Trial design
This was a prespecified sub-study of the PULSE-MI trial (Prehospital Pulse Glucocorticoid Therapy in Patients with ST-Segment Elevation Myocardial Infarction). The trial was a blinded, placebo-controlled, randomized clinical trial investigating the cardioprotective effect of prehospital pulse-dose glucocorticoid in patients with STEMI transferred for primary PCI [13]. The trial was conducted at the Department of Cardiology, Rigshospitalet, Denmark and all patients were randomized in the prehospital setting by the Emergency Medical Services in Region Zealand and Capital Region of Denmark. The trial was registered at https://clinicaltrials.gov (Unique Identifer: NCT05462730) and approved in the Clinical Trials Information System (EU-CT number: 2022–500762-10–00) and by the Danish Data Protection Agency (ID: P-2022–280). The trial protocol and primary results have previously been published [13, 14]. The trial was conducted in compliance with the Helsinki Declaration, European and national laws. The conduct of the trial was monitored by the Good Clinical Practice unit of Copenhagen, Denmark and monitored for safety and efficacy by an independent Data and Safety Monitoring Board. All patients provided informed consent following the acute treatment according to European law [13].
Patients
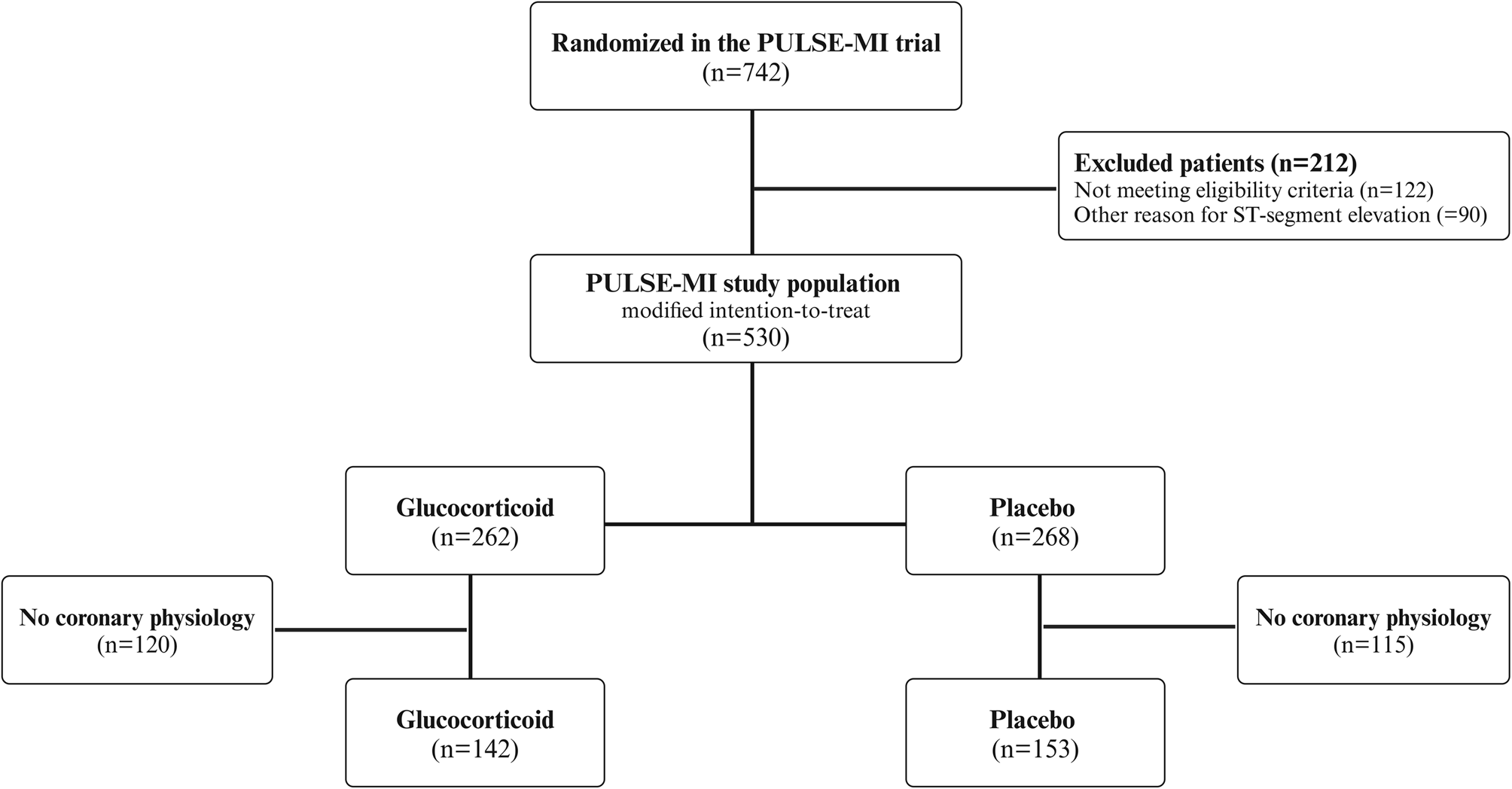
Between November 2022 and October 2023, patients with STEMI [1], aged ≥ 18 years and < 12 h of symptoms were randomized and treated in the ambulance prior to acute coronary angiogram. Main exclusion criteria were out-of-hospital cardiac arrest, previous acute myocardial infarction in assumed culprit, and a history of maniac/psychotic episodes. The full list eligibility criteria and study design have been published [13]. Of 742 randomized patients, 530 patients with STEMI were included in the modified intention-to-treat population [14].
