
Remember me


Very early-onset inflammatory bowel disease (VEO-IBD) is a subtype of inflammatory bowel disease (IBD) defined by onset in children younger than 6 years and is reported to have a specific clinical presentation when compared with children diagnosed at an older age.1 The use of monoclonal antibodies to anti-tumor necrosis factor-alpha (aTNFα) can be effective in maintaining remission in VEO-IBD.2 However, discontinuation of aTNFα medications for loss of efficacy is common, with loss of response occurring in greater than 50% of patients. It is suspected that this number could be decreased with therapeutic drug monitoring.2 Infliximab dose intensification, to achieve and maintain a response and durable remission, is recognized to benefit children with IBD younger than 2 years.3 This same strategy is recommended for all children diagnosed with IBD younger than 10 years, with pretreatment predictors of subtherapeutic infliximab drug levels developed for children of this age group diagnosed with Crohn's disease (CD).4,5 However, compared with adalimumab, dose intensification of infliximab is more likely to be required to maintain a durable response in children with CD.6 We present the case of a child younger than 2 years diagnosed with CD who had a good clinical response and maintained durability of the response, but required dramatic dosing changes to maintain adalimumab trough drug levels during the first 2 months after its initiation.
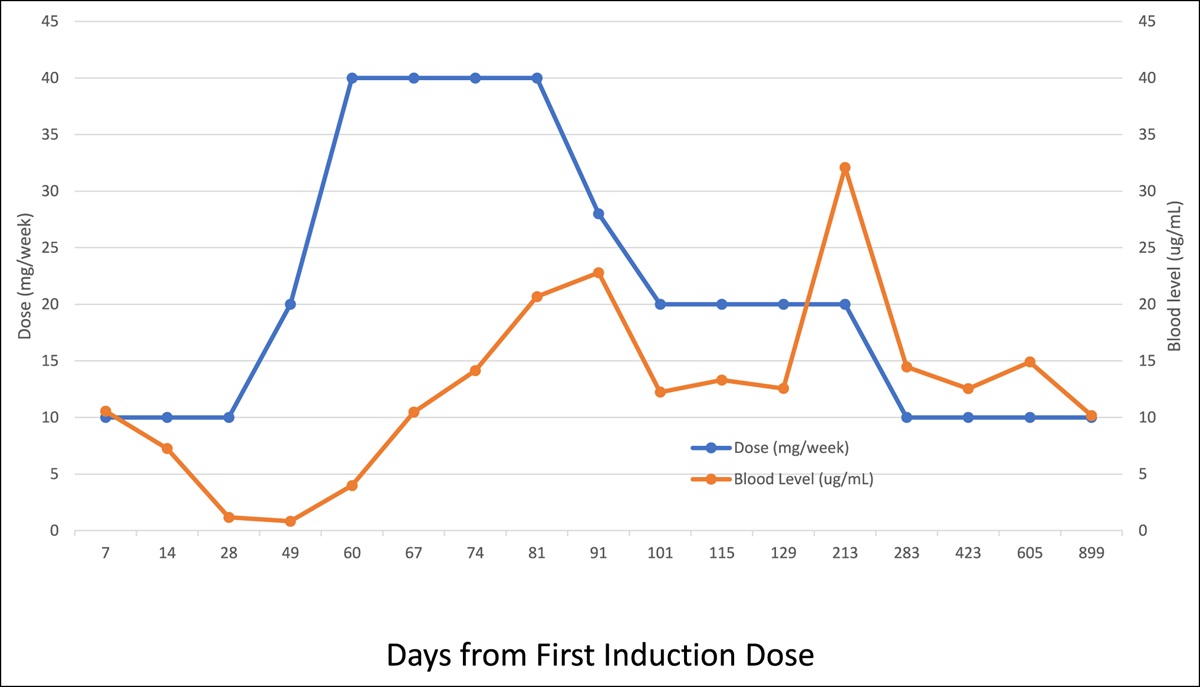
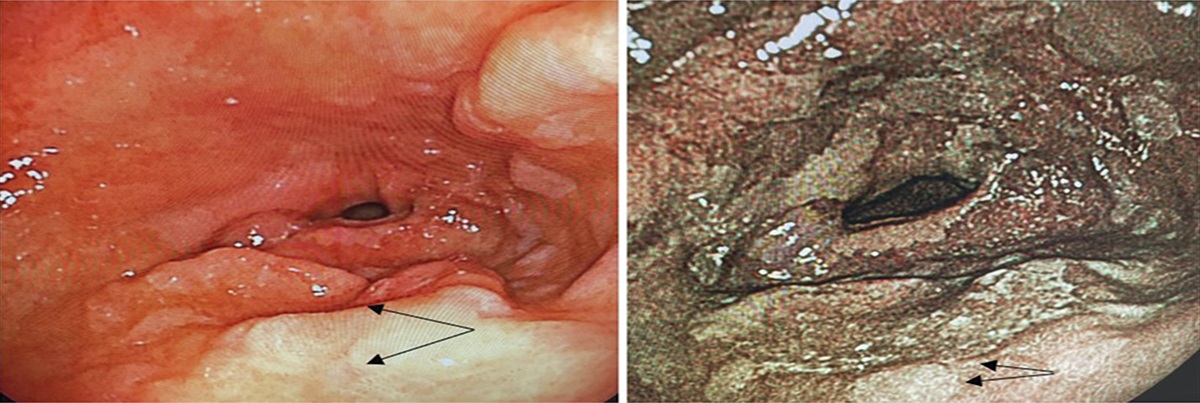
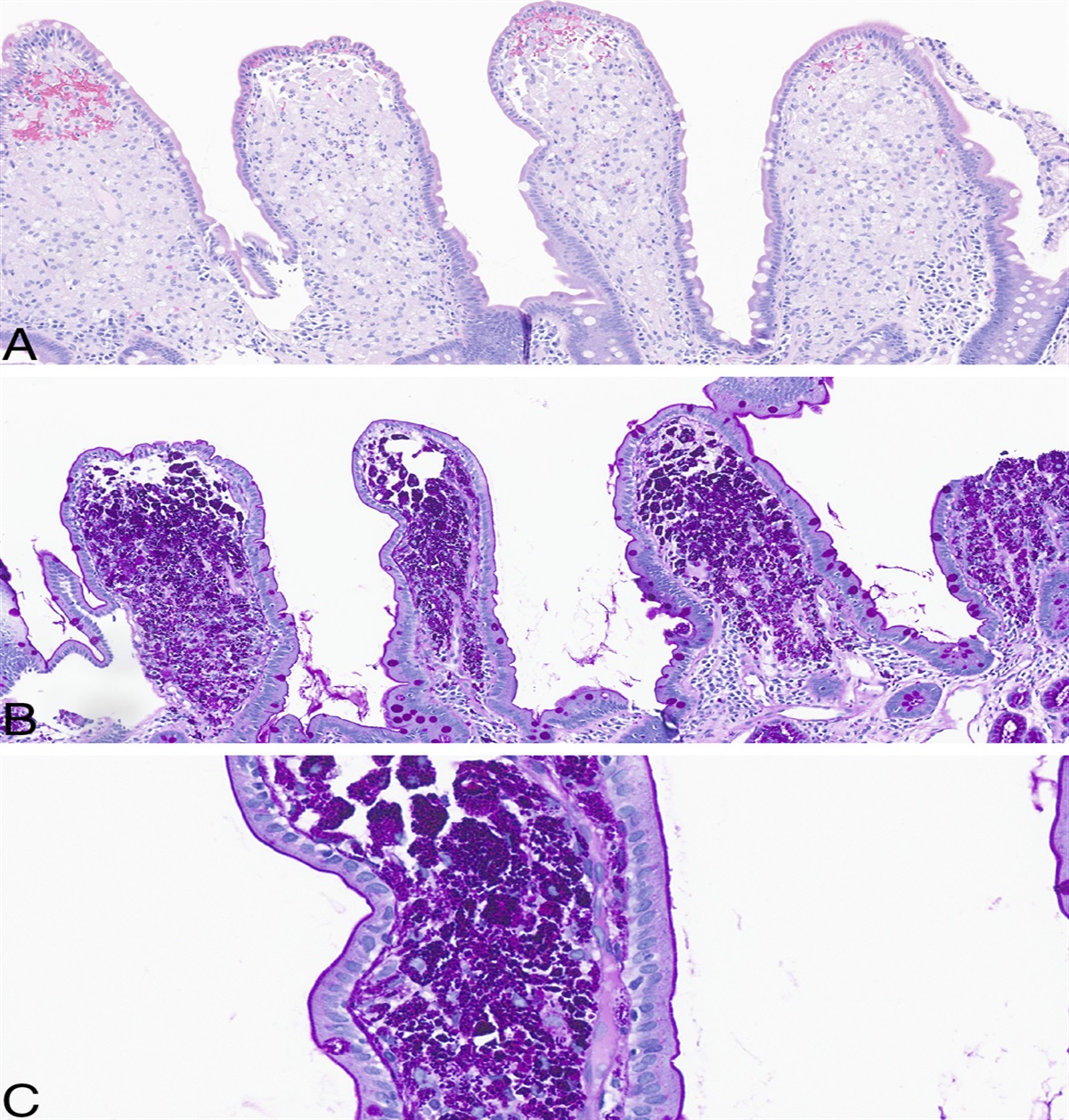
