
Remember me





JCCNG 2024 was developed to help healthcare providers understand and provide nutrition therapy that will improve the outcomes of patients, such as mortality, length of ICU stay, length of mechanical ventilation use, adverse events, and physical functions.
Target population and usersThe target population includes children and adults admitted to ICUs or requiring intensive care, regardless of the type of disease. The intended users of these guidelines are all healthcare professionals involved in intensive care, including those who are not familiar with nutrition therapy.
Relationship with other guidelinesASPEN [5] and ESPEN [4] have published guidelines on nutrition therapy for critically ill patients. However, there are still important CQs outside these guidelines, and the feasibility of nutrition therapy differs depending on countries and regions due to differences in healthcare systems. Therefore, it is important that guidelines for nutrition therapy using the GRADE approach are provided in Japan. These guidelines provide 37 CQs and 24 recommendations, covering immunomodulation therapy, nutrition therapy for special conditions, and nutrition therapy for children. It is important to note that these recommendations are not intended to limit any treatment or the management of patients.
OrganizationJCCNG 2024 was developed in accordance with the GRADE system by a process of developing CQs; searching, collecting, and integrating evidence by a systematic review; evaluating the certainty of evidence (CoE); and formulating recommendations. Experts from various healthcare fields related to nutrition therapy and/or critical care were gathered, including physicians specialized in critical care, emergency medicine, surgery, internal medicine, pediatrics, and anesthesiology, a nurse, dietitian, pharmacist, and physical therapist. A guideline development group (GDG), working groups, systematic review teams, and a methodological support team were then established.
The GDG, named the JCCNG Committee, was established and approved by the Japanese Society of Intensive Care Medicine. The GDG developed and decided on the scope, CQs, and recommendations in the guidelines. The working group comprised members of the Japanese Society of Intensive Care Medicine who were recruited or nominated by the GDG, while some members of the GDG also served as a member of the working group. The working group supported the development of CQs, supervised the systematic review, and drafted the recommendations. Systematic review teams were recruited from members of the Japanese Society of Intensive Care Medicine and conducted the systematic review. The methodological support team comprised physicians and nurses appointed by the GDG, and educated and supported members of the working groups and systematic review teams by explaining the GRADE approach and preparing academic materials from a neutral standpoint.
Quality and transparency controlAfter a draft of the guidelines was formulated, it was peer-reviewed by external evaluators using AGREE II and revised according to their comments and suggestions. To ensure quality and transparency, the contents of the guidelines were peer-reviewed by the members of the GDG and public comments were obtained from several academic organizations. In addition, the drafting processes were disclosed to all members involved in the guideline development process, and all meetings of the GDG were held in public.
Plans for dissemination and revisionFlowcharts to clinical practice (Figs. 1, 2, 3) and a quick reference list of CQs and answers (Table 1) based on JCCNG 2024 are shown. JCCNG 2024 will be disseminated by educational activities mainly by the JCCNG Committee at various scientific meetings and seminars. The dissemination of an application that includes the contents of the guidelines are also planned. In addition, monitoring the degree of the clinical adaptation of JCCNG 2024 using a questionnaire by the committee is planned.
