Acute colonic pseudo-obstruction (ACPO) also known as Ogilvie’s Syndrome (OS) is a rare but serious functional disorder characterized by dilatation of the colon, which usually involves the cecum and right colon without any mechanical obstruction. OS is often preceded by a surgical intervention [4].
Sir William Ogilvie first described Ogilvie’s Syndrome in 1948. Although the exact mechanism of the pseudo-obstruction remains unknown, the initial manuscript attributed its occurrence to the interruption of autonomic supply to the colon [1]. This is particularly relevant given the higher probability of OS in cases involving trauma, spinal anesthesia, and pharmacologic agents (such as Opioids) that affect the autonomic nervous system.
In an analysis of 400 cases, Ogilvie’s Syndrome was most commonly reported in patients in the sixth decade with a male predominance. The most common surgeries associated with it are cesarean sections and hip surgeries [5].
Another study conducted by Norwood et al., which reviewed all patients who underwent abdominal imaging after orthopedic surgery over a five-year period, indicated that Ogilvie’s Syndrome (OS) is relatively rare following major orthopedic procedures, occurring in nearly 1% of cases, with the majority involving hip surgeries. Notably, only one case out of 21 hip operations was insertion of a Dynamic Hip Screw (DHS). However, it significantly increases both morbidity and mortality rates [6].
The primary clinical presentation is abdominal distention, typically occurring three to seven days post-surgery, though it can develop within the first 48 h. Other symptoms include abdominal pain, nausea, vomiting, and constipation. Paradoxically, some cases may present with diarrhea. In rare instances, dyspnea has been reported due to colonic distention, which, in our case, necessitated ICU admission.
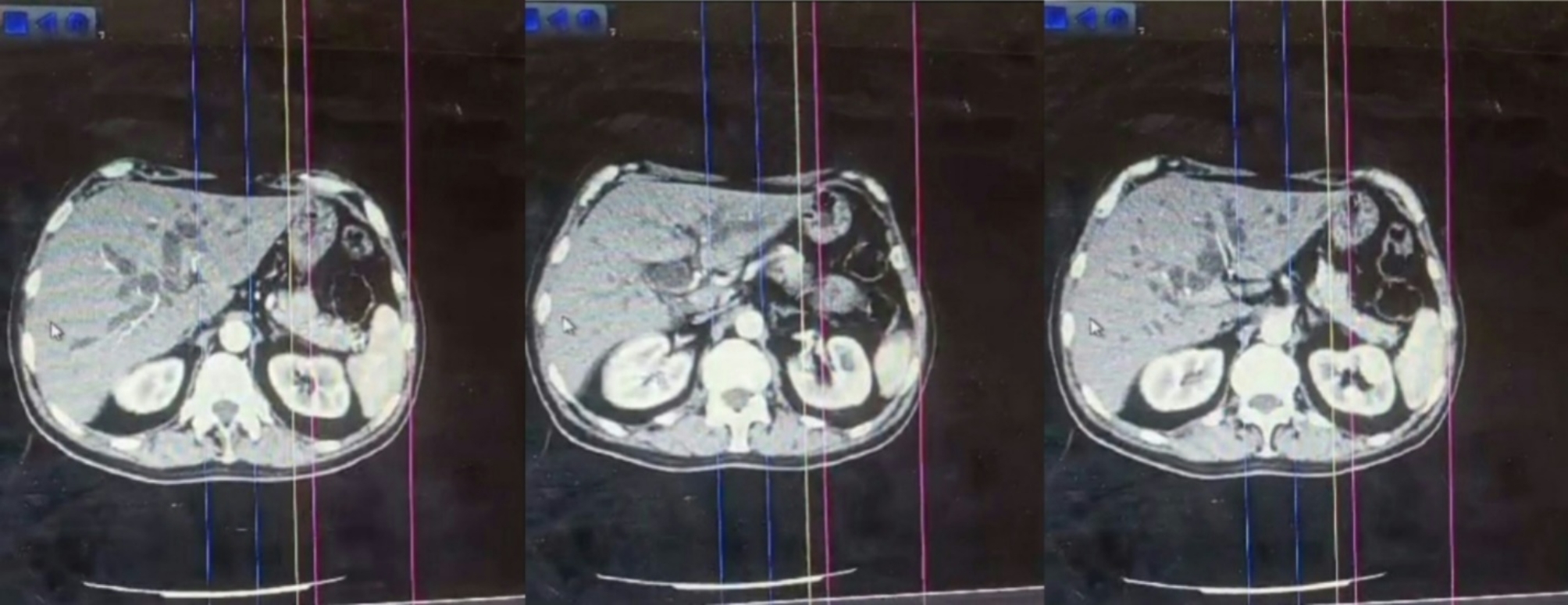
Diagnosis is confirmed by excluding other causes of intestinal obstruction, which requires abdominal imaging such as an Abdominal X-ray or a CT scan of the abdomen. A contrast enema using a water-soluble contrast is not preferred due to the high risk of perforation and subsequent peritonitis. The primary finding is dilatation of the proximal colon, which may occasionally extend to the rectum, without any evidence of mechanical obstruction [7].
Laboratory findings are typically normal or may show mild leukocytosis and metabolic abnormalities, such as electrolyte imbalances, particularly hypokalemia [8]. Differential diagnoses include mechanical obstruction, and toxic mega colon [9].
