
Remember me


Lichen planus (LP) is an inflammatory skin condition that can also affect oropharyngeal and esophageal mucosa. Esophageal LP (ELP) has a prevalence of 0.19%, but is believed to be underdiagnosed.1,2 Patients usually present with dysphagia with a white mucosal surface and sloughing, whereas endoscopy usually shows ulceration, exudates, rings, and/or strictures.2 Although LP is well known within the dermatological literature, ELP has been minimally investigated in the medical literature since the first recognition in 1982 by Al-Shihabi-Jackson and Lefer in independent articles.3 It was not until 2016 that Kern et al2 proposed criteria for the diagnosis of ELP, which included clinical, endoscopic, and pathological evaluation to facilitate early detection. Furthermore, there are limited data on therapy of ELP. Although the pathogenesis of LP is incompletely understood, the Janus-activated kinase (JAK) signaling pathway is believed to play a role. Upadacitinib is a selective JAK1 inhibitor approved for use in ulcerative colitis, but may have some benefit in ELP. We present a case of refractory ELP with endoscopic and histologic response to upadacitinib after failing standard treatment.
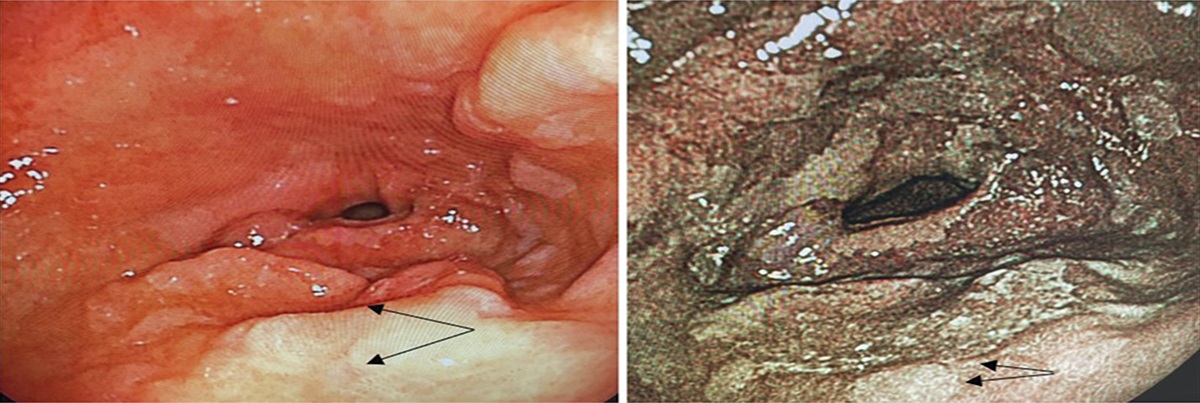
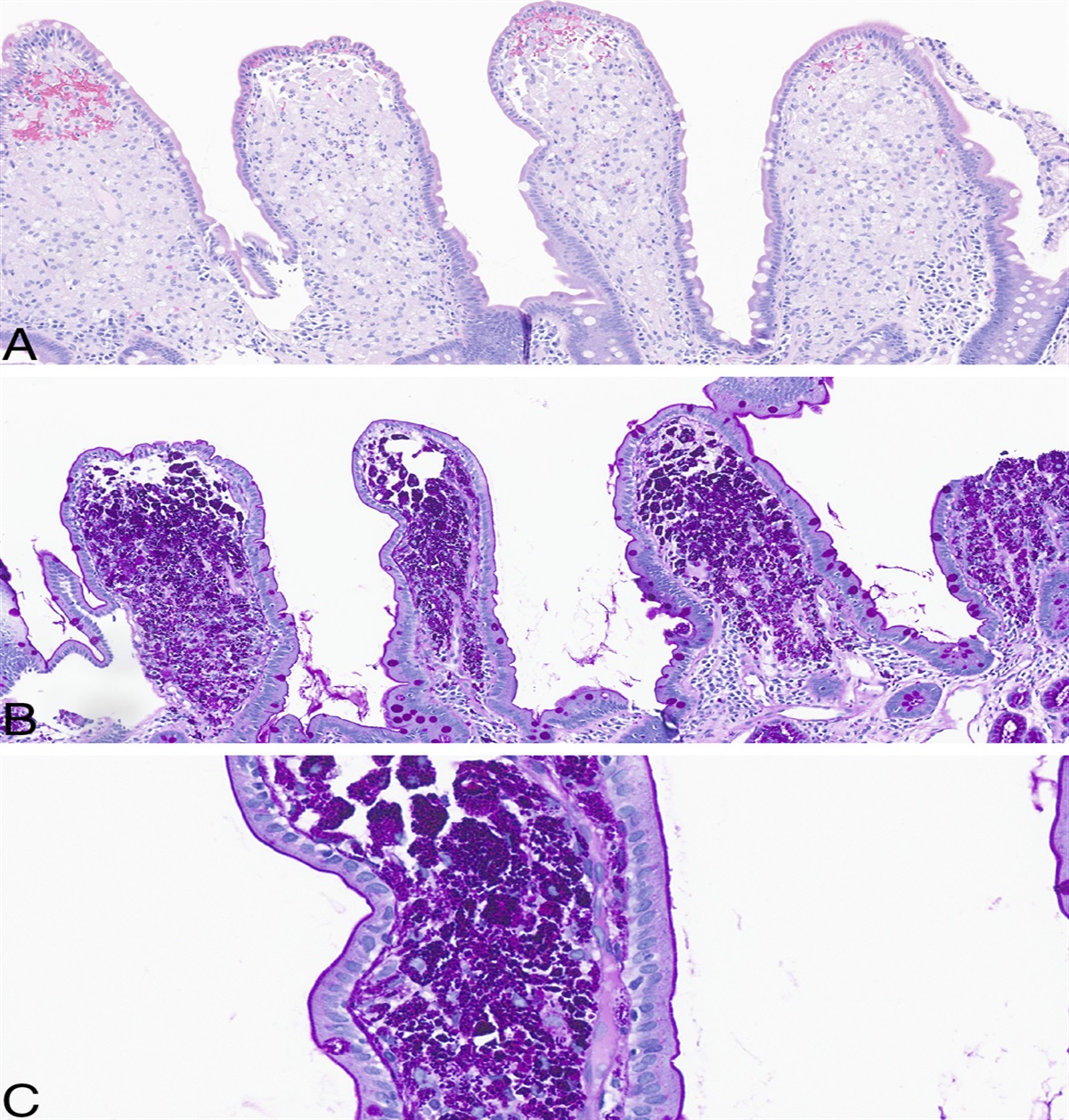
