
Remember me


Dual biologic therapy can improve clinical, biomarker, and endoscopic outcomes in patients with complicated or refractory inflammatory bowel disease (IBD) in whom multiple biologics had failed.1,2 In addition, infliximab was shown to be effective in the treatment of severe gastrointestinal bleeding in Crohn's disease.3,4 In this case, we showed the role of dual biologics in refractory Crohn's disease in a critical condition.
CASE REPORTA 38-year-old man presented with a history of Crohn's disease for 5 years (Montreal A2L3B2B3). He had undergone right hemicolectomy and 6 other surgeries for colonic obstruction, enterocutaneous fistulas, and perforations. He was a primary nonresponder of vedolizumab and under adalimumab treatment for 1 year. He was brought to our emergency department because of periumbilical pain and diarrhea of 5 days’ duration (day 0).
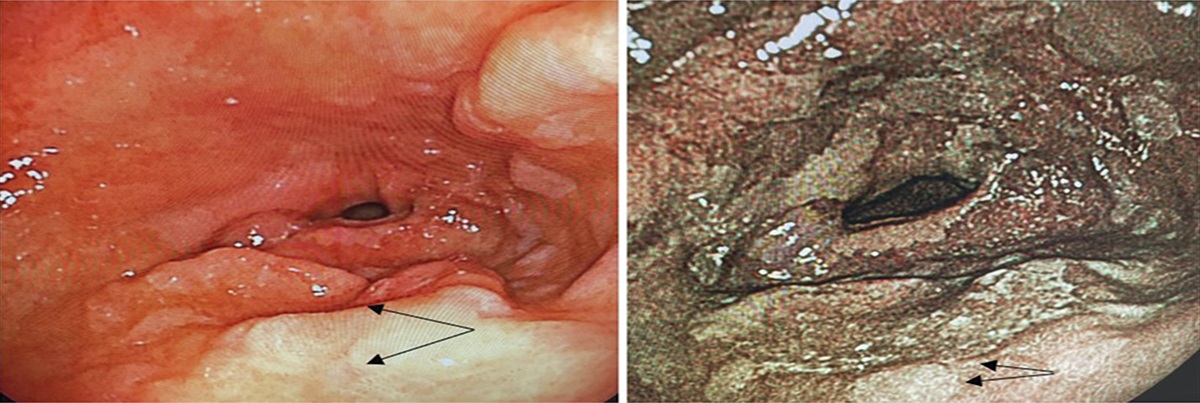
Colonoscopy showed multiple small intestinal ulcers (0.5–1.5 cm) near the anastomotic site (Figure 1). Biopsy revealed ulcerated small intestine mucosa with necrotic debris, marked acute and chronic inflammation, crypt microabscesses, and granulation tissue formation, consistent with Crohn's disease. No definite viral inclusions, granulomas, or parasites were observed. Immunohistochemical staining for cytomegalovirus was negative. Methylprednisolone 40 mg intravenous (IV) QD, ceftriaxone 1 g IV Q12H, and tramadol 37.5 mg + acetaminophen 325 mg 1 pc PO Q6H were prescribed. Because the drug level and anti-drug antibody assays of adalimumab were not available, we shortened the interval of adalimumab to 1 week. Days later, the diarrhea and abdominal pain had subsided and the steroid dose was tapered to 20 mg/d.
 Figure 1.:
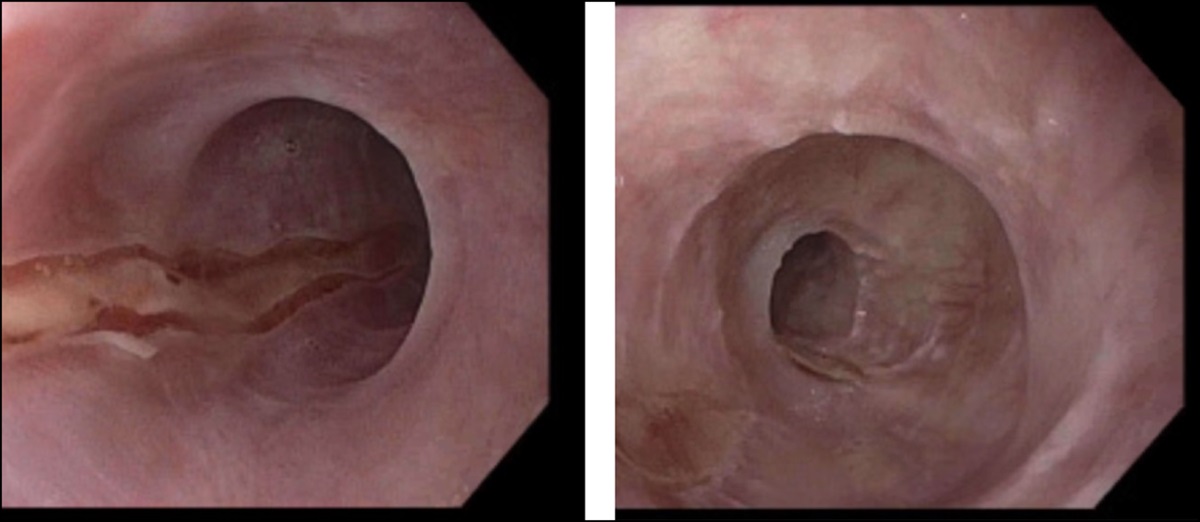
Figure 1.: Colonoscopies. (A and B) Multiple small intestinal deep ulcers, 0.5–1.5 cm, near an anastomotic site on day 2, (C) irregular shaped shallow ulcer, 2 cm, at the terminal ileum, near an anastomotic site at 7 months postepisode.
