This study examined the relationship between venous bicarbonate levels and survival outcomes among patients with OHCA presenting in the ED. We found that a venous bicarbonate threshold of ≥ 12.6 mmol/L is associated with survival in these patients. The sensitivity of this marker was 74%, with a specificity of 47%, and it demonstrated an 88% negative predictive value for survival. These findings underscore the potential utility of bicarbonate levels as a prognostic tool, although the low specificity limits its efficacy in definitively ruling out non-survivors.
Bicarbonate (HCO3) serves as the principal buffer in the human body’s acid-base regulation system. Sodium bicarbonate is commonly administered to treat severe metabolic acidosis in critically ill patients, including those experiencing cardiac arrest, although its use remains a subject of ongoing debate [9, 10]. Our study examines the utility of bicarbonate in a different context, assessing its prognostic value rather than its therapeutic role in emergency medical situations. We found that higher initial bicarbonate levels (≥ 12.6 mmol/L) are significantly correlated with improved survival to hospital discharge in patients with OHCA. This finding aligns with previous research. Torres et al. [11] analyzed venous blood at the scene of OHCA and found minimal difference in bicarbonate levels between patients with and without ROSC (22.55 vs. 22.31 mmol/L), while Lopez-Sobrino et al. [12] observed lower bicarbonate levels in their study, with a wider differentiation between survivors and non-survivors (18.48 vs. 13.93 mmol/L). These discrepancies may be partially explained by the time interval between cardiac arrest and venous blood analysis, suggesting that ongoing cardiac arrest may intensify metabolic acidosis [2, 4, 5].
Furthermore, our study identifies a cutoff point of 12.6 mmol/L for bicarbonate, which demonstrates a notable negative predictive value of 88%. This finding suggests its potential utility in identifying patients at higher risk of mortality when bicarbonate levels fall below this threshold. However, this value is lower than the range found in previous studies (16.5–21.0 mmol/L) [12, 13]. This variation may be due to the fact that optimal thresholds can differ depending on healthcare setting and patient demographics. For instance, a previous study conducted in Srinagarind Hospital noted that the time from cardiac arrest to the initiation of CPR was relatively long (median 18 to 20 min) [13], which could influence bicarbonate levels and affect the optimal threshold for predicting outcomes.
Upon closer examination of patients with bicarbonate levels below 12.6 mmol/L, a notable distinction emerged in the presumed causes of cardiac arrest. Conditions characterized by a gradual onset, such as electrolyte abnormalities and gastrointestinal bleeding, were significantly more prevalent compared to patients with bicarbonate levels above 12.6 mmol/L. Conversely, presumed causes of cardiac arrest associated with a sudden onset, such as myocardial infarction and stroke, exhibited a significantly lower incidence in patients with bicarbonate levels below 12.6 mmol/L. This divergence may be attributed to an extended no-flow time in conditions with more gradual onset, potentially delaying the detection and resuscitation of the arrest, thereby exacerbating anion accumulation. This accumulation, in turn, contributes to the reduction of bicarbonate levels, aligning with existing literature that highlights the impact of prolonged no-flow time on acid-base balance [8].
We also found that patients with respiratory problems were more likely to exhibit higher bicarbonate levels, a phenomenon indicative of compensatory mechanisms for respiratory acidosis. This physiological compensation underscores the intricate interplay between respiratory and metabolic factors in influencing bicarbonate levels [14].
Our study also reaffirms the importance of a multifactorial approach to OHCA prognostication and management by identifying additional predictive factors for survival. These include elevated BUN levels (≥ 19.5 mg/dL), lower potassium levels (< 5.1 mmol/L), private transport, and specific initial cardiac rhythms. This aligns with findings from previous studies and emphasizes the need for holistic assessment to optimize outcomes [15, 16].