CASE REPORTA 68-year-old White woman with a history of Sjogren syndrome, LP, and peptic stricture at the gastroesophageal junction with previous dilation 4 years earlier presented with dysphagia to both liquids and solids, intermittent heartburn, regurgitation, and self-limited impactions. Her vital signs and physical examination were unremarkable. Laboratory work results, including a complete blood count and complete metabolic panel, were normal. An upper endoscopy showed a crepe-paper esophagus, severe esophagitis throughout the entire esophagus, mucosal ulceration, and multiple esophageal stenoses with a narrow 8 mm luminal diameter (Figure 1). Passage of a standard upper endoscope resulted in mucosal tearing; however, formal dilation of stenosis was not performed because of the severity of esophagitis. Esophageal biopsies revealed squamous mucosa with parakeratosis, dyskeratotic cells (Civatte bodies), and scattered lymphocytes characteristic of ELP (Figure 2). The morphologic features are those of lichenoid esophagitis and are not etiology-specific. Etiology considerations include drug-induced esophagitis, reflux esophagitis, lymphocytic esophagitis, ELP, etc. However, in a patient with a clinical history of LP, the findings are compatible with ELP. Subepithelial lamina propria is not included in the biopsy.
 Figure 1.:
Figure 1.: Esophageal lichen planus on initial diagnostic endoscopy before the initiation of therapy. (A) Proximal esophagus. (B) Mid esophagus.
 Figure 2.:
Figure 2.: Lichenoid esophagitis. Lymphocytic infiltrates, focal histiocytic aggregate (blue arrow), dyskeratosis (Civatte body, red arrow), and parakeratosis (black arrow).
