
Remember me

Overall, the studies included were retrospective, had a non-comparative longitudinal design, with a high risk of bias and heterogeneity, and included persons from different geographic areas and epidemiological risks for TBD. In this way, all the recommendations provided here are conditional and health professionals must consider the epidemiological risk, individual factors, the social context, the characteristics of the disease, access to health resources, and the patient’s preferences to choose the ideal course of action for each patient at a given point in their treatment.
The recommendations generated in this document were established through consensus among the panelists, in which more than 80% of panelists voted for options 4—agree—and 5—strongly agree in all scenarios.
Table 3 summarizes the nine recommendations and corresponding CQs, whose search strategies provided the evidence used to develop each recommendation, the overall quality of evidence across all critical outcomes (assessed using GRADE), and the level of agreement (LOA) between panelists.
Table 3 Summary of recommendationsComplete references of all included studies as well as their main characteristics are available in the supplementary material (Appendix 2).
Recommendation 1. Routine investigation for TBI, and consequent TPT when indicated, should be carried out in all persons with IMID who will undergo immunosuppressive treatment, regardless of the class of drug chosen, if there is no recent history of treatment for TBD or TBI.
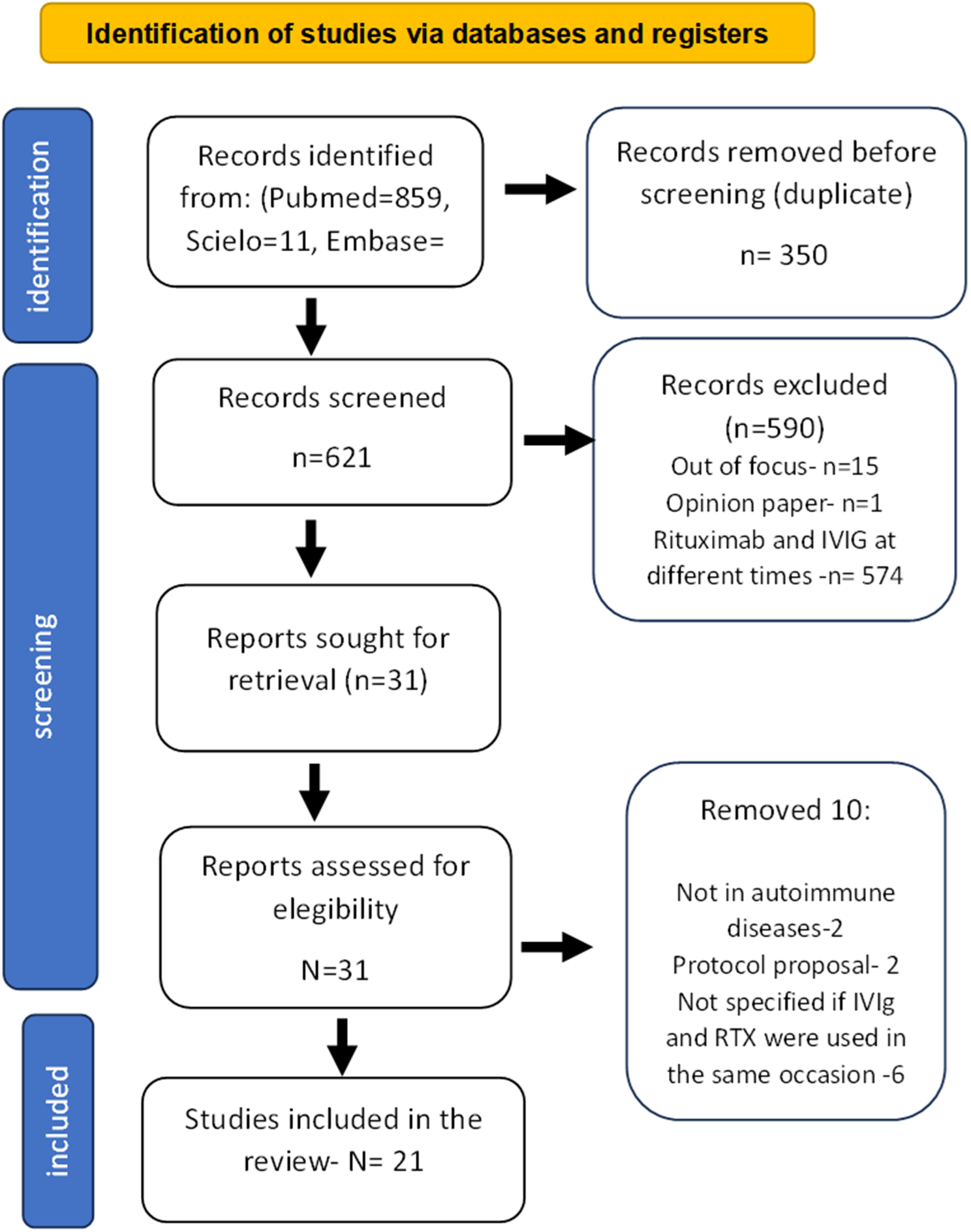
For this analysis, 10,713 reports were initially evaluated, with data from 17,246 patients. After exclusion, 124 studies were analysed.