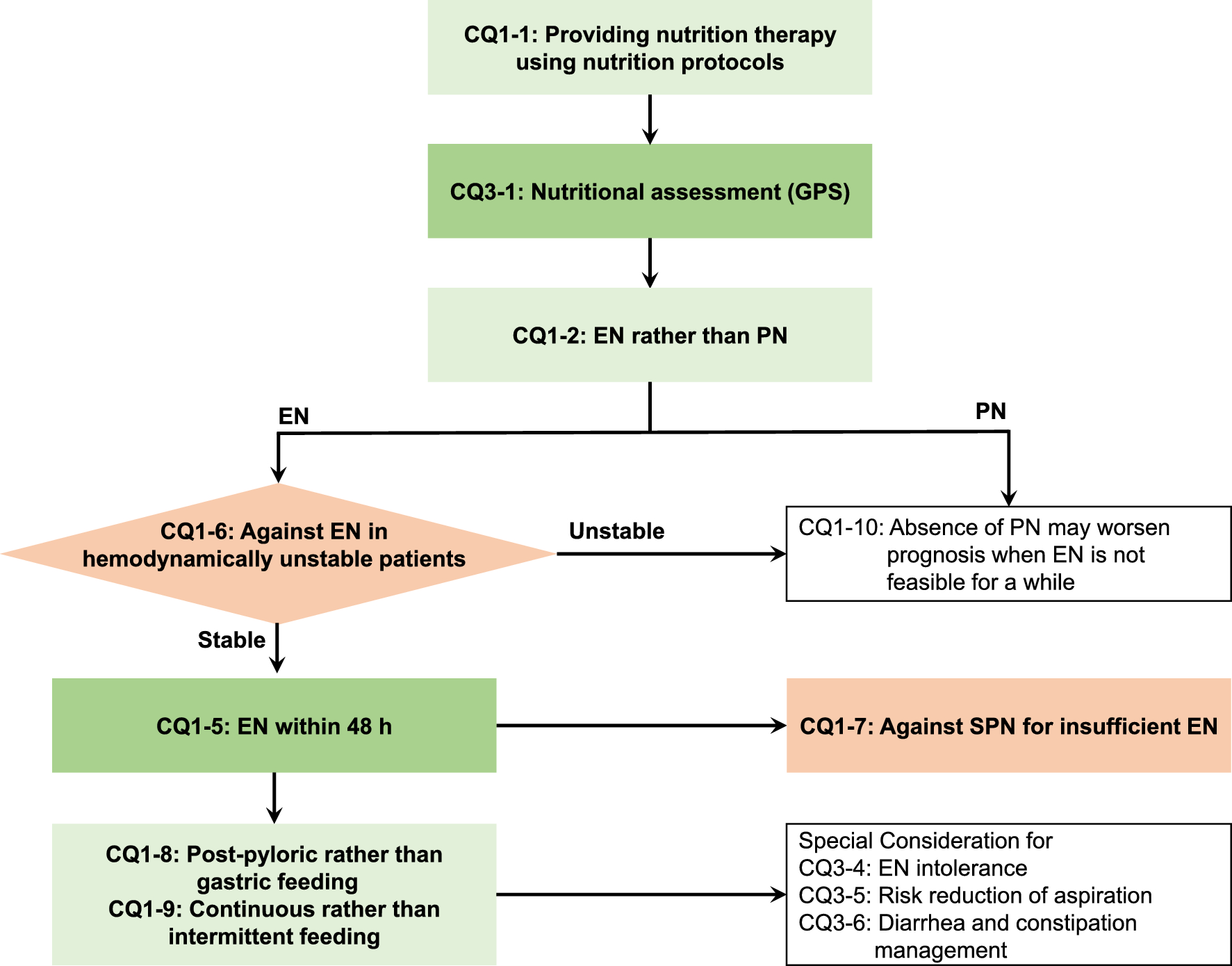
Fig. 1
Nutrition delivery routes and methods for critically ill adult patients. Nutrition delivery routes and methods for critically ill adult patients answered in the guidelines are shown as a flowchart of clinical practice. Green boxes indicate answers recommended, red boxes indicate answers not recommended, and white boxes indicate answers for background questions. CQ: clinical question; GPS: good practice statements; EN: enteral nutrition; PN: parenteral nutrition; SPN: supplemental parenteral nutrition
Fig. 2
Nutrition amounts and nutrients for critically ill adult patients. Nutrition amounts and nutrients for critically ill adult patients answered in the guidelines are shown as a flowchart of clinical practice. Green boxes indicate answers recommended, red boxes indicate answers not recommended, and white boxes indicate answers for background questions. CQ: clinical question; GPS: good practice statements; ECMO: extracorporeal membrane oxygenation; PP: prone position; OAM: open abdomen management; EE: energy expenditure
Fig. 3
Nutrition therapy for critically ill pediatric patients. Nutrition therapy for critically ill pediatric patients answered in the guidelines is shown as a flowchart of clinical practice. Green boxes indicate answers recommended, red boxes indicate answers not recommended, and white boxes indicate answers for background questions. CQ: clinical question; GPS: good practice statements; EE: energy expenditure; EN: enteral nutrition; PN: parenteral nutrition; FRQ: future research question
Table 1 Quick reference list of CQs and answersSince studies on nutritional treatment for critically ill patients are continuously reported worldwide, JCCNG 2024 will be revised in 4 to 6 years. When critical evidence is published, the GDG will discuss the necessity for revisions and will revise as needed.
