Patient characteristics
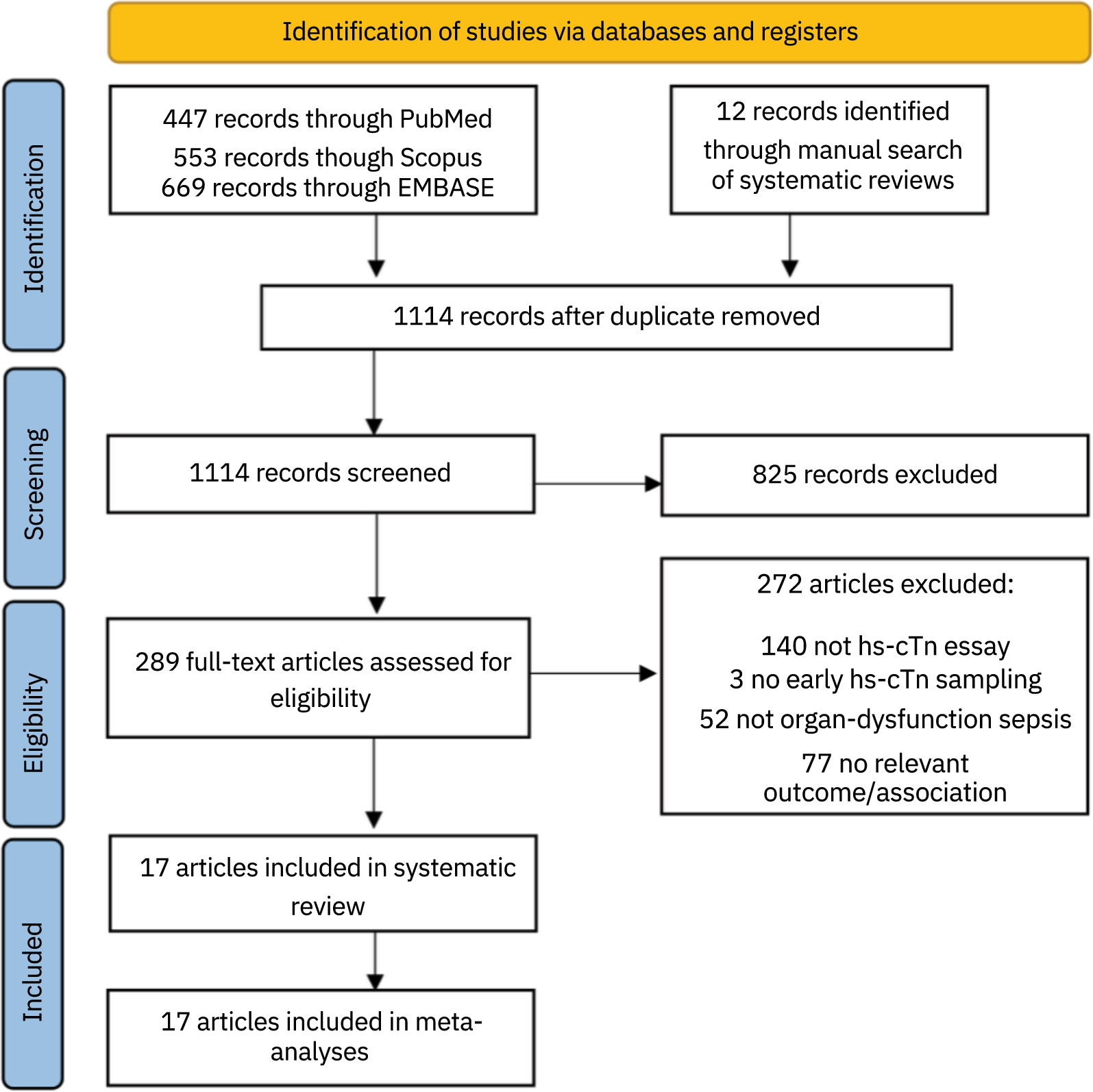
The original study cohort included 384 children admitted to PICU with septic shock. After exclusion of patients with end stage kidney disease or pre-existing kidney disease without a known baseline SCr (n = 14) and those missing SCr data from Day 1 or Day 3 (n = 7), 363 patients were included in the current analysis (Additional file 2: Figure S1), all of whom had complete data on Day 1, Day 3, and Day 28. One hundred forty patients (39%) were sRAI + on Day 1 of septic shock. Table 1 outlines clinical, demographic and outcome data for the cohort by presence or absence of sepsis renal angina fulfillment. sRAI + patients more commonly had: (1) a history of transplant (solid organ or hematopoietic stem cell), (2) higher severity of illness by both PRISM III and PERSEVERE-II, and (3) higher incidence of requiring vasoactive support and invasive mechanical ventilation on Day 1, as well as higher intensity of vasoactive support by VIS. The sRAI + cohort had increased risk for D3 severe AKI (RR 8.9, 95%CI 5.0–16.0, p < 0.001), KRT use in the first week of septic shock (RR 18, 95%CI 6.6–49, p < 0.001), and 28-day mortality (RR 2.5, 95%CI 1.2–5.5, p = 0.013), as well as fewer PICU free days (14.5 days [0–23] vs. 25 days [19,20,21,22,23,24,25,26], p < 0.001). (Additional file 3: Tables S1 and S2) outline the incidence of D3 severe AKI and KRT use by each possible RAI score, sRAI designation (sRAI + /sRAI-) and by individual score components.