The incidence rates (and 95% confidence intervals) of TBD in persons with IMID treated with the different classes of DMARDs extracted from the included studies were combined, determining an overall incidence rate of TBD in each of these groups. These pooled incidences are shown in Table 4.
The Incidence Rate Ratio (IRR) was used as the measure of effect to compare the incidence rates of TBD across different DMARD classes. The analysis was conducted using the general inverse variance (IV) method with a fixed-effects model.
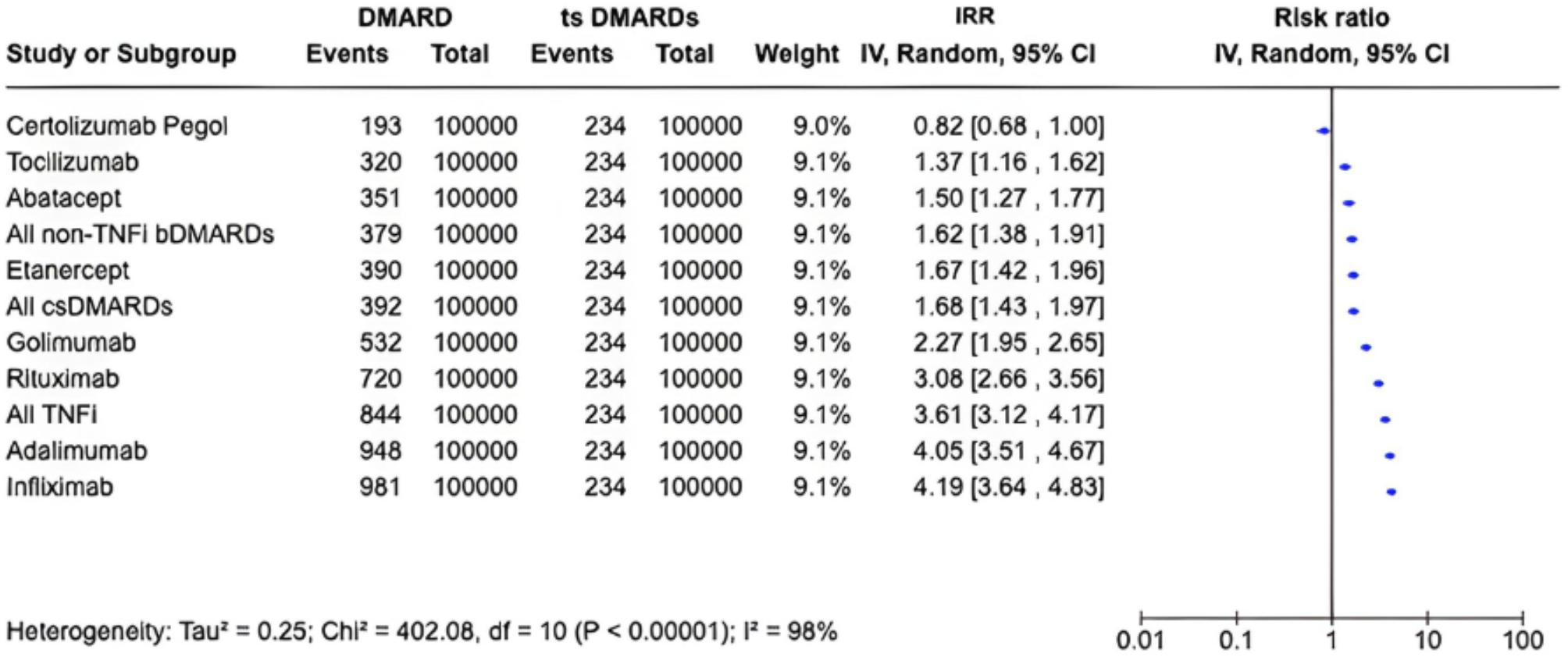
The tsDMARDs were the medications with the lowest incidence rates of TBD in persons with IMID, and were therefore, used as the main comparator concerning the other classes. Table 5 and Fig. 1 show the results of IRR of TBD in persons with IMID being treated with the different classes of DMARDs.