Subsequently, the patient recalled having a remote history of oral lichen planus diagnosed many years ago by an oral surgeon. She was initially started on pantoprazole 40 mg twice daily and budesonide oral slurry (1 mg PO BID) with limited response and recurrent fibrostenotic disease of the esophagus. Then, with comanagement by gastroenterology and dermatology, she was initiated on mycophenolate 500 mg daily. With limited symptomatic improvement, the mycophenolate was increased to 2000 mg twice a day. Her medications were reviewed and included amlodipine, hydrochlorothiazide, losartan, metformin, cevimeline, and fenofibrate. Hydrochlorothiazide was discontinued because of its association with lichen planus. Cevimeline was held for 3 months without endoscopic improvement. Approximately 11 years after diagnosis of oral lichen planus, she had been started on an ace inhibitor, which was later replaced with losartan. Given the association of LP with HCV infection, HCV Ab was checked and found to be negative.
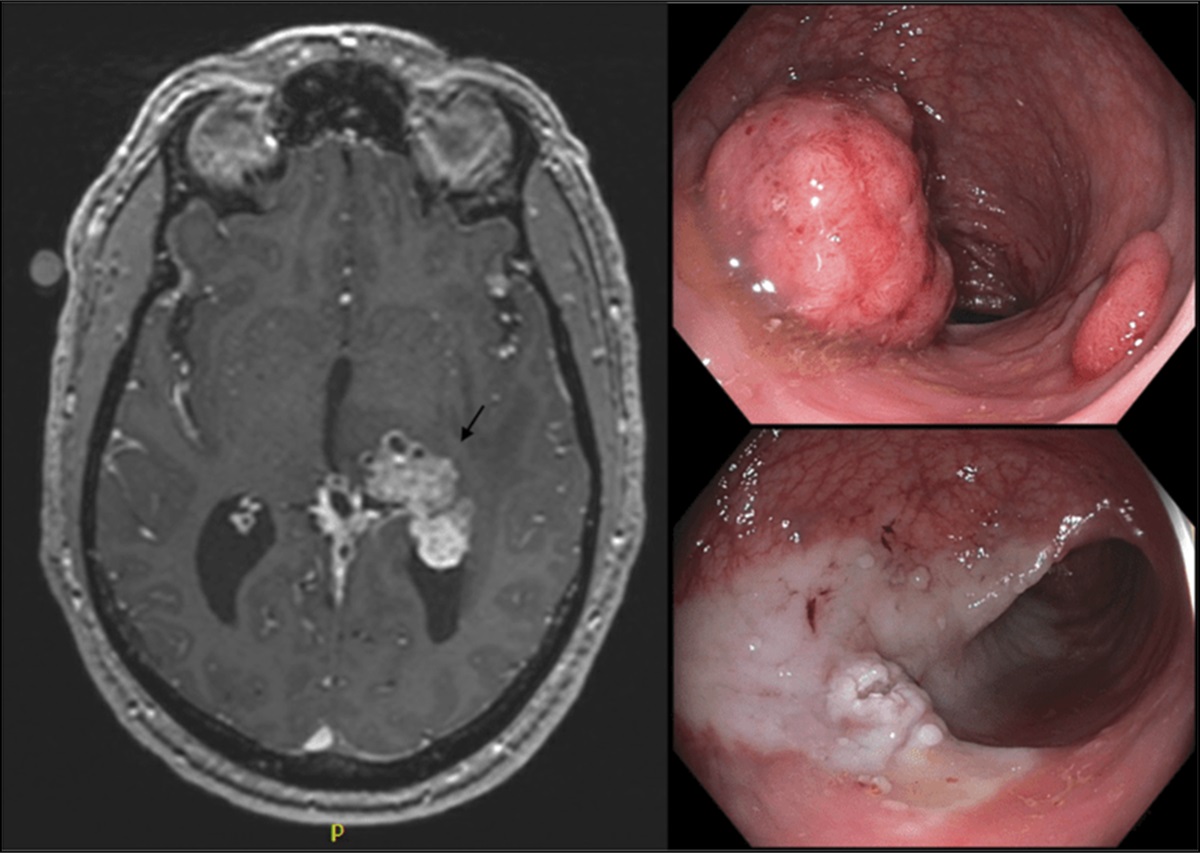
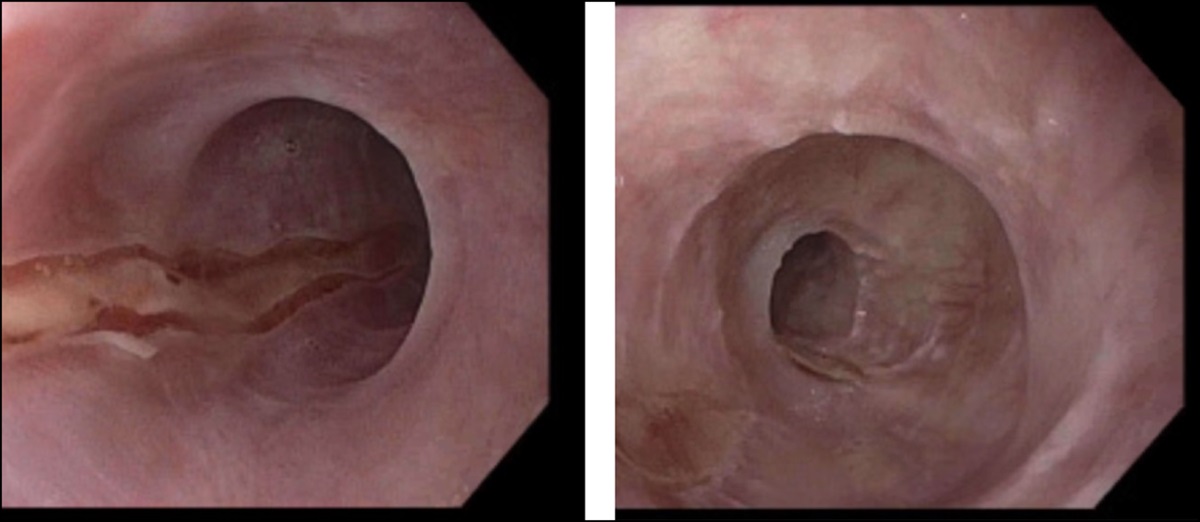
Despite treatment, she continued to lack both histologic and symptomatic improvement and remained limited to a soft and liquid diet resulting in a 20 lb weight loss. Ultimately, she was started on monotherapy with upadacitinib 30 mg daily. This resulted in marked symptomatic recovery with repeat endoscopy 3 months later showing dramatic macroscopic and histologic improvement, with only some residual fibrostenotic disease remaining (Figures 3 and 4).
 Figure 3.:
Figure 3.: Follow-up endoscopy performed after 12 weeks of upadacitinib treatment. (A) Proximal esophagus. (B) Mid esophagus.
 Figure 4.:
Figure 4.: Esophageal mucosa after treatment. Most biopsy fragments show near-normal esophageal mucosa (left panel). Focal areas show parakeratosis (black arrow).
DISCUSSIONLichen planus is a common chronic inflammatory condition with known extracutaneous manifestations, such as esophageal involvement. Reported cases of ELP show female predominance, which is believed to be secondary to an association between oral and vulvar LP.4 Esophageal lichen planus has been documented to have malignant transformation to squamous cell carcinoma (SCC) in 4 patients, thus suggesting that it is a premalignant condition.4 Dysphagia is the most common symptom noted for ELP, but transformation to SCC has been documented despite minimal symptoms.4 Thus, early diagnosis and treatment is essential.