Intervention and randomization
Patients were randomized in the prehospital setting to a single injection of methylprednisolone 250 mg (2 × 125 mg/2 mL) (glucocorticoid group) or placebo (0.9% NaCl 4 mL). The study medicine (active or placebo) was administered as a bolus injection over a period of 5 min as soon as the patient was accepted for an acute coronary angiogram at Rigshospitalet. Randomization was done using a random number generator with allocation in a 1:1 ratio. All ambulances throughout Region Zealand and Capital Region of Denmark were equipped with identical, opaque study medicine boxes, each numbered randomly according to allocation. Prehospital study medicine was administered by the ambulance staff who was blinded when randomly picking a study medicine box. The treating ambulance staff was unblinded after opening the box. All in-hospital personnel, trial investigators, and the patients were blinded for treatment allocation. All patients included in the trial were otherwise treated according to guidelines and standard procedures [1].
Outcome measures and objectives
This prespecified sub-study encompassed patients with invasive coronary physiology assessment following primary PCI. The objective was to determine the effect of prehospital pulse-dose glucocorticoid compared with placebo on the microcirculation determined by IMR in the culprit artery following primary PCI. Moreover, we sought to investigate the relation between microvascular function and randomized treatment using CMR, intracoronary physiology, and inflammation using C-reactive protein (CRP) levels.
Coronary physiology
Coronary physiology was assessed in eligible patients at the discretion of the operator and was assessed immediately following primary PCI. Coronary physiology was performed during all hours and during weekends. The theoretical basis of the physiological thermodilution-derived indices have been published elsewhere [15]. In brief, thermodilution-derived indices were measured by a pressure/temperature gauge guidewire (PressureWire X; Abbott) and data from the guidewire were analyzed with dedicated software (CoroFlow v.3.01; Coroventis). Equalization of the wire pressure and aortic pressure was done with the pressure sensor positioned at the tip of the guide catheter after it was secured that damping was not present. The wire was subsequently advanced to the distal third of the vessel. The mean transit time (Tmn) was calculated from the thermodilution curves by bolus injections of room temperature saline (3 mL) at rest and during maximal hyperemia. The Tmn was measured three times at rest and during maximal hyperemia, and the average Tmn was calculated by the computer in each physiological state. The software automatically marked any recordings of Tmn, deviating with more than 30% from the average value. If a recording was marked, the measurement for the specific recording was repeated. A two-minute infusion of adenosine (140 µg/kg/min) in a large vein was used to induce maximal hyperemia. IMR, reflecting the minimal microcirculatory resistance, was defined as the mean distal pressure multiplied by Tmn during maximal hyperemia [5].
Blood samples and cardiac magnetic resonance
CRP was collected upon admission by arterial blood samples. Between 12 and 36 h of symptom debut, CRP was collected using venous blood samples and the sample closest to 24 h was used for all analyses in this sub-study.
The CMR protocol and analyses has been described [13]. In brief, patients underwent two CMR scans, one during admission and three months after STEMI. This sub-study only included CMR outcomes of the acute scan, as glucocorticoid improved acute CMR outcomes in the primary analysis. Infarct size was measured by late gadolinium enhancement on short axis images performed 6–10 min following contrast infusion using a 5 standard deviations (SD) threshold of visually identified remote healthy myocardium on each short axis slice [16]. Microvascular obstruction was defined as hypointense areas within the infarct region [17]. T2*-images prior to contrast injection were used to identify intramyocardial hemorrhage defined as either hypointense regions within the infarcted area with mean T2*-value > 2 SD below T2*-value of remote healthy myocardium [18], or T2*-value within the infarcted area of ≤ 20 [19]. All quantitative analyses were performed in circle cardiovascular imaging (CVI42) by a reader blinded to clinical data.
Statistical analysis
Continuous variables were presented as mean (SD) if parametric and median (interquartile range (IQR)) if non-parametric. Categorical variables were presented as numbers and percentages. To investigate differences between groups, the Wilcoxon Rank sum test was used for numeric variables and Chi-square or Fishers test for categorical variables, as appropriate.
Box plots showing distributions of CRP at 24 h and IMR in the glucocorticoid and placebo group were conducted. Linear regression was used to investigate the relation between both IMR and CRP at 24 h, and treatment allocation. Logarithmic transformation was used to improve normality. Interaction analysis with culprit artery was performed to elucidate the potential difference of IMR in the treatment arms according to culprit artery. Interaction analysis between IMR and CRP at 24 h according to treatment arm was performed to elucidate the relation between microvascular damage and inflammation. To investigate the microvascular function and inflammation in relation to CMR outcomes according to treatment arm, interaction analyses between IMR, CRP, and CMR outcomes (acute and final infarct size, microvascular obstruction, intramyocardial hemorrhage, left ventricular ejection fraction) were performed. In all interaction analyses, linear regression was used for numeric outcomes, whereas logarithmic regression was used for binary outcomes.
As judged by the operator, not all patients had coronary physiology assessed. To investigate potential differences between these patients and those with coronary physiology, a baseline table stratified by coronary physiology assessment was conducted.
IMR and CMR outcomes were assessed in patients with and without pre-infarction angina in the treatment groups. Pre-infarction angina was defined as episodes of chest pain < 48 before symptom onset.
The P-values were two-sided and considered statistically significant if less than 0.050. All statistical analyses were performed in R Studio, version 4.3.2 (RStudio Team [2020]. RStudio: Integrated Development for R. RStudio, PBC, Boston, MA; URL: http://www.rstudio.com/).





Comments (0)