Table 4 Pooled incidences of TBD among IMID patients treated with different classes of DMARDsTable 5 Incidence rate ratio (IRR) of TBD in IMID patients being treated with the different classes of DMARDsFig. 1
Incidence rate ratio (IRR) of TBD in IMID patients being treated with the different classes of DMARDs
Although TNFi had an increased risk compared with non-TNFi, all bDMARDs increased the incidence of TBD.
TNFi users had a higher incidence rate of TBD than tsDMARD users, except for certolizumab, whose analyses were not statistically relevant. Adalimumab and infliximab increased the rates of TBD in a very similar way—an incidence approximately 2.5 times higher compared to users of tsDMARD.
Etanercept, adalimumab, infliximab, and golimumab considerably increased the rates of TBD in their users when compared to patients treated with certolizumab.
The other classes of DMARDs, when compared to tsDMARDs, showed varied results: rituximab users had a 1.8 times higher rate of TBD, while the risk among users of csDMARDs, tocilizumab, and abatacept did not seem to differ. Rituximab increased the risk of TBD by 2.2 times compared to patients receiving tocilizumab.
Although the statistical analyses point to a higher incidence of TBD among patients being treated with TNFi, especially infliximab and adalimumab, when compared to the other classes of DMARDs, the interpretation of these results must consider some critical limitations.
Some literature data corroborate these results from our systematic review. A recent study evaluated the occurrence of TBD as the primary outcome, with a follow-up of three years, in patients with RA from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis (BSRBR-RA), who initiated bDMARD from the first to fifth line of therapy between 2001 and 2019, but tsDMARDS were not included. A total of 33,897 treatment courses were included in this analysis, 10,643 with etanercept, 7,835 with adalimumab, 4,430 with infliximab, 1,614 with certolizumab, 5,556 with rituximab, 2,633 with tocilizumab and 1186 with abatacept, comprising 62,513 person-years of follow-up. There were 49 cases of active TBD during the study, with an incidence rate of 8.5 (95% CI 5.7, 9.9) per 10,000 patient-years. No cases were observed in the tocilizumab group. The crude incidence rates of active TBD were higher with adalimumab and infliximab than etanercept. The unadjusted HR (95% CI), with etanercept as the reference were 3.3 (1.4 to 7,8) for adalimumab, 3.4 (1.6 to 7.3) for infliximab, 1.6 (0,3 to 7.2) for certolizumab, 0.2 (0.0-1.4) for rituximab and 1.2 (0.1–9.4) for abatacept. It is not recorded whether patients in the BSRBR-RA had received TPT prior to starting bDMARDs [22].
The anti-cytokines IL-17, IL-12 and IL-23 bDMARDs are not mentioned in our review because the studies retrieved contained a small number of cases of TBD in persons with IMID treated with these drugs, making comparisons with other DMARDs difficult.
In line with our findings, the Skin Inflammation & Psoriasis International Network–Fondation René Touraine (SPIN-FRT) has published a recommendation for the treatment of psoriasis with bDMARD and tsDMARD in psoriasis patients with TBI or at risk for TBD progression. This task force highlighted that IL-12/23, IL-17, IL-23, and TYK2 inhibitors have different mechanisms of action related to TNFi, and current evidence suggests that some of these agents are arguably not associated with an increased risk of TBD reactivation. They identified, with limited evidence, a low TBD incidence with IL-17 and IL-23 inhibitors in this population and prompted the need for updates to the existing guidelines [23].
The evidence regarding the risk of TBD associated with the use of tsDMARDs in IMID, suggests that this risk may be lower compared to other immunosuppressive therapies, like TNFi, probably due to a more selective mechanism of action, as they inhibit specific cytokine signaling pathways (JAK-STAT pathway), such as IL-6, IL-23, and interferon-gamma, which are involved in the inflammatory response. This low incidence was observed in clinical trials with these medications and also in real-life studies [24].
