
Remember me
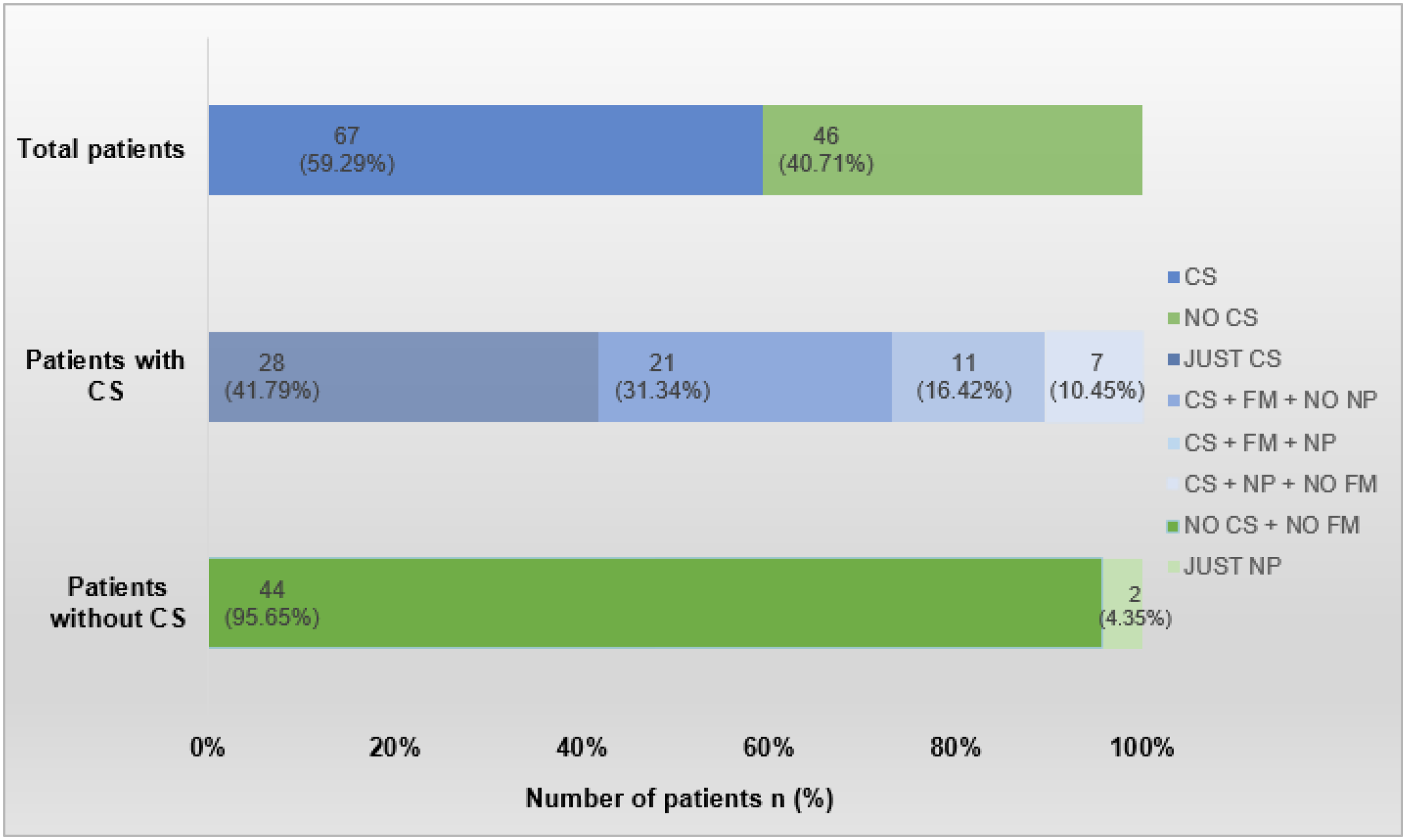

Our sample consisted of sixty-five children and adolescents with suspected MIS-C, hyperinflammation, or conditions associated with SARS-CoV-2 infection. Among these patients, 9 did not meet the criteria for suspicion due to other confirmed etiologies accounting for the inflammatory presentation (including cytomegalovirus infection, disseminated toxoplasmosis, tuberculosis, respiratory syncytial virus, sepsis from Enterococcus sp. and Klebsiella sp., invasive fungal infection, systemic juvenile idiopathic arthritis, and familial hemophagocytic lymphohistiocytosis) or because the duration of contact with COVID-19 was longer than 8 weeks (twice the duration considered for MIS-C suspicion). Of the sixty-five patients investigated, fifty-four were confirmed to have MIS-C (31 patients) or hyperinflammation (23 patients); 4 presented with symmetric peripheral neuropathy (Guillain-Barré Syndrome), with one case overlapping with hyperinflammation (Fig. 1).
Fig. 1
Patients’ median age was 74 months (IQR 22.5 to 116.8). Male patients accounted for 50% (27) of the cohort. Among the studied patients, 44% (24) were of normal nutritional status, 11% (6) were obese, and 7% (4) were severely obese. In the MIS-C group, the median age was 77 months (IQR 23 to 112.5), whereas in the hyperinflammation group, the median age was 72 months (IQR 18 to 131.5). No statistically significant differences were observed between the groups regarding age, sex, ethnicity, nutritional status, or known COVID-19 contact (Table 1).
Regarding exposure to known COVID-19 contacts, 56% (30) did not have identified contacts, while only 39% (21) could identify contacts, with 28% (15) being the patients’ own parents (Table 1).