Table 1 Demographic, clinical and outcome characteristics of the cohort by presence or absence of sepsis renal angina (sRAI) fulfillment on Day 1Seventy-nine patients (22%) developed D3 severe AKI. Demographic, clinical and outcome variables for patients with and without D3 severe AKI are shown in Table 2. On Day 1 of septic shock, patients who developed D3 severe AKI had: (1) higher severity of illness by PRISM III and PERSEVERE-II, (2) higher rates of vasoactive medication use and invasive mechanical ventilation, (3) higher intensity of vasoactive support by VIS and 4) higher %FB, greater degree of elevation of SCr > Baseline, and lower median platelet count (Table 2). Patients with D3 severe AKI also had fewer PICU free days (4 days [0–20] vs. 24 days [16,17,18,19,20,21,22,23,24,25,26], p < 0.001) and great risk for mortality (RR 4.9, 95%CI 2.4–10.2, p < 0.001).
Table 2 Demographic, clinical and outcome characteristics based on the presence or absence of severe acute kidney injury on day 3Assessment of sRAI for prediction of D3 severe AKI and comparison to context-free serum creatinine elevation and original RAI
Table 3 outlines clinical, demographic and outcome variables for sRAI + patients compared to those who were D1 SCr > Baseline + and RAI + , as well as the predictive performance of each for D3 severe AKI. The sRAI performed well to predict D3 severe AKI, with AUROC 0.86 (95%CI 0.82–0.90), sensitivity 85% (95%CI 75–92), specificity 74% (95%CI 69–79), PPV 48% (95%CI 39–56), and NPV 95% (95%CI 91–97).
Table 3 Clinical, demographic and outcome variables and predictive performance of day 1 sepsis renal angina fulfillment (sRAI +) compared to degree of serum creatinine elevation above baseline (D1 SCr > Baseline) and original renal angina fulfillment (RAI +)While the predictive performance of the sRAI compared to D1 SCr > Baseline by AUROC (0.86 [0.82–0.90] vs. 0.82 [0.76–0.88], p = 0.19) did not differ, sRAI had higher specificity (74% vs. 36%), PPV (48% vs. 28%) and + LR (3.3 vs. 1.4) (Table 3). Compared to D1 SCr > Baseline + patients, sRAI + patients had higher risk of D3 severe AKI (RR 1.7, 95%CI 1.3–2.2, p < 0.001), higher risk of requiring KRT in the first week of septic shock (RR 1.9, 95%CI 1.3–2.8, p < 0.001), and fewer PICU free days (14.5 days [0–23] vs. 23 days [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26], p < 0.001).
One hundred ninety-five patients (54%) met the original criteria for renal angina fulfillment (RAI +), compared to 140 (39%) who met sRAI + criteria. D3 severe AKI occurred in 76 of 195 RAI + patients (39%) compared to 67 of 140 sRAI + patients (48%) (p = 0.11). While sRAI + was less sensitive for D3 severe AKI prediction (85% vs. 96%), sRAI + was more specific (74% vs. 58%), with higher PPV (48% vs. 39%) and relatively preserved NPV (95% vs 98%). There were no differences in PICU free days, risk of KRT or mortality, between sRAI + and RAI + patients (Table 3). Additional file 2: Figure S2 further illustrates the incidence of D3 severe AKI using each predictive tool and highlights the additive benefit of the sRAI modification above the original RAI with regard to PPV.
Examining association of sRAI + with outcomes
On multivariable logistic regression, sRAI + retained associations with D3 severe AKI (adjusted OR 4.54, 95%CI 2.03–10.2, p < 0.001) and need for KRT in the first week of septic shock (adjusted OR 5.6, 95%CI 1.48–21.5, p = 0.01), after adjustment for other significant covariates identified on bivariate analysis (PRISM III, D1 VIS, PERSEVERE-II, baseline SCr) (Table 4). While D1 SCr > Baseline + also retained significant associations with D3 severe AKI, similar findings were not seen with need for KRT in the first week (Table 4).
Table 4 Multivariable logistic regression examining the association between sepsis renal angina fulfillment (sRAI +), serum creatinine above baseline on day 1 (D1 SCr > Baseline +), severity of illness and baseline creatinine used on the presence of severe acute kidney injury on day 3 and need for kidney replacement therapy 
Comments (0)