Various studies have shown an increased risk of TBD with the use of bDMARDs or csDMARDs. This is probably due to T cell dysfunction and depletion, changes in cytokines, complement dysfunction, and metabolic abnormalities [25,26,27]. A recent Chinese study has evaluated 270 patients with rheumatic diseases which developed TBD from 2009 to 2022. Based on the medication used for rheumatic immune diseases before TBD, the patients were divided into three groups: bDMARDs, which included the use of TNFi, IL-17 and IL-6 inhibitors, abatacept, and B-cell targeted therapies; no immunotherapy group, with patients who did not receive these drugs to treat their rheumatic disease, and the csDMARDs group, that included the use of sulfasalazine, methotrexate, leflunomide, azathioprine, cyclophosphamide, and corticosteroids. There were 31 cases of TBD in the bDMARDs group, 98 cases in the no immunotherapy group, and 141 cases in the csDMARDs group. The bDMARDs group had more extrapulmonary TBD and the csDMARDs group more cavitations [28].
Some important aspects should be considered. Firstly, we highlight the low quality of the evidence gathered through the literature search. Most of the studies selected in this analysis are retrospective, non-comparative longitudinal studies with a high risk of bias, factors which significantly influence the strength of the recommendations resulting from their analysis.
There is a publication bias regarding TNFi compared to the other classes of DMARDs. This can be explained by the fact that many of the studies included were conducted more than a decade ago, when this class of drugs was widely used and was, therefore, the focus of the publications. Thus, we observed a disproportion in the number of studies on TNFi compared to the other medications.
Many of the included studies do not discriminate whether there has been TPT or treatment of active TBD before the analysis of TBD occurrence, thus it is impossible to assess the impact of these critical factors on the incidence rates of this disease.
Another important point is that the search did not retrieve studies that assessed the risk of TBD independently with the various csDMARDs, as well as immunosuppressants, according to the classes of medications listed in Table 1. The studies evaluated these classes in combotherapy with bDMARDs or tsDMARDs, therefore, it was not possible to assess the risk of each of these classes independently.
Finally, the studies were carried out in different geographical regions, with different population incidence rates of TBD and, therefore, different epidemiological risks of developing this infection, regardless of the underlying disease or the use of the different classes of drugs.
These facts altogether result in a high degree of heterogeneity in the analysis and reduce the strength of the recommendation.
We conclude that, despite an extensive database search and the examination of around 10,000 titles, the existing literature does not allow us to differentiate, with a reasonable degree of statistical certainty, the risk of TBD in patients with IMID being treated with the different classes of DMARDs. However, as the risk of developing TBD is higher in patients with IMID taking DMARDs [8], we conditionally recommend that TBI screening should be carried out in all patients taking DMARDs, regardless of class, especially in Brazil and other countries with high TBD incidence rates.
LOA: 67.5% Strongly agree; 27.5% Agree. Sum of the percentage of “Strongly agree” and “Agree”: 95%. Overall quality of evidence across all critical outcomes: Very low.
Recommendation 2. TBI diagnosis should be considered and TPT indicated in any the following situations: TST ≥ 5 mm; a positive IGRA; signs of lung TBD sequelae in imaging tests (chest X-ray or CT) in the patient not previously treated for TBD; recent exposure to pulmonary or laryngeal TBD, if there is no clinical, and/or imaging evidence of TBD.
In persons with IMID, including candidates for TNFi treatment, a combined approach based on immunological tests, clinical history, chest X-ray, or computed tomography (CT) scan casual findings can be helpful for the indication of TPT [1].
There is no gold standard test for TBI diagnosis. The TST/IGRA results, the presence of TBD sequelae in imaging studies (chest X-ray or chest CT scan), and known exposure to an index patient with active pulmonary or laryngeal TBD should be considered for the diagnosis of TBI.
The use of TNFi therapy and other classes of DMARDS increases the risk of TBD, and this risk can be substantially reduced with rigorous TBI screening and TPT [1].
Both TST and IGRA have advantages and limitations. Both tests can be used for TBI evaluation in persons with IMID, as in other indications. TST cut-off for persons using DMARDs should be 5 mm [1]. There is insufficient evidence to recommend reducing the TST cutoff below 5 mm in IMID patients [29,30,31,32,33]. As for IGRA tests, positivity is considered as by the manufacturer’s recommendations.
