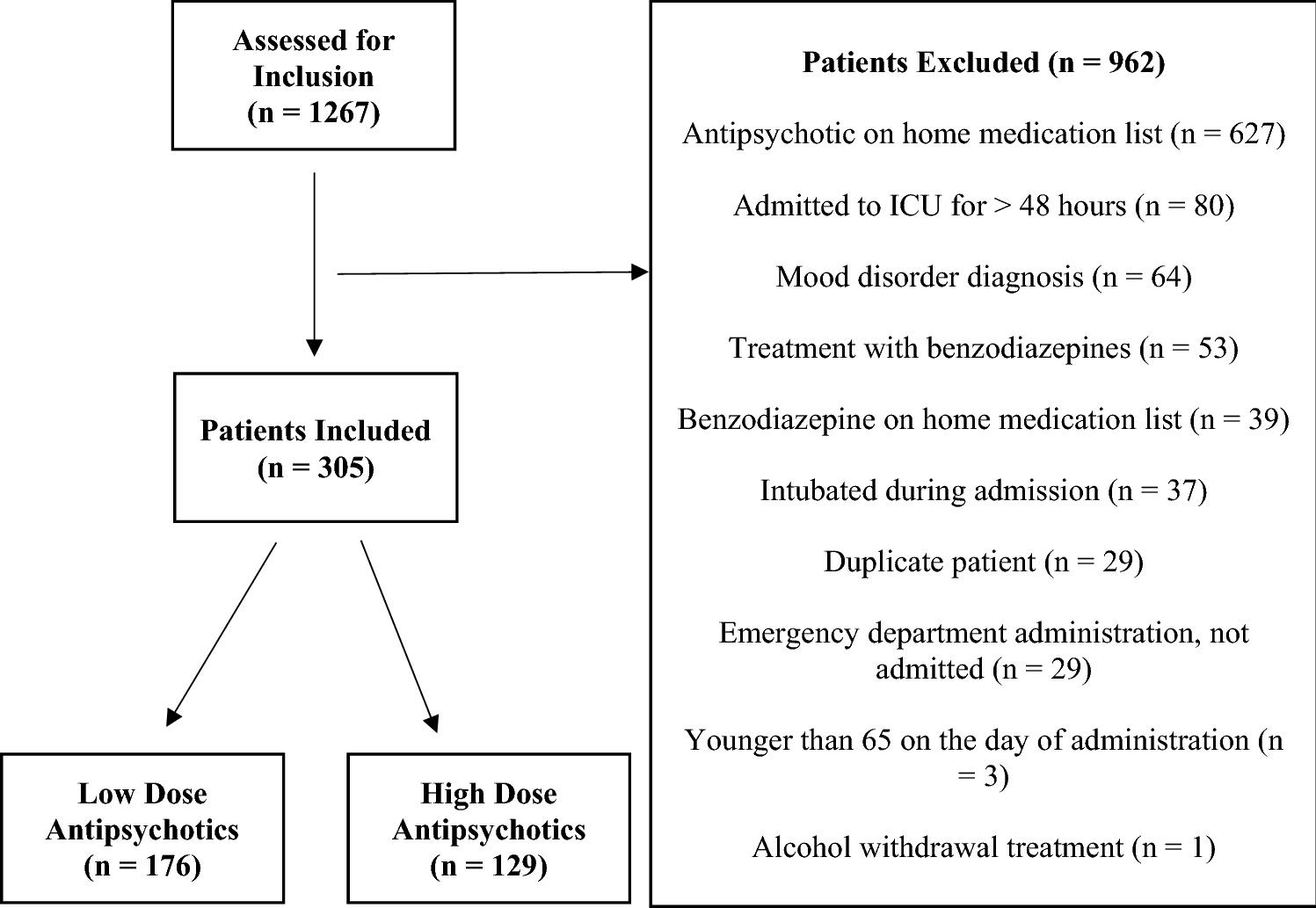

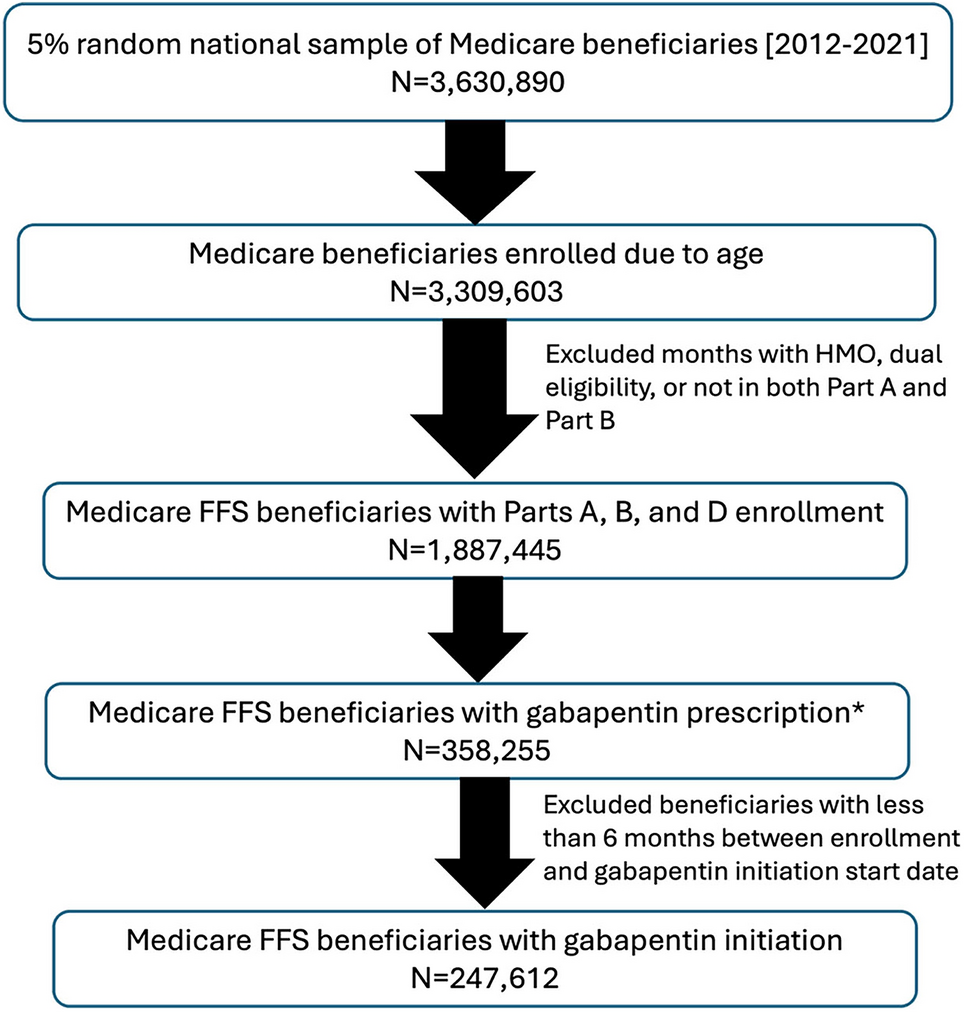
The searches identified 8825 individual citations of which 163 were selected for full text assessment and 29 papers were eligible for inclusion in the review. An additional three eligible papers were identified from the screening of reference lists of included papers, with a total of 32 papers included in this review (Fig. 1). Translation of one potentially eligible non-English paper was unavailable.
Fig. 1: 3.1 Study Characteristics
3.1 Study CharacteristicsThe 32 papers included in this review reported findings from 28 unique research studies (Table 2). All included papers were published between 2013 and 2024. Studies were conducted in 12 countries: Canada (n = 6), Spain (n = 6), the USA (n = 5), Australia (n = 2), the UK (n = 2), France (n = 1), Ireland (n = 1), Italy (n = 1), Japan (n = 1), Sweden (n = 1), Taiwan (n = 1) and the Netherlands (n = 1). Over half of the papers reported studies completed in long-term residential care settings (n = 19). Papers also reported studies undertaken in primary care or community healthcare services (n = 6), hospital inpatient settings (n = 5), hospital outpatient settings (n = 1) and across multiple settings (n = 1). Papers primarily focussed on deprescribing of either psychotropic medications (n = 16, all but one in long-term care settings) or PIMs (n = 9). Eight papers reported randomised controlled trials (RCTs). The length of follow-up ranged from 11 days (mean length of hospital admission) to 2 years, with most papers reporting follow-up periods of 6 (n = 12), 9 (n = 5) or 12 months (n = 5). Attrition was reported in half of the papers (n = 16) and ranged from 8% to 51%, with the main reasons cited being death or a change in the care setting of the participants. The assessed quality of the papers was variable. Quality issues were highlighted with quantitative studies that did not use randomisation to allocate to comparison groups (non-randomised studies) more frequently than with RCTs, quantitative descriptive studies and mixed methods studies. These issues particularly related to confounders and sample representativeness, with non-randomised studies accounting for more than half of the studies (n = 16).
Table 2 Characteristics of the papers included in the reviewIn total, 11 of the 32 papers reported interventions that included active involvement of patients and/or informal carers in the medicine optimisation or deprescribing process [32,33,34,35,36,37,38,39,40,41,42]; only one [39], a medication review and education intervention, incorporated shared decision-making. The study protocol reports dialogue between the professionals, person with dementia and their carer during the medication review [43]. In addition, nine papers reported person-centred deprescribing interventions [32,33,34,35,36,37,38, 41, 42]; however, it is not possible to determine from the papers whether this involvement implemented shared decision-making principles. Another paper reported an intervention [40] that empowered patients to lead deprescribing decision-making through the use of educational materials.