CASE REPORTThe female patient had consultation at age 10 months with symptoms of abdominal pain, partially formed stools with blood and mucus, poor weight gain, food refusal, and iron deficiency anemia that dated back to age 3 months. She was an only child, and there was no significant family history or other patient medical conditions. The patient was breastfed, and several dietary changes to reduce antigens in the mother and child (ie, cow milk protein and soy protein) were attempted with limited benefit. Physical examination was essentially normal, save for reduced weight. Without resolution of rectal bleeding and with persistence of blood work abnormalities [ie, C-reactive protein (CRP; 25.8 mg/L) and platelets (664 × 109/L); low hemoglobin (95 g/L) and albumin (34 g/L)], despite a trial of an amino acid formula, upper and lower endoscopies at age 13 months were completed along with other infectious, immune, and genetic investigations for other etiologies (eg, chronic granulomatous disease). Visually, the upper endoscopy was normal, and colonoscopy revealed a normal terminal ileum but pancolonic mucosal friability with superficial mucosal ulcerations in ascending and transverse colon segments. Histology evaluation of the upper endoscopic biopsies showed a few scattered eosinophils, with more eosinophils throughout the various regions of the colon (eosinophils/high-power field: ascending colon—120; transverse colon—30; descending colon—56; sigmoid—20; and rectum—20) without increases in other inflammatory cells. After 1 month of feeding exclusively with the amino acid formula, a second colonoscopy was completed. Visually, the appearance was similar, but histological examination of the colorectal mucosa showed evolution from the previous biopsies. Specifically, there