Chest X-ray is needed before starting DMARDs. Chest X-ray demonstrating any sign of TBD sequelae such as fibrotic sequelae, calcified nodules in the upper lobe, apical pleural thickening, upper lobe bronchiectasis, interstitial granulomatous calcification, cavitation, and lymph node or pericardial or pleural calcification in a person not previously treated for TBD indicates TBI and TPT should be offered, even in the absence of a positive TBI test [1].
CT scans are not routinely recommended in the screening of TBI, if a chest X-ray is available, but casual findings of the same TBD sequelae in CT scans performed for other reasons in persons using DMARDs should prompt TPT prescription, regardless of TBI test results [1].
In cases of confounding images or in the presence of interstitial lung disease, pleural effusion or something that compromises the accuracy of the X-ray, a chest CT scan should be requested, as well as a specialist opinion (pulmonologists/infectious diseases specialists) [1].
History of known recent exposure (less than two years), to persons with pulmonary or laryngeal TBD, defined as present or past household or close community contact with known cases of TBD in the past two years in persons using DMARDs, should be considered as high-risk for TBI and TBD, and TPT should be indicated [1].
Household contact is someone who shares the same enclosed living space with the index case for one or more nights or frequent/extended daytime periods during the three months before the start of the current treatment [29,30,31,32].
A close community contact is a person who is not in the household but shares an enclosed space, such as a social gathering place, workplace, school or facility, for extended periods during the day with the index case, during the previous three months [29,30,31,32].
In summary, this committee recommends that TPT should be offered in the presence of at least one of the following: positivity of TST or IGRA, signs of TBD sequelae in lung imaging tests or history of recent TBD exposure.
LOA: 82.5% Strongly agree; 17.5% Agree. Sum of the percentage of “Strongly agree” and “Agree”: 100%. Overall quality of evidence across all critical outcomes: Very low.
Recommendation 3. In case TST/IGRA are not available:
-Persons with previous history of TBI/TBD treatment: once TBD is excluded, TPT is not mandatory, even in the absence of a TBI test.
-Persons with no history of TBI/TBD treatment: once active TBD is excluded, TPT should be recommended in a shared decision with the patient, regardless of the class of medication to be used.
In a scenario where tests for diagnosing TBI (TST and/or IGRA) are unavailable, if the patient has already undergone treatment for TBI or TBD previously, there is no indication to treat TBI again. If TBI/TBD has not been previously treated, TPT should be recommended if the tests are unavailable, in a shared decision with the patient since TBD is excluded, regardless of the class of medication to be used. In both situations, it is important to consider chest image exams and patient’s epidemiology.
Although there is evidence of an increased risk of developing TBD in persons treated with bDMARDs or other immunosuppressive drugs with a positive TBI test compared to those with a negative test, there is no evidence of the risk in persons without the test results [6, 33,34,35].
According to the Brazilian Society of Rheumatology, patients with RA, when using bDMARDs, with a negative history of contact with a case of pulmonary TBD should receive TPT if both tests (TST/IGRA) are unavailable. The decision to treat TBI should be individualized and consider risks and benefits. When assessing the potential benefit of treatment, consider increased epidemiological risk (high disease burden in the living environment) and synergy of risk factors for progression to TBD [36].
Because of the high risk of disease in high transmission settings in immunosuppressed persons, we extrapolate the WHO recommendations for people living with HIV [2] and recommend treating all persons who will be prescribed immunosuppressive drugs, regardless of the class, especially those who have had recent contact (within two years) with a person with active pulmonary or laryngeal TBD if a TBI test is not available, after excluding TBD with symptom screen and a chest image exam, in a shared decision with the patient.
LOA: 60% Strongly agree; 35% Agree. Sum of the percentage of “Strongly agree” and “Agree”: 95%. Overall quality of evidence across all critical outcomes: Low.
Recommendation 4. Both TST and IGRA can be used to diagnose TBI in IMID persons, since there is no gold standard test for diagnosing TBI in clinical practice.
IGRA and TST are recommended as screening methods for TBI, along with epidemiological risk assessment, and radiographic evaluation [37].
The TST includes a mixture of precipitated proteins from mycobacteria culture, being less specific to Mycobacterium tuberculosis when compared to IGRA, that is driven for more specific peptides (ESAT-6 and CFP-10), which are not present in the bacillus Calmette–Guérin (BCG) vaccine, neither in most of the other non-tuberculous mycobacteria. However, it is necessary to consider the prevalence of TBI in every country for a more suitable interpretation. Thus, IGRA may be indicated as a feasible option for TBI screening [37].