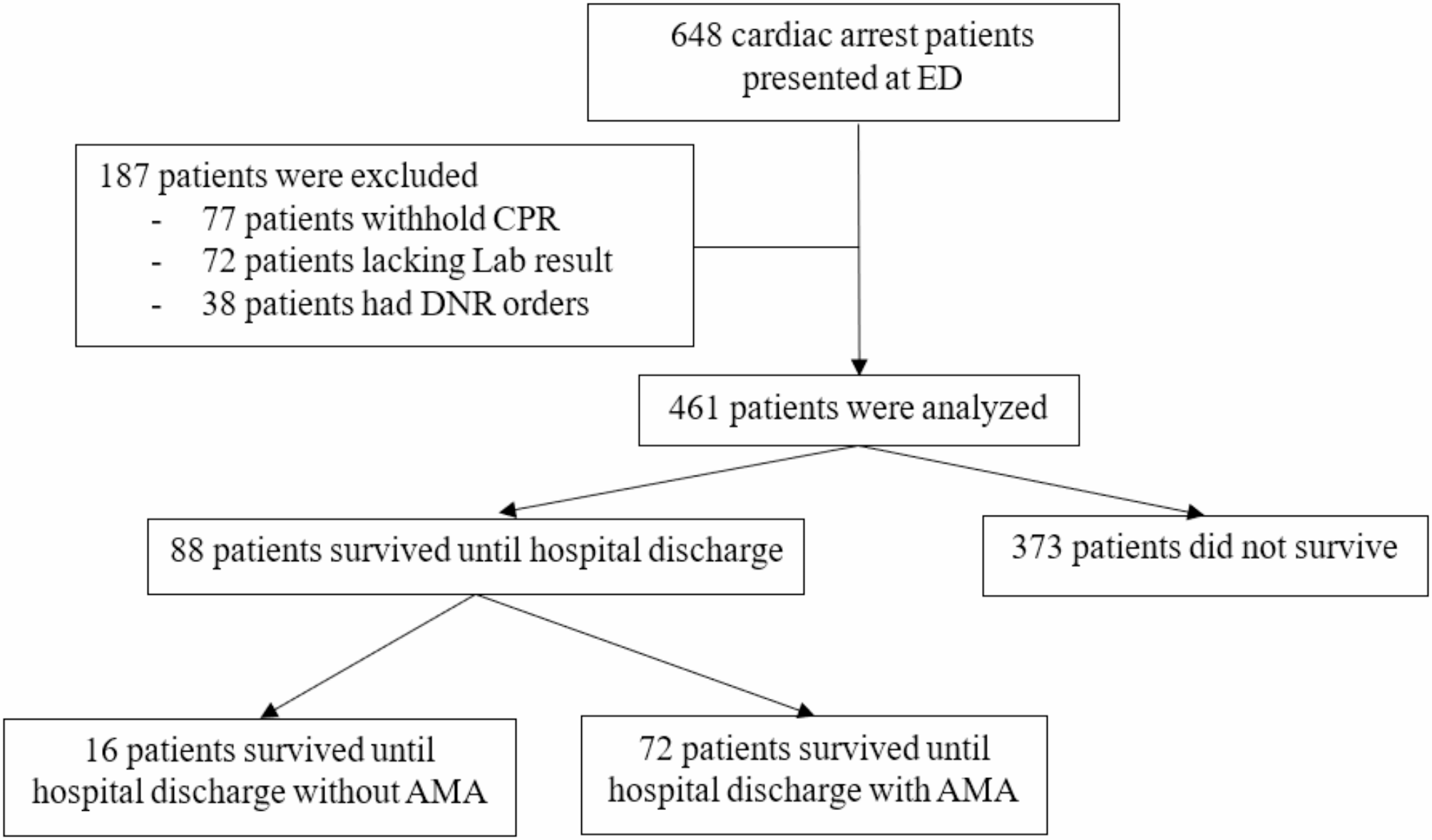
Interestingly, we observed a unique phenomenon where a significant proportion of survivors opted out of additional medical care and returned home against medical advice, where they subsequently succumbed to their condition. This finding likely reflects cultural beliefs prevalent in our region, particularly northeastern Thailand, where there is substantial value placed on dying within familiar surroundings and a belief that it is ethical to withdraw life support at home but not in the hospital [17]. Similar observations have been reported in studies from geographically diverse regions with distinct cultural contexts [18, 19]. This underscores the importance of considering cultural factors when interpreting patient decisions and suggests the potential need to tailor resuscitative strategies to align with individual preferences and values.
The sensitivity analysis conducted in our study, which reclassified patients who discharges AMA as non-survivors, offered critical insights into the robustness and reliability of our initial findings. Following this reclassification, the optimal bicarbonate cutoff increased from 12.6 mmol/L to 13.9 mmol/L, accompanied by a substantial improvement in sensitivity (from 74 to 93.8%) and a modest rise in specificity (from 47 to 52.1%). The AUC also improved from 0.607 to 0.72, reflecting moderate predictive capability.
This shift in the bicarbonate threshold highlights the significant impact of including discharged AMA patients in survival analyses, as their exclusion or reclassification can substantially influence study conclusions. The increased sensitivity observed in the refined analysis suggests that a bicarbonate level of 13.9 mmol/L may serve as a more reliable prognostic marker in clinical settings, especially for identifying patients with a higher likelihood of survival when discharged AMA cases are classified as non-survivors.
The improved AUC and high sensitivity associated with this new cutoff point underscore the importance of refining predictive models to address real-world complexities, including patients opting out of care. This is particularly pertinent in settings where cultural factors influence medical decision-making, as observed in our cohort. Moreover, the higher cutoff aligns more closely with thresholds reported in previous studies, bridging the gap between our findings and existing literature [12, 20]. Therefore, a cutoff point between 12.6 and 13.9 mmol/L may be used to guide the termination of resuscitation once the bicarbonate result is obtained.
Our study has several limitations. First, its retrospective design, single-center setting, and relatively small sample size limit its generalizability and make it challenging to account for confounding factors. Second, the lack of standardized criteria for terminating resuscitation and the inherent complexity of out-of-hospital cardiac arrest (OHCA) may have influenced patient outcomes. Third, the timing of cardiac arrest could affect bicarbonate levels; however, the exact time of onset was unknown for most cases, preventing its inclusion in our analysis. Future research incorporating multi-center collaborations and prospective study designs could help validate and expand upon our findings.
Our study contributes significantly to the understanding of the association between venous bicarbonate levels and critical outcomes in OHCA patients. The potential utility of readily available bicarbonate levels as a prognostic marker, particularly with the identified optimal cutoff of greater than 12.6 mmol/L, may improve outcome prediction in OHCA patients. Additional factors influencing survival outcomes include BUN, potassium, private transport, and initial cardiac rhythm. These findings offer valuable insights into resuscitation strategies, equipping clinicians with practical tools for assessing severity and estimating prognosis, especially in resource-limited settings.







Comments (0)