Choosing the optimal therapy depends on two main factors: the cecal diameter and the presence of complications. For patients without complications, conservative management is preferred. This primarily involves discontinuing pharmacologic agents especially opioids that reduce intestinal motility and decompressing the intestines using nasogastric tube and enemas to reduce the risk of perforation and peritonitis. Patients should be kept NPO (nothing by mouth) and given IV fluids to correct any electrolyte imbalances that may be present [10].
Alternatively, if the cecal diameter exceeds 12 cm or if conservative treatment fails, the preferred treatment is the administration of neostigmine, an acetylcholinesterase inhibitor. Neostigmine is given intravenously over a period of 5 min to minimize autonomic complications such as bradycardia and bronchoconstriction. Therefore, it is crucial to have atropine or glycopyrrolate on hand [11].
If the patient does not respond to the initial dose of neostigmine, a second dose can be administered after 24 h. A study demonstrated that the clinical response rate ranges from 40 to 100% [12].
Other methods to manage ACPO include colonoscopic decompression, which is reserved for patients who do not respond to neostigmine. This procedure is technically challenging and carries a high risk of complications, such as perforation.
Surgical treatment is reserved for patients with complications such as perforation, ischemia, and peritonitis, as well as those who are refractory to other management regimens [10].
In cases of acute intestinal pseudo-obstruction, the mortality rate is approximately 15% with prompt and appropriate management. However, when complications such as ischemia or perforation occur, the mortality rate can escalate to around 40% [5, 13].
The development and progression of acute pseudo-obstruction may be affected by several factors, including advanced age, electrolyte imbalances, and conditions such as diminished functional status, immobility, diabetes mellitus, non-operative trauma, severe infections, post-myocardial infarction states, and neurological disorders like Parkinson’s disease [14, 15].
This underscores the importance of early diagnosis of ACPO. Early detection allows for timely intervention, significantly improving patient outcomes. In its early stages, ACPO is manageable and can prevent severe complications.
However, if not promptly diagnosed and treated, ACPO can lead to serious complications with high morbidity and mortality rates. This highlights the need for healthcare professionals to maintain a high level of suspicion for this condition, especially in post-surgical patients presenting with symptoms like abdominal distention, pain, nausea, and vomiting.
Although Ogilvie’s Syndrome is rare and not commonly encountered in daily clinical practice, it is important to keep it in mind. Its complications, such as perforation, ischemia, and peritonitis, can be avoided if clinicians are familiar with the diagnostic methods and management algorithms.







Comments (0)