Facilitators and barriers of applicationIn Japan, a new medical claim for early nutrition therapy has been introduced highlighting the importance of nutrition therapy for critically ill patients across numerous health care institutions, which will facilitate the application of JCCNG 2024. Conversely, the lack of designated dietitians in hospitals will hinder the clinical adaptation of recommendations in these guidelines. Therefore, the nationwide allocation of certified dietitians who support nutrition therapy needs to be promoted.
Conflicts of interest (COI) and fundsAll members of the GDG, working groups, systematic review teams, and a methodological support team declare their economic and academic COI in accordance with the COI Management Guidelines of the Japanese Association of Medical Sciences. The guidelines were developed with funds from the Japanese Society of Intensive Care Medicine, but do not reflect the intentions or interests of the society and no members received any compensation.
Methodology for the development of clinical practice guidelinesPrinciple of guideline developmentFollowing “Minds Manual for Guidelines Development 2020” [12], recommendations were drafted for each CQ based on the findings of a systematic review. Each recommendation was ultimately selected based on an evaluation of the balance between benefits and risks obtained by a systematic review, patients’ interests and conditions, medical economics, and social backgrounds.
CQ planning and classificationIn CQ planning, fundamental knowledge of nutrition therapy is thought to support physicians providing standard nutrition therapy for critically ill patients. Basic rules for CQ development include the following: (1) clinically important questions need to be selected regardless of high-quality evidence; (2) among CQs in the published international guidelines, questions requiring an updated search on and the collection and integration of evidence need to be selected; and (3) CQs need to be in the form of a question and presented in the Patients, Intervention, Control, and Outcome (PICO) framework if they are foreground questions (FQs).
CQs were classified into two categories: background questions (BQs) providing information rather than recommendations, and FQs providing recommendations (Table 2). The recommendations in FQs are further classified into two categories: GRADE recommendations developed based on evidence that is obtained by systematic reviews, and GPS selected by the GDG when the benefits of the intervention clearly outweigh its risks, a RCT is not ethically feasible, and the GDG decides to make a strong recommendation. FQs for which sufficient evidence was not obtained were shown as future research questions (FRQs), and no recommendation was made.
Table 2 Classification of a clinical questionCQs were allocated to four working groups: 1. General principles of nutrition therapy, 2. Specific nutrients in nutrition therapy, 3. Nutrition monitoring and specific conditions, 4. Nutrition therapy in pediatrics. Each working group prepared a draft of sentences for CQs, which was then approved by the GDG. PICO was confirmed by the same processes, in which the outcome of PICO was unified for all FQs. Details on the outcome adopted into PICO and its level of importance were selected by consensus of the GDG (Table 3).
Table 3 Basic outcomes adopted in JCCNG 2024Answers to BQs were described as an explanation of fundamental knowledge using published international guidelines, previous systematic reviews, and statements from academic organizations. GPS for FQs were developed by each working group, and GRADE recommendations were developed by a search for and the collection and synthesis of evidence using a systematic review and an evaluation of CoE.
Literature search and data extractionArticles were searched in CENTRAL, PubMed, and Ichushi, a database for Japanese articles, in April 2023, and those published until the day of the search were targeted. The search strategy was developed by the systematic review team using Medical Subject Headings terms and free search terms, and was supervised by the working group. Target articles were limited to RCTs written in English or Japanese. The search strategy was finalized after confirming that the predefined important articles were appropriately included. The date when the literature search was conducted and the number of papers searched in each database were recorded, and bibliographic information was obtained.
After excluding duplicates of the retrieved references, two or more members in the systematic review team independently conducted primary screening; references that matched PICO were screened from titles and abstracts using Rayyan (https://rayyan.qcri.org/welcome).
The secondary screening of the selected articles was independently conducted by two or more members in the systematic review team, in which the full text of the articles was obtained and eligibility based on the study design and PICO was evaluated. Any disagreements were discussed by a third member in the systematic review team or working group members. Reasons for exclusion were recorded in each step and summarized in a PRISMA flow diagram.
Data extraction and bias risk assessmentData extraction was performed by two or more members in the systematic review team using a standardized data extraction form. The study design, inclusion and exclusion criteria, the number of patients, interventions and controls, and outcomes were extracted for each study. No inquiries to the original authors were conducted.
The risk of bias was assessed by two or more members in the systematic review team. In each study and outcome, the risk of bias was assessed in five domains according to the RoB 2.0 methodology. The potential of bias was evaluated as high, low, or unclear, and the reason was noted for a high potential of bias. The risk of bias is summarized in the risk-of-bias table.
