Patients and study design
A prospective, single-center, single-masked, randomized controlled clinical trial compared the bilateral implantation of two monofocal IOLs and one enhanced monofocal IOL. Patients scheduled for consecutive bilateral cataract extraction at the Trieste University Eye Clinic’s Cataract Surgery service were enrolled between November 2019 and May 2022. The enrolled patients were divided into three groups of 30 patients each, each of whom was a candidate for bilateral implantation of one of the three lenses under investigation: Tecnis Eyhance™ -ICB00 (Johnson & Johnson Vision), Tecnis® 1-piece monofocal (PCB00) (Johnson & Johnson Vision) or Clareon® monofocal (CNA0T0) (Alcon Laboratories). The second eye was implanted 1 month after the first.
Exclusion criteria included anterior segment pathology that could have a significant impact on outcomes (e.g., chronic uveitis, iritis, corneal dystrophy, keratoconus), axial length ≤ 21 mm or ≥ 26 mm, corneal topographic astigmatism higher than 0.75 D, diabetic retinopathy, uncontrolled glaucoma and or IOP > 24 mmHg, all kind of infections (acute ocular disease, external/internal infection, systemic infection), traumatic cataract, pseudoexfoliation syndrome, pupillary abnormalities including aniridia and/or pupillary diameter in mesopic conditions in distance vision ≤ 2.5 mm and ≥ 6 mm, microphthalmia, amblyopia, degenerative visual disorders (e.g., macular degeneration, optic nerve atrophy or retinal disorders), previous intraocular and corneal surgery, systemic or ocular pharmacotherapy which could impact the visual acuity and/or cause floppy iris syndrome and/or insufficient dilation according to the investigator's opinion, strabismus, nystagmus, pregnancy or lactation period for female patients.
Following the Helsinki Declaration, each patient provided written informed consent before participating in the study. The Hospital Ethics Committee approved the study (RCTICB00; protocol 202/2019). The trial was retrospectively registered (ClinicalTrials.gov Identifier: NCT06118944). Patients were consecutively randomized by block randomization and assigned in a 1:1:1 allocation ratio to three study arms using Sealed Envelope Ltd. 2017 [Available from: https://www.sealedenvelope.com/simple-randomiser/v1/lists]. An automatically generated unique randomization code was assigned to the randomized patient, followed by the abbreviation LE or RE to distinguish between left and right eyes, respectively.
Assessments
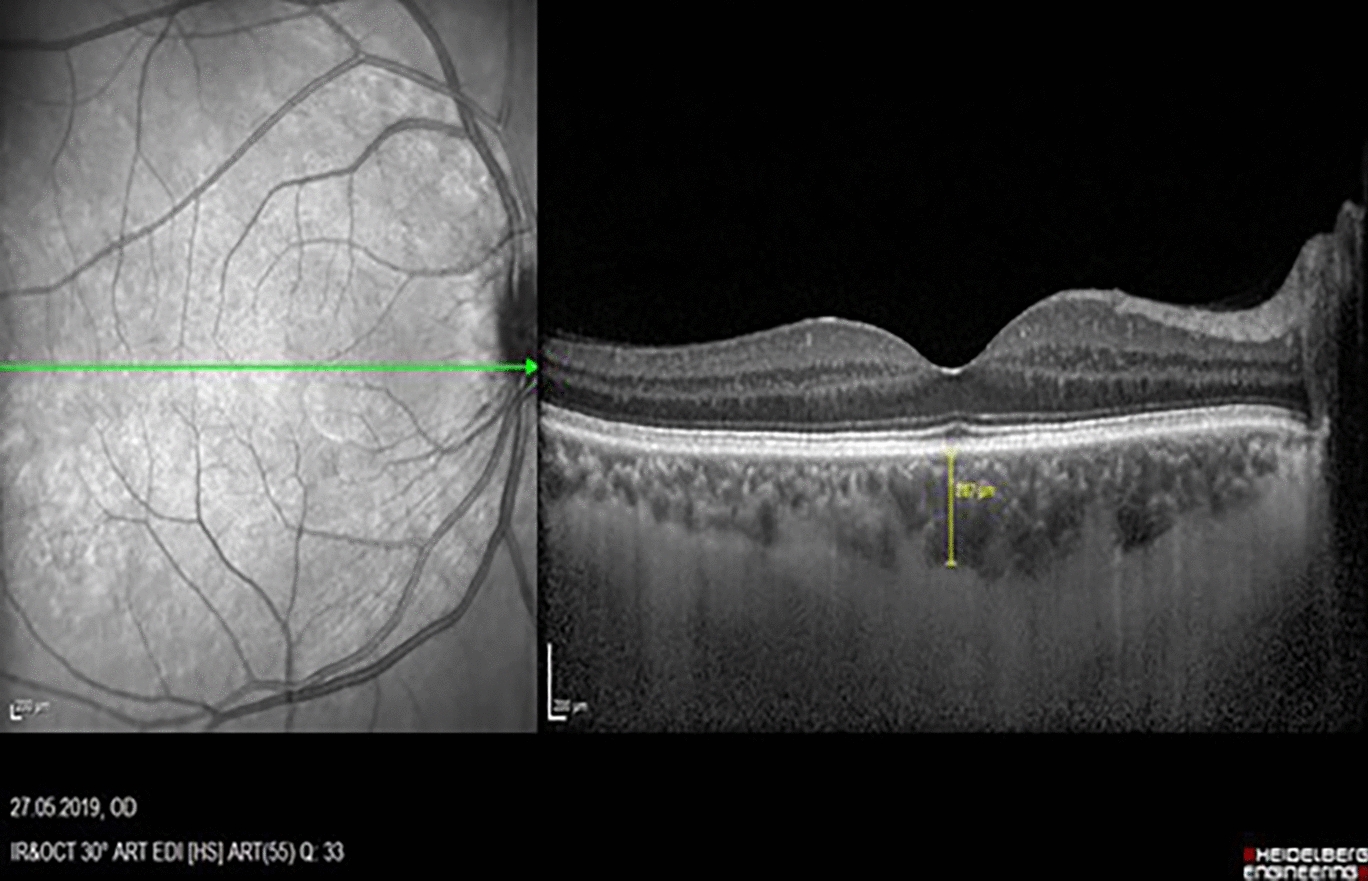