Current diagnostic criteria and management have not been standardized. Diagnosis is often delayed because of rarity and unfamiliarity of the disease, which requires a high clinical index of suspicion. Endoscopic findings must be correlated with clinical presentation. For instance, ELP typically involves the proximal and middle esophagus, whereas reflux esophagitis is distal.3,5 However, as signified by our patient, this is not always the case. Furthermore, the patient described in this report had a previous stricture of gastroesophageal junction requiring prior dilation. Some providers note that the gastroesophageal junction should be preserved in ELP assisting with diagnosis,3,5 which unfortunately was not the case for our patient. Other comorbidities and delayed diagnosis with progressive disease can confound the endoscopy findings, making it harder to diagnose ELP. Other indicative findings include erosions, ulcerations, stenosis, and reticulated white streaks, which were all seen on our patient's endoscopy.
Diagnostic criteria have been proposed and assessed in a study reviewing 32 patients with a diagnosis of ELP.2 The authors recommend including endoscopy, histopathology, and direct immunofluorescence as a means to diagnosis.2 Endoscopy was considered diagnostic if white rough mucosal surface, denudation/sloughing, and spontaneous tearing of the mucosa were present.2 Esophageal stenosis, gastroesophageal junction involvement, or length/location of esophagitis was not included in the diagnostic criteria. Histopathological criteria included detachment of the epithelium, lymphocytic infiltrate, and intraepithelial apoptosis.2 Direct immunofluorescence was diagnostic if strong fibrinogen deposits were present on the basement membrane.2 Of the 32 patients reviewed, 20 fulfilled the criteria to meet ELP diagnosis.2 Given the small sample size, more data need to be collected before standardizing this diagnostic approach; however, it does give us a glimpse into the potential workup and necessary evaluation.