Meta-analysis and CoEA meta-analysis of extracted outcome data was performed using Revman 5. CoE, which encompasses the findings of a meta-analysis, was assessed for each outcome based on the GRADE approach. The risk of bias, indirectness, inconsistency, imprecision, and publication bias were evaluated, and CoE was then rated as high, moderate, low, and very low. The findings obtained were summarized as an evidence profile using Guideline Development Tool (GDT) online software (http://gdt.guidelinedevelopment.org). CoE was estimated as high, downgraded if there were serious limitations in each item, and ultimately classified into high, medium, low, and very low (Table 4).
Table 4 Definition of certainty of evidenceDevelopment of recommendations and consensus buildingBased on the evidence profile generated by the systematic review, the working group developed GRADE recommendations using the Evidence to Decision (EtD) table. This table evaluates benefits and risks, CoE, values and preferences, resources, acceptability, and feasibility, and the overall evaluation then selects a recommendation, which is either support or against and weak or strong. Classifications of the strength and CoE in each recommendation are shown in Table 5. Certainty of evidence for the recommendations is determined as the highest one among those for outcomes when either benefits or harms exist, whereas it is determined as the lowest one when both benefits and harms exist.
Table 5 Strength and certainty of evidence in each recommendationAll GRADE recommendations developed by these processes, as well as GPS and answers to BQs, were finalized by consensus building by the GDG. Consensus was confirmed using the modified Delphi method, in which each member of the GDG independently voted on each proposal on a scale of 1 to 9 (1: disagree, 9: agree). Voting was conducted anonymously, and members with a COI related to the relevant CQ and those directly contributing to the development of a recommendation for the relevant CQ abstained from voting. A median score ≥ 7 and a disagreement index < 0.4 were used as consensus criteria. In the case of a disagreement, the EtD table and recommendations were revised by the responsible working group and GDG member. Revisions and votes were repeated until the consensus criteria were met. Minor revisions to CQs were made by consensus of the GDG.
Relevant information for a recommendation based on GRADE in each working group (working group 1–4) was available at Additional file 1–4, respectively.
Terms in guidelinesNutrition therapy: A component of medical treatment that involves enteral and/or parenteral nutrition including oral nutrition.
Nutritional disorder: The state of an altered body composition and/or diminished function due to deficiencies, excesses, or imbalances of energy and/or nutrients.
Malnutrition: A condition where pathological symptoms appear due to quantitative or qualitative deficiencies in nutrients necessary for normal metabolism and development.
Overweight/obesity: A condition of excessive fat deposits; a body mass index (BMI) between 25 and < 30 kg/m2 is classified as overweight, between 30 and < 35 kg/m2 as obese, and ≥ 35 kg/m2 as severely obese. Morbid obesity is defined as obesity with health issues that are caused by or related to obesity, regardless of BMI.
Enteral nutrition : (EN). A system of providing nutrition by the intestinal tract, broadly including oral nutrition.
Enteral tube feeding: A system of providing nutrition via a tube or stoma into the intestinal tract distal to the oral cavity.
Parenteral nutrition (PN): The intravenous administration of nutrients, which may be provided by a central or peripheral venous line.
Supplemental parenteral nutrition (SPN): PN added to EN when EN alone is insufficient.
Gastric feeding: The administration of EN into the stomach via a nasogastric tube or gastrostomy.
Post-pyloric feeding: The administration of EN beyond the pylorus via a nasoduodenal or nasojejunal tube or jejunostomy.
Continuous feeding: The hourly administration of EN over 24 h assisted by a feeding pump.
Intermittent feeding: The administration of EN several times a day (for example, 2–4 times) over a period of time (for example, 1–3 h each).
1.General principles of nutrition therapy
CQ 1-1: Should nutrition therapy using nutrition protocols be provided in critically ill patients?
Answer: We suggest providing nutrition therapy using nutrition protocols to critically ill patients. (GRADE 2B: certainty of evidence = “moderate”).
Rationale
Critically ill patients are more likely to have difficulty achieving nutritional targets for energy and protein, and their nutritional supply is typically insufficient. Therefore, when providing nutrition therapy to critically ill patients, it is favorable to have a protocol that outlines criteria for the initiation of EN and PN, the administration methods for EN formulas, the use of specific nutritional products, and the management of enteral feeding intolerance (EFI) and gastrointestinal complications. The clinical benefits of nutrition administration protocols have been demonstrated, particularly those that improve target nutritional dosing [13]. However, it remains unclear whether the implementation of nutritional protocols improves patient outcomes; thus, it is important to clarify the effectiveness of nutrition therapy using these protocols.