Both IGRA and TST may present false negative results due to anergy related to immunosuppression, particularly in those with RA, PsA and IBD using DMARDs. Thus, a negative TBI screening test does not entirely rule out the possibility of TBD after DMARD exposure over time [38, 39].
TST may have limited specificity because previous contact with other mycobacteria and BCG vaccination may influence the results. Likewise, immunosuppression, performance or incorrect reading of the test can affect sensitivity. TST performance by an experienced professional is recommended to avoid variability in interpretation. On the other hand, IGRAs also have limitations and its sensitivity may be reduced in immunosuppressed persons and in children. The rate of indeterminate results has been reported to be up to 40%. These findings challenge previous evidence that IGRA may be more suitable than TST in the immunocompromised host, as the immunosuppressant causes a significant reduction in the number of T cells that are essential for the release of adequate levels of IGRA. Furthermore, several studies have suggested very different concordance rates between IGRA and TST, likely due to heterogeneity (e.g., TBD prevalence, varying immunosuppressive therapies, or underlying BCG status) [38, 39].
Comparing TST and IGRA in persons with IMID is complex, considering that there is no gold-standard tool for diagnosing TBI, the test prevalence varies worldwide and the influence of the degree of immunosuppression of these patients that may occur [38, 39].
Therefore, both tests can be used to assess TBI, depending on the availability and specific characteristics of each patient. The healthcare professional must consider the limitations of each test when interpreting the result.
Table 6 summarizes the sensitivity and specificity of the tests in IMID, which resulted from our literature review. The analysis was carried out using either positive test as a gold standard reference. There was no superiority between them.
Table 6 The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of TST and IGRA having either test positive as the golden standardLOA: 80% Strongly agree; 20% Agree. Sum of the percentage of “Strongly agree” and “Agree”: 100%. Overall quality of evidence across all critical outcomes: Moderate.
Recommendation 5. When screening for TBI in persons with IMID, it is neither mandatory nor recommended to perform TST and IGRA tests simultaneously, and immunosuppressive treatment should not be postponed in order to perform both tests. If the first test is negative, the other can be considered. TPT should be started at any time if one of the tests is positive.
The studies included in this analysis showed a heterogeneous prevalence of TBI (29%, ranging from 6 to 48%). The discordance rate between both classes of tests was high. Without a gold standard test, the analysis of the diagnostic performance of each of the tests, IGRA and TST, was carried out considering the other test as a reference. According to this analysis, using both tests simultaneously increased the chance of diagnosing TBI by 20%, as shown in Table 7.
Table 7 Performance analysis regarding TST or IGRA for the diagnosis of TBI, considering as reference the other test, in the absence of gold standard methodDespite this increment, performing both tests is not mandatory or recommended, and the treatment of the underlying IMID should not be delayed. According to statement 4, either of the tests, TST or IGRA, can be used for TBI diagnosis.
LOA: 62.5% Strongly agree; 35% Agree. Sum of the percentage of “Strongly agree” and “Agree”: 97,5%. Overall quality of evidence across all critical outcomes: Moderate.
Recommendation 6. In the event of an indeterminate IGRA test result, it is recommended to repeat the test as soon as possible. If the result remains inconclusive, consider TPT.
The observational studies included in this analysis showed a wide range of IGRA indeterminate results, from 2.1 to 31.5%. Some disease and treatment-associated factors, as well as methodological issues may have contributed to an indeterminate IGRA result, such as living in an endemic area for TBD, glucocorticoid and other immunosuppressive treatments, disease activity, older age, low serum protein and albumin, lymphopenia, and high C-reactive protein (CRP) levels [40,41,42,43,44,45,46,47,48].
In one study with 190 IBD patients, indeterminate IGRA occurred in 26 patients (13.7%). All 26 patients with indeterminate IGRA had a negative TST. Twenty-four of 26 patients received TNFi, with no cases of TB [44, 45]. At the same time, there were also controversial TBD outcomes related to an indeterminate IGRA, corroborating the present recommendation to repeat the test as soon as possible and consider TPT if the test remains inconclusive [40,41,42,43,44,45,46,47,48].
LOA: 62.5% Strongly agree; 35% Agree. Sum of the percentage of “Strongly agree” and “Agree”: 97,5%. Overall quality of evidence across all critical outcomes: Moderate.
