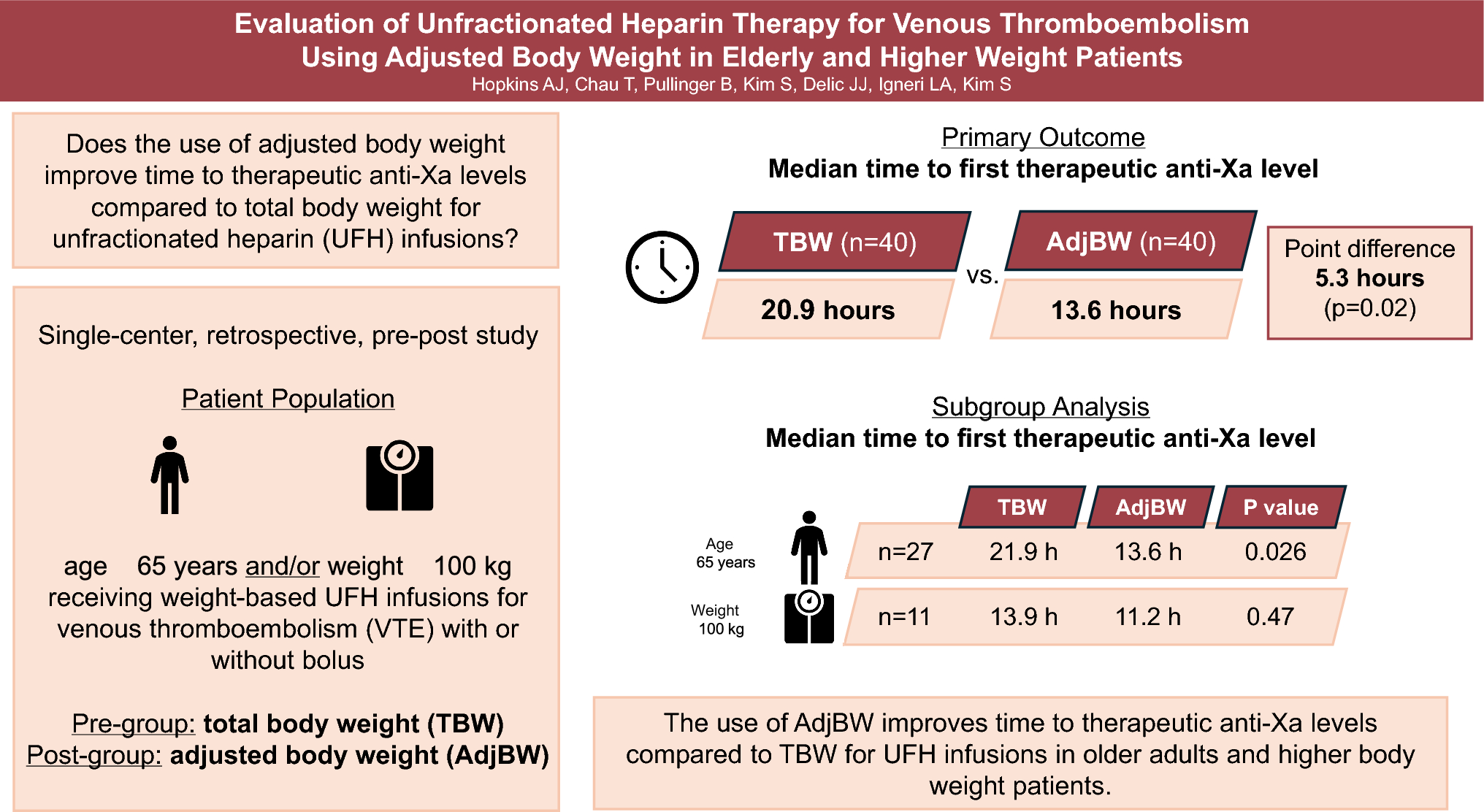
In this study, we compared the use of AdjBW versus TBW-based heparin dosing in older adults and higher weight patients. The median time to therapeutic anti-Xa level was significantly shorter in the AdjBW cohort compared with the TBW cohort. In subgroup analyses, this improvement in time to therapeutic anti-Xa was only observed in patients ≥ 65 years old. To our knowledge, this is the first study that directly compares the effects of AdjBW versus TBW dosing on anti-Xa outcomes in older adults [6,7,8,9]. The results of our study support the hypotheses generated by Schurr et al. and Barletta et al. who both found evidence supporting the need for an adjustment to heparin dosing that takes advanced age into account [10, 11]. Schurr et al. also demonstrated that utilizing AdjBW in higher weight and older adult patients significantly reduces the risk of the first collected anti-Xa value being supratherapeutic, which was supported by our results as well.
