
Remember me
One hundred and fifty-one (151) nodes in 65 node-positive LACC patients were included. The median age of patients was 48 years (range 32–77 years). Majority of the patients had squamous histology (n = 57, 87.7%); 7 had adenocarcinoma (10.7%) and 1 patient had adeno-squamous carcinoma (1.5%). Forty-three (66%) patients had IIIC1 and 22 (34%) patients had IIIC2 disease. Patient characteristics and treatment details are depicted in Table 1.
Table 1 Patient and disease characteristicsStage IIIC1 patients were treated with pelvic fields. Twenty two patients (34%) with para-aortic lymphadenopathy were treated with extended field RT. Sixty one (94%) patients received concurrent chemo radiation, while 4 (8%) patients received radiation alone. The reasons for chemotherapy omission included low glomerular filtration and cardiac comorbidities(1), infection (3). The median number of chemotherapy cycles were 5 (Range 1–6). A median of 2 nodes were involved (range 1–6) (IQR 1–3). Median volume of the largest node was 3.4 cc (IQR 1.8–6.8 cc). As per the RECIST 1.1 definition, 58 (38.4%) nodes were non-pathologic (< 10 mm), 59 (39%) nodes were non-target lymph nodes (measuring ≥ 10 mm to < 15 mm) and 34 (22.6%) nodes were target lymph nodes (≥ 15 mm).
Mean treated PTV volume for SIB was 25.3 cc (median 21.9 cc, IQR 11.5 – 33.5 cc) Number of nodes receiving dose of 50 Gy were 7 (4.6%), > 50 to < 55 Gy were 36 (23.8%) and ≥ 55 Gy were 108 (71.5%).
Follow-Up and ResponseThe median time to first follow-up was 4 months (IQR-12–24 weeks) and the median overall follow-up time of the cohort was 43 months (6–64 months).
Patient OutcomesTreatment ResponseAt the first follow up with imaging (median of 4 months), of the 151 nodes that were evaluated, 92.1% nodes (n = 139/151) had complete response, 7.3% (n = 11/151) had partial response and 0.6% (n = 1/151) had progressive disease.
Disease Free SurvivalAt a median follow up of 43 months (range 6–64 months), 21(32%) patients had recurred. The 5-year local control and 5-year disease free survival for the overall cohort was 88.7 and 66% respectively. For patients with stage IIIC1 and IIIC2 patients, the 5-year DFS was 76.7% and 43.5% respectively (p = 0.034) (Fig. 1A). For patients with largest gross nodal volume of > 3 cc, (n = 37) the 5-year DFS was 55%, compared to 80.8% for patients with largest gross nodal volume of ≤ 3 cc node (n = 28) (p = 0.034) (Fig. 1B). The 5-year DFS for patients receiving SIB < 55 Gy was 62% and ≥ 55 Gy was 67.2% (p = 0.618) (Fig. 1C). For patients who received concurrent chemotherapy, the 5-year DFS was 66.5% compared to 60% for patients who did not (p = 0.377) (Fig. 1D). On multivariate analysis, none of the factors were significant for DFS (Supplementary Table 1).
Fig. 1
Kaplan Meier Survival Graphs depicting 5-year Disease Free Survival. A Stratified on stage IIIC1 vs. IIIC2. B Volume of largest node ≤ 3 cc vs > 3 cc. C Dose received by largest node < 55 Gy vs ≥ 55 Gy. D Chemotherapy received or not
Nodal ControlThe 5-year nodal control for the 65 patients was 85.6%, the 5-year paraaortic and 5-year pelvic nodal control were 88.8 and 94.6% respectively. For patients with stage IIIC1 and IIIC2 disease, the 5-year nodal control was 89.7 and 74.3% respectively (p = 0.466) (Fig. 2A). For patients with largest gross nodes of > 3 cc volume, (n = 37) the 5-year nodal control was 82.5% compared to patients with largest gross node ≤ 3 cc with a 5-year nodal control of 88.9% (p = 0.810) (Fig. 2B). The 5-year nodal control for patients with largest gross nodes receiving < 55 Gy was 89.1% and ≥ 55 Gy was 82.1% (p = 0.718). For patients receiving concurrent chemotherapy along with radiation, the 5-year nodal control was 86.4% and for those receiving radiation alone, the 5-year nodal control was 75% (p = 0.377) (Fig. 2C).
Fig. 2
Kaplan Meier Survival Graphs depicting 5-year Nodal Control. A Stratified on stage IIIC1 vs. IIIC2. B Volume of largest node ≤ 3 cc vs. > 3 cc. C Chemotherapy received or not. D Figure 2D shows 5 year in-field nodal control for patients that received simultaneous integrated boost
In-Field Nodal FailureOf the 151 nodes that were evaluated and received SIB, there was in-field nodal failure in only 1/151 nodes that received SIB, with the 5-year pathological nodal control rate within the nodal boost volume was 99.3% (Fig. 2D).
