To our knowledge, this is the first case report that documents left arm numbness and subjective weakness as a presenting complaint for isolated posterior STEMI. Numbness in the arms, generalized weakness and left arm pain are known associated symptoms of myocardial infarction [7], while isolated left arm weakness is unique. In this case, initial differential diagnoses include acute sensory stroke or aortic dissection, which was promptly excluded with normal CT brain and 4-vessel angiography.
Atypical presentations of STEMI are variable, with chest pain or no chest pain. A systematic review of case reports showed that most atypical MI occur in patients at age > 50 years, with comorbidities such as diabetes, hypertension, and hyperlipidemia [8]. Our patient was unique as he had no known comorbidities and is not of the age range previously reported.
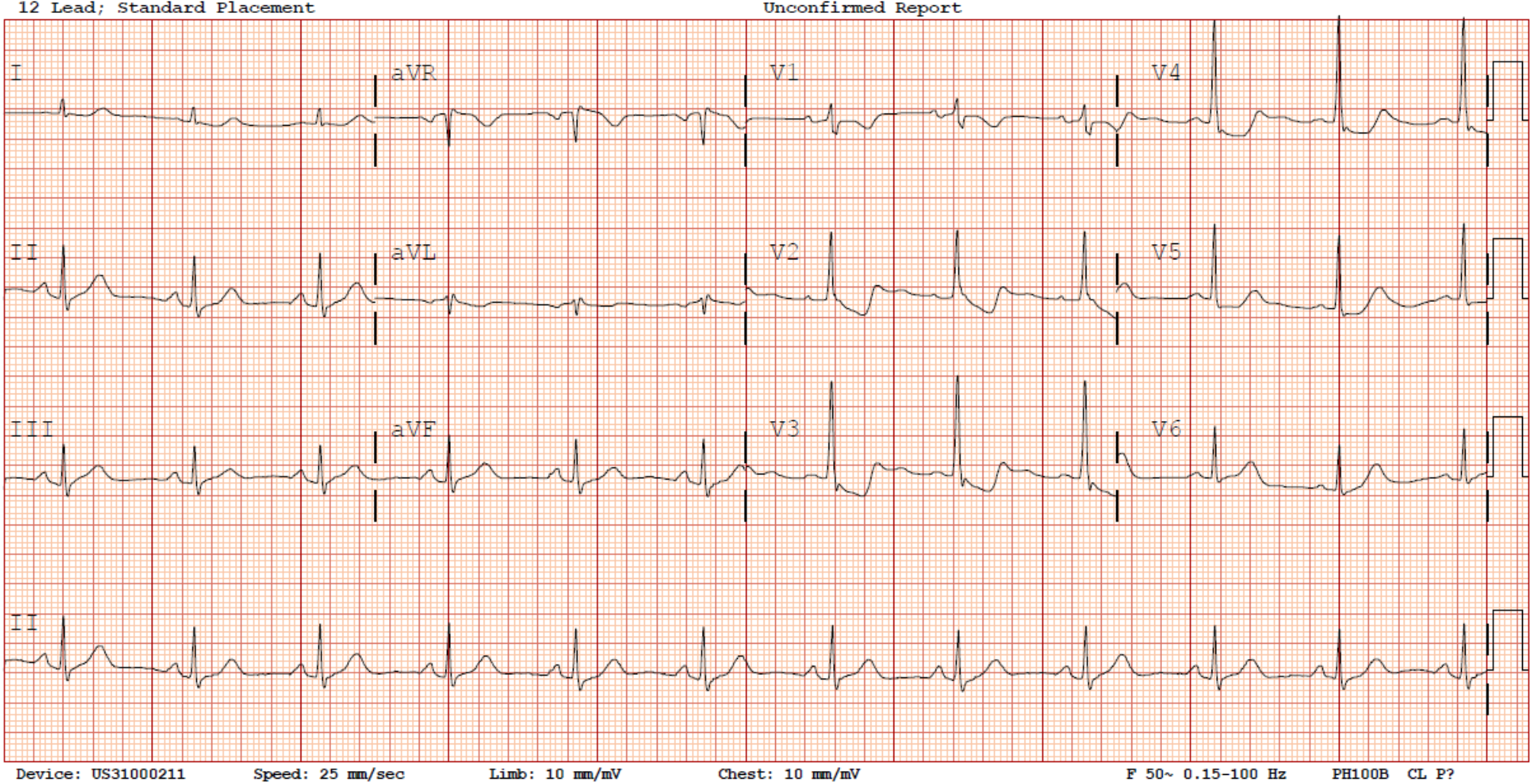
The additional challenge in this case was prompt recognition of the ECG changes of posterior STEMI. In this case, as the treating team was focused on investigating for cerebrovascular accident, the ECG recognition was delayed, with the posterior ECG taken 30 min after the initial ECG, despite machine reading of acute MI. During initial workup of the undifferentiated patient, care must be taken to maintain a broad differential diagnosis and to follow up on investigations ordered promptly. Additionally, further education and/or change in workflow may be required to ensure that the staff performing investigations alert emergency physicians of concerning machine reading such as this ECG tracing.
Majority of posterior STEMI happen together with inferior or lateral STEMI, which trigger clinicians to look for posterior changes. Isolated posterior STEMI remains underrecognized, as there are no obvious ST elevations in the standard 12-lead ECG. In posterior STEMI, attention must be paid to look for reciprocal changes in anteroseptal leads V1-3. Following initial suspicion, inclusion of lead V7, V8, and V9 increases diagnostic accuracy in posterior STEMI [9]. Of note, the threshold value for ST elevation in V7-9 is 0.5 mm [10].
In addition, other than posterior STEMI, ST depressions in anteroseptal leads V1-3 may also be caused by other non-ischemic causes such as left ventricular hypertrophy, left bundle branch block, or digoxin use [11]. Also, ECG abnormalities can often be found in stroke, such as T-wave abnormalities, prolonged QTc, Q waves, ST elevation and ST depression [12]. This adds to the challenge faced by the emergency physician in recognizing posterior STEMI promptly in this case.







Comments (0)