In terms of the weight subgroup, it is important to note that only eleven patients in each group exclusively met the weight criteria, and this analysis was likely underpowered to detect a statistically significant difference. The benefits of utilizing AdjBW for higher weight patients have been previously studied [5, 11, 13]. When George et al. divided patients into weight-based cohorts (< 100 kg, 100–124.9 kg, 125–150 kg, and > 150 kg), they found that higher body weight patients (≥ 100 kg) required a higher unit/hr dose, but a lower weight-based unit/kg/hr dose compared with lower body weight patients (< 100 kg) in order to achieve therapeutic aPTT levels. Based on this previously published data, the use of AdjBW in higher weight patients is reasonable even if they do not meet the age criteria.
Our study also found that the use of AdjBW improved the time to therapeutic anti-Xa levels specifically in patients who received an initial 80 unit/kg bolus dose. Given that bolus doses are administered to achieve rapid therapeutic anticoagulation in the presence of an active thrombus, our findings support the use of AdjBW for weight-based boluses. This may minimize the risk of bleeding while continuing to provide adequate anticoagulation in the setting of thromboembolism.
There were several instances of major bleeding events in this study (10% and 5% in the TBW and AdjBW cohorts, respectively). Of the four bleeding events noted in the TBW cohort, two received Naranjo scores of greater than 4, indicating that the adverse event was possibly due to the use of UFH (Online Resource 2). The two bleeding events noted in the AdjBW cohort received low Naranjo scores due to the lack of temporal association and presence of alternative causes.
This study is limited by its retrospective, single-center nature. Many hospitals utilize an institution-specific protocol for monitoring and titrating UFH infusions, which limits the generalizability of this study. There were two factors noted that may have contributed to lengthened times to therapeutic anti-Xa levels as well. First, anti-Xa levels drawn greater than six hours after infusion initiation or a rate change were included in the analysis. There were two patients in each cohort whose first anti-Xa levels were collected over 10 h following UFH initiation. Second, several blood samples were reported as hemolyzed, requiring the samples to be redrawn. While this issue impacted similar amounts of patients in the TBW (12 of 249 samples) and AdjBW cohorts (10 of 259 samples), the hemolyzed samples may have delayed time to therapeutic anti-Xa by several hours for patients that had not yet achieved a therapeutic anti-Xa, five patients in the TBW group and three patients in the AdjBW group. Additionally, the primary outcome of this study focused on laboratory values rather than patient-centered endpoints such as successful VTE treatment or decrease in bleeding rates. Lastly, the time frames studied were chosen to avoid the early COVID-19 era, when virus-induced coagulopathy was a poorly understood concern. This limits the generalizability of our study to patients with COVID-19-induced coagulopathy who may have different heparin requirements. The promising findings from this study warrant a larger, prospective randomized controlled trial to strengthen the hypothesis that utilizing AdjBW-based dosing is efficacious in treating VTE and will minimize the risk of bleeding compared to TBW-based dosing.
To obtain the most accurate anti-Xa assessments, 44 patients were excluded for use of oral factor-Xa inhibitors, such as apixaban or rivaroxaban, during or directly prior to the index admission. Given the increasing use of these medications for prior VTE and stroke prophylaxis in patients with atrial fibrillation, additional studies should be conducted in these populations to assess clinical outcomes.
Some strengths of this study include its real-life applicability given the inclusion of inconclusive anti-Xa assays and allowance for minor delays in anti-Xa testing. Additionally, the use of anti-Xa in this study allowed monitoring of UFH infusions that was not impacted by the variables that impact aPTT monitoring, such as liver dysfunction, hypercoagulable states, and abnormal Factor II and VIII concentrations. The time periods selected for this study also carefully avoided the early COVID-19 era, during which COVID-19-induced coagulopathy was of greater concern and not as well understood. Finally, by stratifying patients during the inclusion process, it was ensured that the sample evaluated was balanced in terms of weight and age.
In conclusion, the results of our study find that the use of AdjBW-based dosing of UFH improves time to therapeutic anti-Xa levels in older adults and higher body weight. This finding was seen primarily in older adults and the subgroup analyses did not find a statistically significant difference in time to therapeutic anti-Xa levels in higher body weight patients who did not meet the older age criteria.

Comments (0)