Multimodal treatment is typically used in ELP with medical therapy and endoscopic dilation. Systemic or topical steroids are first-line, with efficacy estimated at 60%–70%. Several case reports have documented control of disease with topical steroids (eg, fluticasone or budesonide) with possible preference to the use of budesonide because of high first-pass effect and reduced systemic side effects.2 Other medical therapies include azathioprine, tacrolimus, cyclosporine, mycophenolate, rituximab, adalimumab, tofacitinib, and acitretin; however, data for these therapies are limited. To date, there are only 2 cases reported in the literature of successful treatment of oroesophageal LP with upadacitinib.6,7 Given the profound improvement seen in our patient, upadacitinib may offer another alternative for these difficult-to-treat patients. Medical management and endoscopic dilation are recommended when patients have uncontrolled ELP and scarring strictures. We suggest endoscopic follow-up approximately 3 months after systemic treatment is started and when disease control is achieved, annual surveillance to monitor disease activity. However, it is important to note that endoscopy can exacerbate oral lesions.5 Duration of treatment with steroid-sparing immunosuppressants for patients in remission is unknown. In addition, adjunctive treatment with acid reflux prevention may be helpful to prevent the Koebner phenomenon and protect the esophagus from further damage.4
Esophageal lichen planus should be considered in the differential for all adult female patients with dysphagia. Dysphagia is the most commonly reported symptom; however, other notable symptoms include odynophagia, weight loss, hoarseness, choking, and epigastric pain.3 In a review of 79 ELP cases, 89% of patients also had extraesophageal LP in the oral cavity3; thus, obtaining detailed physical examination and clinical history is essential. Prompt diagnosis is necessary to prevent long-term sequala (eg, ulcers, strictures, and malignant transformation to SCC) and reduced quality of life. Further information regarding superiority data and duration of treatment may help reduce recurrences and the need for repeated esophageal dilations. Working closely with dermatology and a dermatopathologist is ideal to facilitate rapid diagnosis and alter the disease course.
DISCLOSURESAuthor contributions: EC Becker and M. Mavilia-Scranton wrote the manuscript. J. Finch, M. Yu, and H. Rezaizadeh revised the manuscript for intellectual content. EC Becker, M. Mavilia-Scranton, J. Finch, M. Yu, and H. Rezaizadeh approved the final manuscript. H. Rezaizadeh is the article guarantor.
Financial disclosure: None to report.
Previous presentation: This case was presented at the ACG Annual Scientific Meeting in Charlotte, North Carolina, October 21-26, 2022.
Informed consent was obtained for this case report.
REFERENCES 1. Jacobs J, Kukreja K, Camisa C, et al. Demystifying esophageal lichen planus: A comprehensive review of a rare disease you will see in practice. Am J Gastroenterol 2022;117(1):70–7. 2. Kern JS, Technau-Hafsi K, Schwacha H, et al. Esophageal involvement is frequent in lichen planus: Study in 32 patients with suggestion of clinicopathologic diagnostic criteria and therapeutic implications. Eur J Gastroenterol Hepatol 2016;28:1374–82. 3. Oliveira JP, Uribe NC, Abulafia LA, Quintella LP. Esophageal lichen planus. An Bras Dermatol 2015;90(3):394–6. 4. Fox LP, Lightdale C, Grossman M. Lichen planus of the esophagus: What dermatologists need to know. J Am Acad Dermatol 2011;65(1):175–83. 5. Madhusudhan KS, Sharma R. Esophageal lichen planus: A case report and review of literature. Indian J Dermatol 2008;53(1):26–7. 6. Kooybaran N, Petzold G, Ströbel P, et al. Alleviation of erosive oral and esophageal lichen planus by the JAK1 inhibitor upadacitinib. J Dtsch Dermatol Ges 2021;19(12):1778–80. 7. Balestri R, Bortolotti R, Rech G, et al. Treatment of oral erosive lichen planus with Upadacitinib. JAMA Dermatol 2022;158(4):457–8.
Comments (0)