In our sample, 67% (36) of patients had some form of comorbidity, with no statistically significant difference between the groups. The most frequent comorbidity was obesity, found in 19% (10) of patients. Among patients with hyperinflammation, the second most common comorbidity was cancer, affecting 26% (6 patients in this group), while in the MIS-C group, asthma was the second most common comorbidity, affecting 23% (7 patients in this group). Other comorbidities are detailed in Table 1.
Table 1 Demographic, anthropometric, social and comorbidity dataClinical aspectsIn our sample, 69% (37) of patients had a positive PCR-RT test, and 43% (23) had positive COVID serology. 100% (23) of the patients with hyperinflammation had a positive COVID RT-PCR, while it was positive in 45% (14) of the MIS-C group. Regarding serology, 68% (21) of the MIS-C group had a positive result, with 81% of these (17) showing only positive IgG (indicating previous COVID infection (Table 2).
Regarding clinical findings, the most frequent sign was fever present in 96% (52) of all patients. The frequency of symptoms varied according to the group analyzed, as detailed in Table 2. Altered mental status was observed in 61% (19 patients) of the MIS-C group and in 26% (6 patients - p = 0.014) of the hyperinflammation group. Cardiological symptoms were present in 48% (15 patients - p = 0.018) of the MIS-C group, and conjunctival hyperemia was noted in 29% (9 individuals - p = 0.032) of this group.
Aneurysms and serosal inflammation (serositis) were exclusive to patients with multisystem inflammatory syndrome. Arthritis and arthralgia were predominant in the MIS-C group but did not show statistical significance. In contrast, symmetric peripheral neuropathy (Guillain-Barré) was observed only in one patient in the hyperinflammation group.
Among our entire sample, 40% (22 patients) required supplemental oxygen, some with the need for ventilatory support. Specifically, 13% (7) required mechanical ventilation, 15% (8) required high-flow nasal cannula, 4% (2) required non-invasive ventilation, and 20% (11) required supplemental oxygen. Additionally, 38.9% (21) required admission to a pediatric intensive care unit, and 20% (11) required vasoactive drugs. The hyperinflammation group exhibited ventilatory dysfunction in 57% (13 children - p < 0.001) of patients, whereas 13% (4 children) had dysfunction in the MIS-C group.
Table 2 Diagnostic test and clinical dataThe most frequent laboratory findings in the MIS-C group was increased ESR (p = 0.001), triglycerides (p = 0.009), and fibrinogen (p = 0.03), as well as elevated troponin (p = 0.034), D-dimer (p = 0.015), and BNP (p = 0.02), and decreased albumin (p = 0.02) compared to the HI group. The hyperinflammation group exhibited a higher percentage of ferritin levels exceeding 500 ng/mL (p = 0.046) as shown in Table 3.
The median serum BNP level was higher in the MIS-C group, with a value of 126 pg/ml (IQR 30–770), compared to 17.5 pg/ml (IQR 10-102.3) in the hyperinflammation group (p = 0.048). Although other tests did not show statistical significance, the median levels of troponin and D-dimers were higher in the MIS-C group (Table 4).
Although there was statistical significance regarding the presence of elevated ESR, triglycerides, fibrinogen, troponin, D-dimers, and reduced albumin in the dichotomous analysis (presence or absence of the alteration), statistical significance was not maintained when analyzing the test values in our population.
Table 3 Presence of laboratory abnormalityTable 4 Laboratory valuesThe ROC curves were performed for the main tests (BNP, Troponin, D-dimer, and AST) and are detailed in Table 5; Fig. 2.
For BNP measurement, a value of 52.15 pg/mL was identified as the optimal cutoff for differentiating between the groups (AUC = 0.69), with a sensitivity of 72% and specificity of 67%. Troponin testing showed a cutoff point of 14.45 pg/mL with a sensitivity of 52% and specificity of 67%, while D-dimer testing demonstrated high specificity (81%) at a cutoff of 4.25 µg/mL. The test with the best sensitivity, despite an AUC of 0.59, was AST (aspartate transaminase) with a cutoff of 93 U/L, showing a sensitivity of 84% and specificity of 52%.
Fig. 2
The recommended treatment for inflammatory conditions associated with COVID-19 includes the use of glucocorticoids for both groups, and the use of immunoglobulin and aspirin (ASA) restricted to the MIS-C group.
Although glucocorticoids are considered the first-line treatment for both MIS-C and hyperinflammation, they were used in only 56% (30) of the sample, with 61.3% (19) of the MIS-C group and 47.8% (11) of the hyperinflammation cases receiving this treatment, with no statistically significant difference.
Regarding the use of intravenous human immunoglobulin, 74.2% (23) of the patients with MIS-C received the medication, with an average dosage of 2 g/kg. In contrast, only 17% (4) of the hyperinflammation group received immunoglobulin (all before the diagnosis of hyperinflammation), and this difference is statistically significant (p < 0.001). Regarding acetylsalicylic acid use, 61% (19) of the MIS-C group received this medication, while only 9% (2) of the hyperinflammation population used it due to the associated risk of thrombocytosis. This difference is also statistically significant (p < 0.001).
Among the patients analyzed, there were only three deaths, resulting in a mortality rate of 5.5% in the overall study population, with no statistically significant difference between groups. In our sample, there were two deaths in the hyperinflammation group among children with comorbidities (one with panhypopituitarism and another with severe asthma), while in the MIS-C group, the patient who died had primary bone marrow aplasia.
Comments (0)