He had intermittent fever, chills, and progressive abdominal pain on day 17, and the antibiotics were changed to IV cefepime 2 g Q12H. However, he had septic shock, disseminated intravascular coagulation, and signs of peritonitis 6 days later. Abdominal computed tomography showed pneumoperitoneum, features of peritonitis, dirty ascites, dilated small intestine, terminal ileal wall thickening, and deep ulcers, suggesting terminal ileal obstruction and perforation near the anastomotic site (Figure 2). The final diagnosis was refractory Crohn's disease with terminal ileal perforation, bleeding, shock, and disseminated intravascular coagulation.
 Figure 2.:
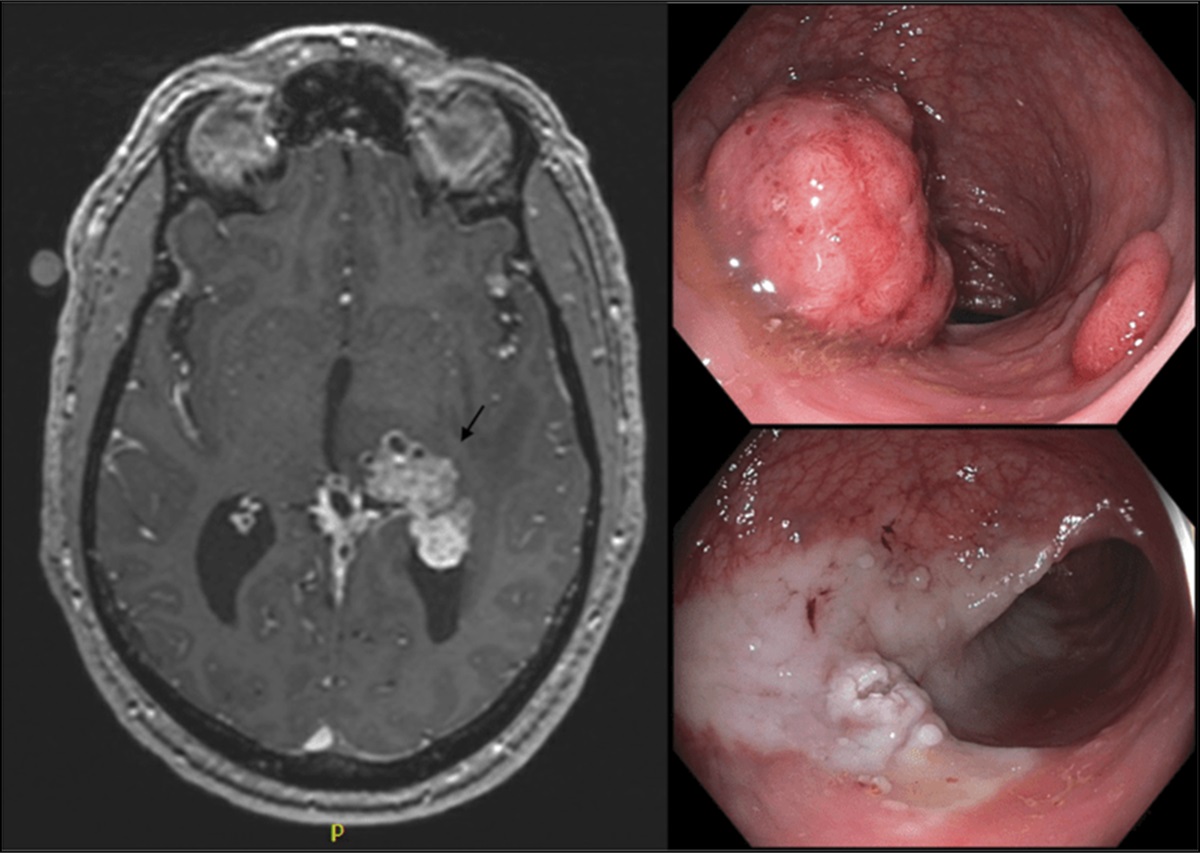
Figure 2.: Imaging examinations. (A–C) Abdominal CT showing pneumoperitoneum (white arrows), dilated small intestine (white star), terminal ileal wall thickening (green arrow), and deep ulcers (red arrow), suggesting terminal ileal obstruction and perforation near an anastomotic site (day 23). (D) MRI showing regression of intra-abdominal free air, terminal ileal inflammation, and dilated small intestine (day 68). (E) CTE showing regression of small intestinal inflammation and dilatation (day 145). CT, computed tomography; CTE, computed tomography enterography; MRI, magnetic resonance imaging.