3.2 Participant CharacteristicsStudy sample sizes ranged from 29 to 17933 patients. Participants were predominately older people, with the mean patient age ranging from 74 to 88 years. However, this does not preclude a small minority of the study populations from being aged under 65 years; one study explicitly stated that 4% of the participants were under 65 years [44], with an age range of 55 to 99 years (mean of 84 years) provided in one study set in long-term care [45, 46]. Moreover, seven studies explicitly recruited populations aged 65 years and over [32,33,34, 41, 47,48,49,50,51] and one recruited participants aged 60 years and over [38]. The percentage of female patients ranged from 51% to 79%, except in two outlier studies (one recruited only male patients [52], whilst the other had 22% female patients [47]). In total, 26 papers reported on outcomes for people with dementia, 5 for people with either dementia or MCI and 1 for people with MCI only. Participant dementia type was rarely provided, with this information only provided in five studies [45, 46, 48, 49, 51, 53, 54]. The diagnosis of dementia or MCI was determined by the study authors, mostly using medical records, including documented diagnosis, prescription of anti-dementia medication or other relevant information. Some study authors also used one or more of the following criteria to determine a diagnosis of dementia or MCI: (1) being a resident in a long-term care dementia unit, (2) assessment by specialist professionals and (3) the use of tools to assess disease severity, including the Clinical Dementia Rating Score, Functional Assessment Staging Test, Global Deterioration Scale, Mini Mental State Examination and Montreal Cognitive Assessment.
3.3 Types of InterventionsOwing to heterogeneity of outcome measures and study designs, papers were grouped according to the intervention investigated as either “medication review and healthcare professional education interventions” (14 papers), “medication review interventions” (13 papers) or “patient, carer and/or healthcare professional education interventions” (5 papers), although there was considerable variation between interventions in each group.
Medication review and healthcare professional education interventions (reported in 14 papers) [35,36,37,38,39, 45, 46, 50, 52, 55,56,57,58,59], all implemented in long-term care settings, involved formal education that included a focus on deprescribing delivered either through taught sessions or by provision of information. The medication review component of the interventions was led by either a doctor, pharmacist or a multi-disciplinary (MDT) team.
Medication review interventions (reported in 13 papers) [34, 41, 42, 44, 47,48,49, 54, 60,61,62] were either a standalone intervention (n = 10/13) or combined with other components (such as a new model of coordinated primary care or proactive medication monitoring), with data specifically relating to the medication review reported. These were implemented in a range of settings. In total, seven papers reported medication reviews led by pharmacists, four papers reported MDT-led reviews and one paper reported an automated review using a computer algorithm triggering alerts to professionals. There were no details provided of the medication review process in one paper.
Patient, carer and/or healthcare professional education interventions (reported in five papers) all included formal education relating to deprescribing as the only intervention [32, 33, 40, 63, 64]. Two reported studies were completed in long-term care settings and three in primary care or community settings. These involved either educational sessions or the provision of educational materials: two interventions were solely for professionals, one intervention was solely for patients and two interventions involved patients, informal carers and professionals.
Variation in intervention characteristics within these groups are explored in the synthesis narrative and more details about each individual intervention is provided in Online Resource 2. A range of deprescribing tools was used across all intervention group types, including Beers criteria [65], the Screening Tool of Older Person’s Prescriptions (STOPP) [66], anticholinergic burden scores, national or provincial guidelines, and intervention specific tools (Table 2). These were used either to inform the intervention, such as medication review or educational content, or to identify inappropriate medications for the purposes of measuring study outcomes.
3.4 Outcomes of InterventionsTo assess effects of the interventions, the outcomes have been grouped into medication-related outcomes (reported in 28/32 papers), clinical-related outcomes (reported in 19/32 papers), and safety-related outcomes (defined as reported adverse events, hospital admission and/or mortality; reported in 10/32 papers) and are outlined in Sections 3.4.1–3.4.3. Less than four papers reported outcomes related to feasibility and/or costs, and measurements were too varied to usefully synthesise.
The direction of effect of the interventions on each outcome is summarised in Table 3 (full details are provided in Online Resource 3).
Table 3 Direction of effect of intervention on study outcomes for each included paper3.4.1 Medication-Related Outcomes3.4.1.1 Psychotropic MedicationIn total, 17 papers reported impact on psychotropic prescribing in general (n = 6) or specific medication classes [such as antipsychotics (n = 6) or benzodiazepines (n = 1)] from across all intervention groups. The studies were primarily completed in long-term care settings (n = 14) [35,36,37,38, 41, 45, 53, 55,56,57,58,59, 63, 64], with two in community settings [40, 42] and one in an inpatient setting [61]. Effects were not measured in the same way across the studies. The most common measures used were the percentage of participants for whom psychotropic medications were stopped or reduced (n = 7) and the change in the mean number of psychotropic medications per participant (n = 5).
A decrease in at least one class of psychotropic medication was reported in 12 out of the 17 papers [
Comments (0)