was resolution of increased mucosal eosinophils, but focal mucosal ulceration, focal active colitis, chronic nonactive proctitis, mucosal granuloma with interspersed normal mucosa were observed in some colonic biopsies consistent with CD. Induction therapy of prednisone with maintenance sulfasalazine had a good initial clinical response, but blood testing continued to show abnormalities (ie, elevated platelets, elevated CRP, and low albumin). Symptoms worsened on tapering of the corticosteroid medication, and repeat colonoscopy and biopsies showed acute and chronic inflammatory changes. Infliximab was initiated with a 10 mg/kg induction dose given at day 0 and day 5 as inpatient, with a third induction dose given 4 weeks later as outpatient. There was a good clinical response, but an infliximab trough level (ELISA methodology) drawn before administration of the third induction dose revealed an undetectable drug level (<0.035 ug/mL) with anti-infliximab antibodies of 51 AU/mL. During the third infusion, the patient developed hives, and 2 weeks after the third infusion, no drug level was detectable and antibodies to infliximab had risen to 243 AU/mL. Infliximab was discontinued, and adalimumab was initiated with an induction dose of 20 mg subcutaneously every 2 weeks. The adalimumab drug level quickly declined (Figure 1), leading to a dose of 40 mg weekly to try to obtain levels of ≥12.5 μg/mL. After 2 months, the dose was reduced to 20 mg every second week as summarized in Table 1. The patient currently remains clinically well, with resolution of mucosal inflammation on colonoscopy 3 years after diagnosis.
 Figure 1.:
Figure 1.: Anti-TNF-alpha dosing and serum levels.