All patients underwent a comprehensive preoperative ophthalmological examination before surgery, which comprised a complete medical history recording, including demographic data and systemic diseases, the measurement of monocular and binocular uncorrected distance visual acuity (UDVA) (at 4 m) and corrected distance visual acuity (CDVA), anterior segment slit lamp examination, Goldmann applanation tonometry, fundus oculi examination after dilatation with Tropicamide 1% eye drops, macular optical coherence tomography (Spectralis HRA + OCT; Heidelberg Engineering, Heidelberg, Germany), bilateral optical biometry (IOLMaster® 700; Carl Zeiss Meditec AG, Jena, Germany, OPD), corneal topography and pupillometry (Scheimpflug camera—Sirius; C.S.O.) and quality of life assessment using Catquest-9SF questionnaire. Data acquired with IOLMaster® 700 were used to calculate the IOLs' dioptric power. The IOL powers were calculated using the Barrett Universal II formula. The dioptric power with the expected refractive target closest to emmetropia was chosen.
Postoperatively, patients were evaluated 12 weeks (3 months) after the second eye surgery. Each patient underwent biomicroscopy of the anterior segment to assess the overall state of the operated eye and, subsequently, monocular and binocular visual outcomes with uncorrected and corrected visual acuity for far distance (UDVA, CDVA), uncorrected visual acuity for intermediate distance (UIVA), distance-corrected intermediate visual acuity (DCIVA), distance-corrected near visual acuity (DCNVA), corrected near visual acuity (CNVA). Near vision correction (NVC) spherical equivalent (SE) was recorded as well. Corrected visual acuity was obtained using the “Maximum plus” (or minimum minus) technique, a subjective refraction technique that produces the best vision with the minimum minus or maximum plus correction.
Early Treatment Diabetic Retinopathy Study (ETDRS) acuity charts were used to measure pre- and postoperative visual acuities. Distance Visual Acuity (DVA) was obtained with a 4 m ETDRS board illumination cabinet at high contrast (96%) with an 85 cd/m2 lamp filter tube (Precision Vision), intermediate visual acuity (IVA) was obtained with a 70 cm ETDRS printed chart (Precision Vision), and near visual acuity (NVA) was obtained with a 40 cm ETDRS printed chart (Precision Vision). Binocular corrected distance defocus curves were obtained. To produce defocus, a progression of IOLs in − 0.50 D increments was consecutively added (range + 2.00 to − 4.00 D), after which visual acuity was tested with 100% contrast ETDRS distance acuity charts at a test distance of 4 m. The self-administered validated Catquest-9SF questionnaire assessed patients' satisfaction with visual outcomes for daily life activities at 12 weeks.