The patient refused surgical treatment and signed the do-not-resuscitate form because of the disease course and high risk of short bowel syndrome after surgical resection. Percutaneous needle decompressions was performed with a 16 G venous catheter and syringe filled with water (Figure 3). The patient was placed on nil per os, with IV antibiotics (teicoplanin and imipenem/cilastatin kabi) and antifungal drugs (anidulafungin). Total parenteral nutrition (SmofKabiven®) was administered for nutrition support and morphine for pain control. Kidneys, ureters, and bladder (KUB) radiographs revealed extremely dilated bowel loops on day 25 (Figure 4). His condition was aggravated by passage of massive bloody stools from day 34. Meanwhile, the patient refused endoscopic examinations. The nasogastric tube did not contain fresh blood or coffee-ground material. Under the impression of Crohn's disease-related small intestinal bleeding, IV infliximab 300 mg was prescribed on day 35. The bleeding subsided 3 days later, but he still complained of severe abdominal pain and distension. Air leakage still occurred during percutaneous needle decompression. Out-of-class switch was a more reasonable option, and IV ustekinumab 390 mg was then added on day 39. The abdominal pain and distension had subsided 2 days later. He received a second dose of IV infliximab 300 mg on day 46.
 Figure 3.:
Figure 3.: Percutaneous needle decompressions. A 16 G venous catheter and a syringe filled with water were used to release the intra-abdominal free air.
 Figure 4.:
Figure 4.: Kidneys, ureters, and bladder (KUB) radiograph. (A) Dilated bowel loops (day 25). (B) Minimal bowel loop dilatation in the central part of the abdomen (day 67).
We verified an improvement in KUB findings, with the absence of any further peritoneal signs. Consequently, he had a liquid diet on day 48 and a soft diet/full diet on day 50. KUB radiographs showed minimal bowel loop dilatation on day 67 (Figure 4). Magnetic resonance imaging showed significant regression of intra-abdominal free air, terminal ileal inflammation, and dilated small intestine on day 68 (Figure 2). His Crohn's Disease Activity Index decreased from 509 to 83 points. The Harvey-Bradshaw Index improved from 22 to 4 points. C-reactive protein decreased from 262.25 to 9.33 mg/L. Under stable conditions, the patient was discharged on day 70.
He was maintained on IV infliximab 300 mg Q8W and IV ustekinumab 390 mg Q8W after standard induction in the outpatient department. Follow-up computed tomography enterography at 2 months postdischarge showed significant regression of small intestinal inflammation and dilatation (Figure 2). However, a colonoscopy at 7 months postepisode revealed a 2 cm shallow ulcer over the terminal ileum, near the anastomotic site (Figure 1). After 1-year dual biological treatment, he continued ustekinumab and was under steroid-free clinical remission.
DISCUSSIONDespite receiving the best available medical or surgical treatments, many patients with IBD experience persistent and progressive disease activity. These individuals are often categorized as having difficult-to-treat IBD, requiring additional therapeutic strategies.5 The potential of dual biologics or combining biologics with small molecules to overcome the limitations of advanced therapy is an emerging hope for this subgroup of patients. Initial evidence suggests that this approach is generally safe.6 A systematic review and meta-analysis have suggested that dual biologic therapy might be a viable option for patients with highly selected, refractory IBD at specialized centers. However, it is worth noting that the outcomes of the included studies showed significant heterogeneity.7 In the most recent review focusing on the role of dual biologic therapy in IBD treatment, the authors highlighted its positive impact on reducing morbidity.8
The potential efficacy should be weighed against the risk of possible adverse events. It is essential to carefully assess the potential efficacy against the risk of adverse events when considering these therapies. The choice of regimen should take into account factors such as disease severity, complications, medication history, safety profiles of the biologics, and extraintestinal manifestations. Owing to their favorable safety profiles, vedolizumab and ustekinumab are commonly included as part of dual biologic therapy regimens. Nonetheless, more studies are needed in this evolving field to provide a more comprehensive comparison of different biologic combinations and their associated safety profiles. We chose infliximab because it has been shown to be effective for severe gastrointestinal bleeding in Crohn's disease.9–12 The patient had primary nonresponse to vedolizumab and secondary loss of response to adalimumab, even after shortening the interval of adalimumab to 1 week. Another class of biologic was a more reliable treatment in the critical condition, so we prescribed ustekinumab as the second combined biologic.