Table 1. - Adalimumab injections and blood work measures Injection Timea (day) Dose (mg) and frequency changes Drug levelb (mg/mL) Weight (kg) Height (cm) BMI (kg/m2) CRP (mg/L) ESR (mm/hr) Hb (g/L) Alb (g/L) 1 0 20aTime is the number of days from the first induction dose of adalimumab.
bDrug levels were drawn premedication.
cDenotes change in the dosing schedule.
Alb, albumin; BMI, body mass index; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Hb, hemoglobin.
Eosinophilic colitis is a form of chronic intestinal inflammation characterized by elevated mucosal eosinophils that, in infants, is commonly due to food proteins and resolves with an amino acid formula. This case illustrates that eosinophilic infiltration of colonic mucosa is not always diagnostic of allergy or infectious etiologies and that there can be evolution to an IBD diagnosis. Eosinophilic colitis is reported to predate more typical histological findings of IBD in children, speculated to be protective or part of a continuum of evolution of IBD and a distinguishing feature of VEO-IBD.7–9 The CD responded to aTNFα therapy, but even with high-dose accelerated infliximab, the patient rapidly cleared the drug and developed infliximab antibodies.
An empiric dosing schedule of 20 mg biweekly was initiated, but quickly proved inadequate with rapidly falling drug levels and increasing CRP that resolved with higher adalimumab doses. With infliximab, pretreatment predictors of rapid drug clearance by week 14. Ongoing tumor necrosis factor-alpha (TNFα) drug monitoring in well-controlled young children may allow for dose reduction and should also be considered.
In summary, in infantile IBD, there is evolution of colonic histologic changes to clarify diagnosis and loss of response to treatment using anti-TNFα medications is preventable, but requires individualization of dose intensification based on obtaining numerous trough drug level tests.
DISCLOSURESAuthor contributions: T. Gillmore collected and interpreted data and drafted the manuscript initially. C. Jimenez-Rivera collected data and reviewed the manuscript. D.R. Mack interpreted data, planned and edited the manuscript, and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Bequet E, Sarter H, Fumery M, et al. Incidence and phenotype at diagnosis of very-early-onset compared with later-onset paediatric inflammatory bowel disease: A population-based study [1988-2011]. J Crohns Colitis. 2017;11(5):519–26. 2. Kerur B, Fiedler K, Stahl M, et al. Utilization of antitumor necrosis factor biologics in very early onset inflammatory bowel disease: A multicenter retrospective cohort study from North America. J Pediatr Gastroenterol Nutr. 2022;75(1):64–9. 3. Assa A, Dorfman L, Shouval DS, et al. Therapeutic drug monitoring-guided high-dose infliximab for infantile-onset inflammatory bowel disease: A case series. J Pediatr Gastroenterol Nutr. 2020;71(4):516–20. 4. Jongsma MME, Winter DA, Huynh HQ, et al. Infliximab in young paediatric patients: It is all about the dosing. Eur J Pediatr. 2020;179(12):1935–44. 5. Xiong Y, Mizuno T, Colman R, et al. Real-world infliximab pharmacokinetic study informs an electronic health record-embedded dashboard to guide precision dosing in children with Crohn's disease. Clin Pharmacol Ther. 2021;109(6):1639–47. 6. DeBruyn JC, Huynh H, Griffiths AM, et al. Adalimumab versus infliximab in luminal pediatric Crohn's disease: One-year outcomes in a multicenter inception cohort. Gastroenterology. 2022;162(7):S-236. 7. Mutalib M, Blackstock S, Evans V, et al. Eosinophilic gastrointestinal disease and inflammatory bowel disease in children: Is it a disease continuum? Eur J Gastroenterol Hepatol. 2015;27(1):20–3. 8. Mehta P, Furuta GT. Eosinophils in gastrointestinal disorders: Eosinophilic gastrointestinal diseases, celiac disease, inflammatory bowel diseases, and parasitic infections. Immunol Allergy Clin North Am. 2015;35(3):413–37. 9. Conrad MA, Carreon CK, Dawany N, et al. Distinct histopathological features at diagnosis of very early onset inflammatory bowel disease. J Crohns Colitis. 2019;13(5):615–25.
Comments (0)