Intraocular lenses
ICB00 is a 1-piece acrylic aspheric refractive foldable posterior chamber IOL designed for placement in the capsular bag. This IOL is made of the same hydrophobic Sensar acrylic material and has the same overall geometry/dimensions (13 mm overall length and 6.0 mm optic diameter) as the standard 1-piece monofocal IOL. It has the same features as the PCB00 IOL, except for the modified aspheric anterior surface of the optic. The enhanced and standard monofocal IOLs are based on refractive technology without diffractive rings or zones and have the same IOL constant. The enhanced monofocal IOL has a refractive optical design with a higher-order aspheric anterior surface that creates a continuous power profile (the power increases continuously from the periphery to the center of the lens), which is intended to extend the depth of focus, thus improving vision for intermediate tasks compared with a standard monofocal IOL [7,8,9,10].
Moreover, ICB00 IOL compensates for corneal spherical aberration similarly to the standard 1-piece monofocal PCB00 IOL, adding a negative spherical aberration of 0.27 μm. The standard IOL PCB00 is a 1-piece UV-light filtering acrylic monofocal IOL with a modified prolate (aspheric) design on the anterior optic surface to reduce the overall spherical aberration to near zero once it is implanted. The CNA0T0 monofocal IOL is a one-piece aspheric, hydrophobic, monofocal non-toric IOL made of ultra-violet and blue-light filtering acrylate/methacrylate copolymer. It has the same mechanical design as the AcrySof® model SN60WF with a reported 0.20 μm negative spherical aberration [11]. CNA0T0 IOL features include Stableforce® modified-L haptics (Alcon Vision), a full 6.0-mm optic diameter, a proprietary square-edged design, and a 13.0-mm overall length.
Surgery
Patients considered eligible during the preoperative visit were scheduled for surgery and were operated on by an expert surgeon (DT). Standard phacoemulsification through a 2.4 mm clear corneal incision followed by IOL insertion in the capsular bag is the routine approach for cataract extraction using topical anesthesia at our department (unless complicated cases). Anterior capsulotomies were performed as a continuous, curvilinear capsulorhexis of 5.0 to 5.5 mm diameter performed by manual capsulorhexis.
Outcome measures
The study's primary goal was to evaluate and compare the clinical outcomes of three parallel groups of patients following bilateral implantation of the ICB00 IOL, PCB00 IOL, or CNA0T0 IOL. Considering the modified optical profile of the ICB00, the primary outcome was the evaluation of intermediate-distance visual performance. The primary endpoint was to compare groups in terms of binocular DCIVA at 12 weeks after the second eye implant. Secondary endpoints included monocular and binocular UIVA, UDVA, CDVA, DCNVA, CNVA, monocular NVC SE, binocular defocus curves and Catquest-9SF questionnaire scores.
Statistical analysis
One-way ANOVA with partial eta squared (ηp2) as an effect size indicator was applied to compare the groups regarding clinical and demographical variables. The between-group differences in postoperative data were evaluated with ANCOVA, including age-controlled covariate. In this case, all between-group comparisons performed with controlled covariates were carried out individually for each dependent variable. The Catquest-9SF data were fit to the Rasch model using WINSTEPS version 4.2 using the Andrich version of Rasch model estimates based on joint maximum likelihood estimation. A Rasch analysis compares the difficulty required to complete a task mentioned in the items to the participant’s ability level to perform that activity. Both the object’s difficulty and the individual’s ability are sorted on the same linear scale. If the data fit the Rasch model’s assumptions, the ordinal raw score is transformed into a valid Rasch scale. This scale is linear and has a logit unit, which is the natural logarithm of the odds ratio. Because the Catquest-9SF should be valid for measuring both before and postoperative patient data, Rasch analysis was done with preoperative and postoperative data stacked as a single dataset. The Bonferroni correction was applied to establish a statistical significance threshold resulting from multiple tests of other controlled covariates. After determining the distributional parameters significantly differentiating the groups, correlations between these parameters were calculated separately.



Comments (0)