Patterns of RecurrencePatterns of recurrence are described in Supplementary Fig. 1. Of the 21 patients who had recurred, 11 (17%) patients had distant metastasis (2 with locally recurrent disease and 1 with pelvic nodal), 5 recurred in para-aortic region (7.7%), and 5 recurred in the pelvis (7.7%) (1 in nodal region and 4 were locally recurrent). Of these 11 patients with distant metastasis, the most common site of relapse was lung (n = 7), 2 patients had supraclavicular nodal recurrence, 1 had bone metastasis, 1 had peritoneal metastasis. Eight of the patients with distant metastasis were Stage IIIC2, and 3 patients were stage IIIC1.
There were a total of 7 patients with nodal failure, 4 in the para-aortic region, 2 in the pelvic nodes, and 1 patient failed in para-aortic and pelvic (presacral) nodal region. This is depicted in Table 2 with representative nodal failure images in Fig. 3. Of the patients who recurred in the paraaortic region, 3 patients were initially Stage IIIC1 (not previously radiated regions), and 2 patients were stage IIIC2 (previously irradiated region). There was only 1 patient with nodal failure that occurred in the SIB volume, 3 patients had nodal failure in the 45 Gy treated volume (which did not receive any SIB dose due to no nodes at the time of initial treatment), and 3 patients had failures which had not received any radiotherapy. Seven patients had local failure or persistent disease, of which 2 also developed distant metastases and 1 patient had pelvic nodal failure as well.