Emergency percutaneous decompression in tension pneumoperitoneum is not a definitive treatment; it is only a method to bridge the time gap to definitive surgical repair.13 Percutaneous decompression was performed in our patient to release the abdominal pressure and for symptomatic relief. Severe inflammation and ulcers of the terminal ileum led to obstruction and perforation; therefore, the condition improved after the commencement of dual biologics.
This patient underwent 2 biological treatments and 7 surgeries in the past 5 years, resulting in the retention of approximately 2 m of small intestine. This profile aligns with the latest definition of difficult-to-treat IBD established during an international consensus meeting.5 The arduous therapeutic journey has subjected him to considerable stress and painful memories, leading to his decision to decline further surgical interventions. Dual biologics played a pivotal role in saving his life during this critical period and have since allowed him to lead a relatively normal life. In patients with refractory, complicated, or critical Crohn's disease, dual biologics could prove an effective and safe option. In conclusion, dual biologic therapy can be an effective treatment option for patients with difficult-to-treat IBD who are in a critical condition and have declined surgical intervention. Nonetheless, it is imperative to meticulously assess the potential benefits and risks and limit its use to experienced medical centers.
DISCLOSURESAuthor contributions: PH Le created the therapeutic plan, treated the patient, and drafted the manuscript. MY Su, CT Chiu, and YK Tsou collected and analyzed the data. CM Chen read radiological images. PH Le and CJ Kuo treated the patient and critically revised the manuscript. All authors have read and approved the manuscript.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Yang E, Panaccione N, Whitmire N, et al. Efficacy and safety of simultaneous treatment with two biologic medications in refractory Crohn's disease. Aliment Pharmacol Ther. 2020;51(11):1031–8. 2. Privitera G, Onali S, Pugliese D, et al. Dual targeted therapy: A possible option for the management of refractory inflammatory bowel disease. J Crohns Colitis. 2020;15(2):335–9. 3. Chowdhury M, Kudara N, Chiba T, et al. Evaluation of infliximab effects on gastrointestinal bleeding in Crohn's disease using double-balloon endoscopy. Case Rep Gastroenterol. 2009;3(2):193–7. 4. Aniwan S, Eakpongpaisit S, Imraporn B, Amornsawadwatana S, Rerknimitr R. Infliximab stopped severe gastrointestinal bleeding in Crohn's disease. World J Gastroenterol. 2012;18(21):2730–4. 5. Parigi TL, D'Amico F, Abreu MT, et al. Difficult-to-treat inflammatory bowel disease: Results from an international consensus meeting. Lancet Gastroenterol Hepatol. 2023;8(9):853–9. 6. Alayo QA, Fenster M, Altayar O, et al. Systematic review with meta-analysis: Safety and effectiveness of combining biologics and small molecules in inflammatory bowel disease. Crohns Colitis 360. 2022;4(1):otac002. 7. Ahmed W, Galati J, Kumar A, et al. Dual biologic or small molecule therapy for treatment of inflammatory bowel disease: A systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20(3):e361–79. 8. McCormack MD, Wahedna NA, Aldulaimi D, Hawker P. Emerging role of dual biologic therapy for the treatment of inflammatory bowel disease. World J Clin Cases. 2023;11(12):2621–30. 9. Ando Y, Matsushita M, Kawamata S, Shimatani M, Fujii T, Okazaki K. Infliximab for severe gastrointestinal bleeding in Crohn's disease. Inflamm Bowel Dis. 2009;15(3):483–4. 10. Belaiche J, Louis E. Severe lower gastrointestinal bleeding in Crohn's disease: Successful control with infliximab. Am J Gastroenterol. 2002;97(12):3210–1. 11. Tsujikawa T, Nezu R, Andoh A, et al. Inflixmab as a possible treatment for the hemorrhagic type of Crohn's disease. J Gastroenterol. 2004;39(3):284–7. 12. Kocaman O, Aygün C, Konduk T, Celebi A, Sentürk O, Hülagü S. Infliximab treatment of massive upper gastrointestinal bleeding in gastroduodenal Crohn's disease. Turk J Gastroenterol. 2008;19(3):197–8. 13. Chiapponi C, Stocker U, Körner M, Ladurner R. Emergency percutaneous needle decompression for tension pneumoperitoneum. BMC Gastroenterol. 2011;11:48.
Comments (0)