A meta-analysis was performed using 2 RCTs and 4 cluster RCTs (Additional file 1) [14,15,16,17,18,19]. The results of the favorable outcomes were as follows: pneumonia yielded a risk difference (RD) of 16 fewer per 1000 (95% CI 65 fewer to 148 more) (2 RCTs, n = 576), dialysis days yielded an RD of 29 fewer per 1000 (95% CI 60 fewer to 2 more) (2 RCTs, n = 2970), and enteral nutrition initiation time yielded a mean difference (MD) of 0.4 days shorter (95% CI 0.6 shorter to 0.1 shorter) (6 RCTs, n = 3854). A slight effect was observed on mortality and length of ICU stay. Therefore, the favorable outcomes were judged as small. The results of the unfavorable outcomes were as follows: duration of mechanical ventilation yielded a standardized mean difference (SMD) of 0.3 longer (95% CI 0.2 shorter to 0.7 longer) (4 RCTs: n = 2173) and vomiting yielded an RD of 9 more per 1000 (95% CI 18 fewer to 65 more) (2 RCTs, n = 576). Therefore, the unfavorable outcomes were judged as trivial. Based on the overall balance of effects, we thought that nutrition therapy using nutrition protocols was likely superior.
A nutrition intervention is acceptable from a patient’s perspective because there is no additional cost to the patient for the intervention. It is included in the current requirements for a medical service fee and is considered acceptable under current practice. Additionally, the intervention does not necessitate new medical equipment required for the intervention, and it is acceptable from the perspective of management by the medical institution. Furthermore, the implementation of the protocol does not impose a significant workload on healthcare professionals. Based on the balance of these effects, we concluded that nutrition therapy using nutrition protocols was likely superior.
CQ 1-2: Should enteral nutrition be administered rather than parenteral nutrition in critically ill patients?
Answer: We suggest administering enteral nutrition rather than parenteral nutrition in critically ill patients (GRADE 2C: certainty of evidence = “low”).
Rationale
EN is generally thought to have the potential to reduce infectious complications in critically ill patients [20]. PN is more likely to cause hyperglycemia and overfeeding, which are associated with infectious complications [21], whereas EN has been shown to improve intestinal epithelial cell function [22, 23]. However, recent large-scale RCTs did not report an improvement in prognosis [24, 25]. EN was found to increase gastrointestinal complications, such as vomiting, diarrhea, and mesenteric ischemia [25, 26]. The choice of a nutrition delivery route is a crucial process in the nutrition therapy, and it is important to establish whether PN or EN is more favorable based on the findings of recent studies. Therefore, this CQ has been identified as an important clinical issue.
A meta-analysis was performed using 36 RCTs [24, 25, 27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] and secondary analyses of these RCTs (Additional file 1) [61,62,63,64]. The results of the favorable outcomes were as follows: length of ICU stay yielded an MD of 0.9 days shorter (95% CI 1.8 shorter to 0.1 shorter) (14 RCTs, n = 5431), duration of mechanical ventilation yielded an MD of 0.4 days shorter (95% CI 3.6 shorter to 2.7 longer) (5 RCTs, n = 268), sepsis (including bacteremia) yielded an RD of 28 fewer per 1000 (95% CI 37 fewer to 15 more) (15 RCTs, n = 5892), and pneumonia yielded an RD of 9 fewer per 1000 (95% CI 32 fewer to 19 more) (18 RCTs, n = 5943). Therefore, the favorable outcomes were judged as small. The results of the unfavorable outcomes were as follows: 90-day mortality yielded an RD of 20 more per 1000 (95% CI 8 fewer to 48 more) (3 RCTs, n = 4800) and mesenteric ischemia yielded an RD of 7 more per 1000 (95% CI 0 more to 22 more) (3 RCTs, n = 4861). Therefore, the unfavorable outcomes were judged as small. Based on the overall balance of effects, we thought that the favorable and unfavorable effects of enteral nutrition were balanced, leading to the conclusion that neither enteral nutrition nor parenteral nutrition was superior to the other.
To evaluate the balance of effects, we conducted three sensitivity analyses and three subgroup analyses. Sensitivity analyses included the following: “excluding studies that administered EN at the standard dose (20 kcal/kg/day) to hemodynamically unstable patients [24, 27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,
Comments (0)