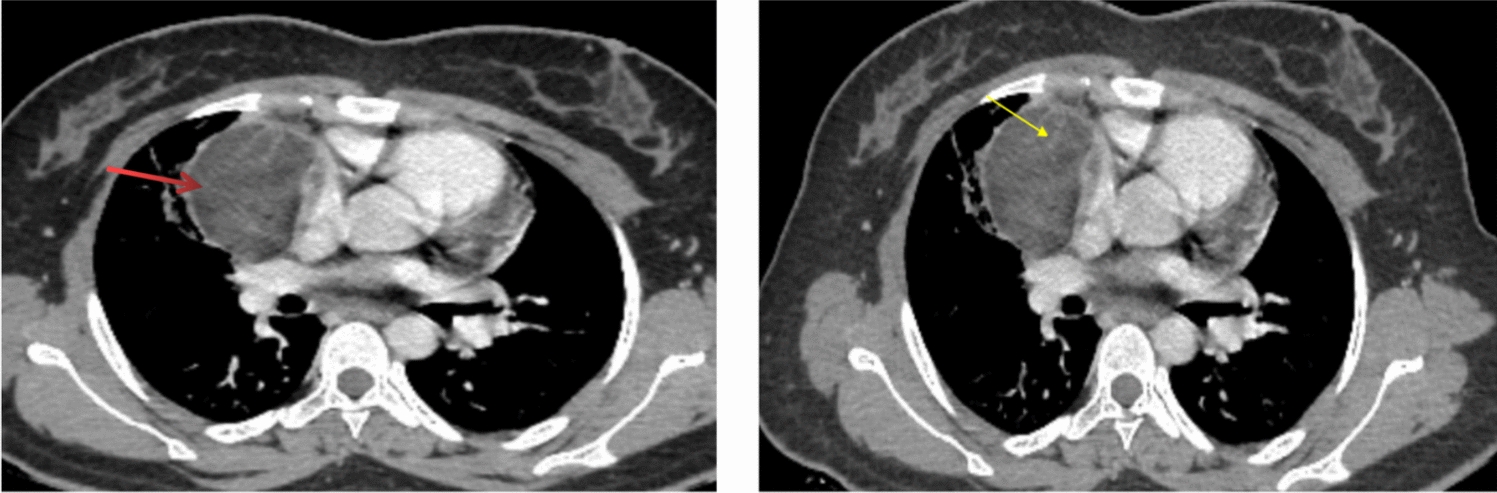
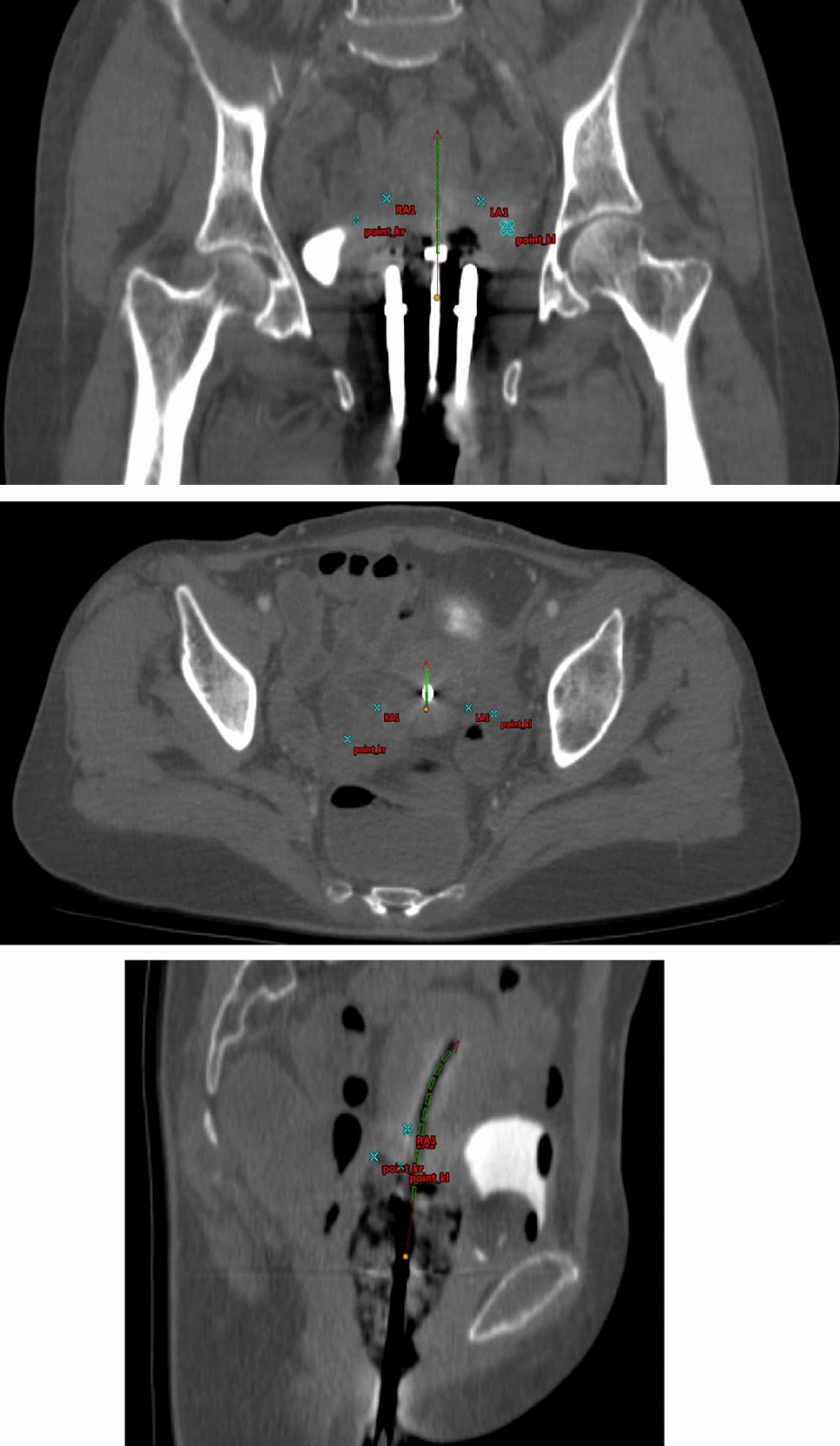
Table 2 Table depicting patterns of nodal failure (PALN: Para-Aortic Lymph Node, fr: Fraction)Fig. 3
Patterns of nodal failure. Patient A & B nodal failure in 45 Gy treated volume (Potentially reduced contribution from Brachytherapy). Patient C nodal failure in 54 Gy boosted volume
ToxicityFourteen patients (21%) reported to having grade ≥ 2 gastrointestinal toxicities and 2 patients (3%) had grade ≥ 2 genitourinary toxicity.
Majority of the patients (n = 34, 52.3%) did not report any chronic gastrointestinal toxicities, while grade 1, 2 and 3 toxicities were reported by 17(26%), 3 (4.6%) and 11 (17%) patients respectively. Grade 1 toxicities included abdominal pain (9), diarrhea (1), Fecal urgency (1), occasional per rectal bleed (6). Grade 2 toxicities included abdominal pain (1) and per rectal bleed (3). All of the grade 3 GI toxicities were radiation proctitis and bleeding for which patients underwent sigmoidoscopy SOS argon-plasma coagulation or hyper-baric oxygen therapy. Forty-eight patients (73.8%) experienced no acute genitourinary toxicity while 12 patients (18.5%) had grade 1 toxicity, 2 (3%) patients had grade 2 genitourinary toxicity, and none had grade 3 toxicity. Grade 1 toxicity included occasional burning micturition (6), occasional hematuria (4) and urinary urgency (2). Grade 2 GU toxicities included hematuria (2).
Comments (0)