Recommendation 7. If the pre-treatment TST/IGRA test is negative, annual repetition of the test is recommended until the third year of treatment, especially in IMID patients taking TNFi. After this period, clinical and epidemiological surveillance is recommended during the immunosuppressive treatment, regardless of the class. In persons with a previous history of treatment for TBI or TBD, screening should not be repeated.
In the studies included in this analysis, all the patients had negative TBI tests (TST and/or IGRA) at baseline. The mean conversion rate after TNFi exposure was 12.8% over a mean time of 12.4 months (95% CI 8.8–17.4 months). Of patients who converted, 4% developed TBD. However, no prospective randomized clinical trials or observational cohorts demonstrated the effectiveness of different intervals for TST/IGRA conversion and incident TBD as the primary outcome related to the use of the different classes of DMARDs.
TBD diagnosis occurs early (less than three years after starting DMARDs, mainly TNFi) in most patients. Jauregui-Amezaga evaluated the risk of developing TBD in IBD patients under TNFi treatment, despite TBI screening. During the study period, 423 patients received TNFi therapy. Screening for TBI before TNFi treatment was positive in 30 patients (6.96%). Seven patients (1.65%) developed TBD while under TNFi treatment. In 4 of these patients, TBD was diagnosed within the first 16 weeks after starting TNFi therapy [33].
There is no consensus on the ideal timing for repeating TBI tests or how many times it should be performed. Although robust data on the effectiveness or cost-effectiveness of this strategy in clinical practice has yet to be collected, the ACR/EULAR has guided the annual repetition of the tests during TNFi/immunosuppressive treatment [49]. The Brazilian Ministry of Health recommends repetition of the test one year after the introduction of the immunosuppressive treatment, if the initial tests were negative [7].
Some aspects should be considered regarding this issue. The studies have heterogeneous results, such as different IMIDs (RA, axial SpA, PsA, vasculitis, juvenile idiopathic arthritis, PsO, and IBD), sample size, and follow-up time. The TST conversion rate may vary among IMIDs because of different pathophysiological characteristics, signaling pathways of the diseases themselves, impairment of cellular response, including anergy, and the different doses and classes of DMARDs and glucocorticoids. Finally, there is a lack of information regarding therapeutic measures introduced after the TST conversion rate, concerning TBD diagnosis, in the context of switching among biological DMARDs (TNFi versus non-TNFi), and TNFi discontinuation.
Two main hypotheses could better explain the higher positivity regarding the TST conversion rate after exposure to DMARDs. The main reason is that it would be directly related to re-exposure or new contact with the bacillus, since patients were previously negative and became positive with repetition. In this case, we would expect the frequency of TBD to increase over time, but most cases occur in the first 1–3 years, even in screened patients. Moreover, it could also be associated with an improved cellular response after immunosuppressive treatment, as well as reduction of glucocorticoid dosage and better control of disease activity with DMARDs [50, 51].
Indiscriminate repetition generates higher direct and indirect public health costs, especially in countries with cyclical shortages of TST. Therefore, prospective observational studies and randomized controlled clinical trials are needed to better define the effectiveness of repeating the TST.
This committee recommends the annual repetition of TST/IGRA during the first three years of DMARD treatment, mainly with TNFi. If either of the tests is positive, TPT should be carried out. After this period, clinical and epidemiological surveillance is recommended.
LOA: 32.5% Strongly agree; 52.5% Agree. Sum of the percentage of “Strongly agree” and “Agree”: 85%. Overall quality of evidence across all critical outcomes: Moderate.
Recommendation 8. In IMID, if it is necessary to change the medication, regardless of the class, if there is a previous negative TBI screening, TST/IGRA should be performed annually for the next 3 years, according to recommendation 7.
There is a lack of information regarding TST or IGRA repetition when a specific therapeutic decision needs to be made, due to inadequate response or side effects related to current treatment. Some aspects must be considered, such as disease activity and severity, comorbidities, concomitant medication, and other safety aspects. Moreover, some details could interfere with the need to rescreen patients for TBI diagnosis, such as the baseline result of the tests, time since the first screening, preventive measures implemented, and the order of bDMARDs used [50, 51].
For patients with positive baseline screening and adequate proven treatment for TBI, the repetition of TST or IGRA is not necessary. Similar recommendations may be made for those with a previous history of TBD who were adequately treated [1].
Considering the TST/ IGRA conversion rate in IMIDs during immunosuppressive therapy, the repetition might be considered in patients with negative baseline screening who need to
Comments (0)