
Remember me


Eosinophilic gastrointestinal diseases (EGID) are disorders of chronic eosinophilic infiltration of gastrointestinal (GI) tissue.1 Eosinophilic disease of the GI system beyond the esophagus is an uncommon diagnosis involving infiltration of the mucosal, serosa, or muscular layer of the GI tract.2 Prevalence of EGID is currently 6.3/100,000 persons for eosinophilic gastritis, 8.4/100,000 persons for eosinophilic enteritis, and 3.3/100,000 persons for eosinophilic colitis.3 The incidence of these cases is increasing, yet the treatments remain limited.4 This can cause malabsorption, strictures, obstruction, and pain. Although rare, cases of ulcers in EGID have been reported.5 Avoidance of common food triggers and corticosteroids are the mainstay of treatment for EGID. When these therapies fail, there only limited reports of successful options for treatment. In addition, elimination diets can be challenging to maintain, and prolonged or recurrent corticosteroids have many potential side effects. Beyond these therapies, there is little evidence for other treatments for persistent or refractory disease. Case reports of the use of other therapies for EGID have been published, but large-scale data are not yet available. Dupilumab is a therapy that has been used for refractory cases of eosinophilic esophagitis, but there are limited data on other EGIDs.6 We present a rare case of diffuse EGID involving the esophagus, stomach, small intestine, and colon with severely symptomatic duodenal ulcers and pyloric stenosis, which was successfully treated with dupilumab, obtaining both histologic and symptomatic improvement.
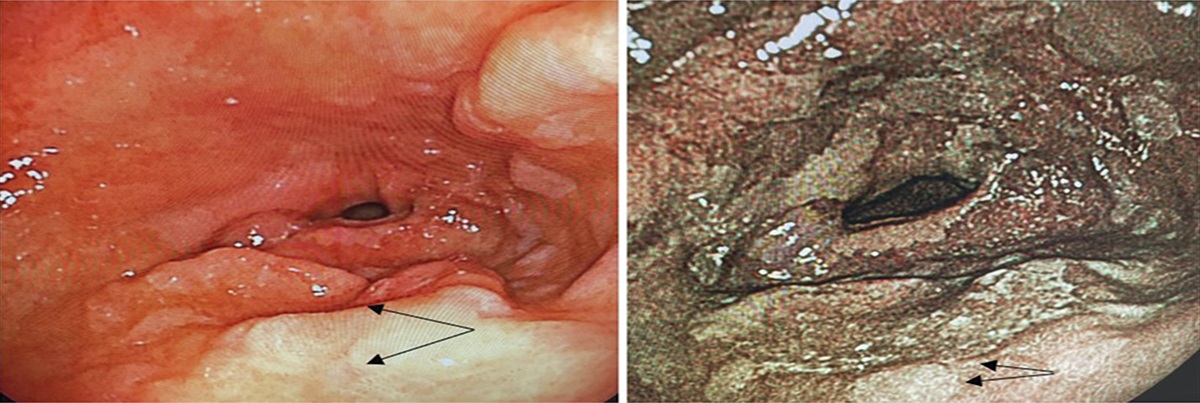
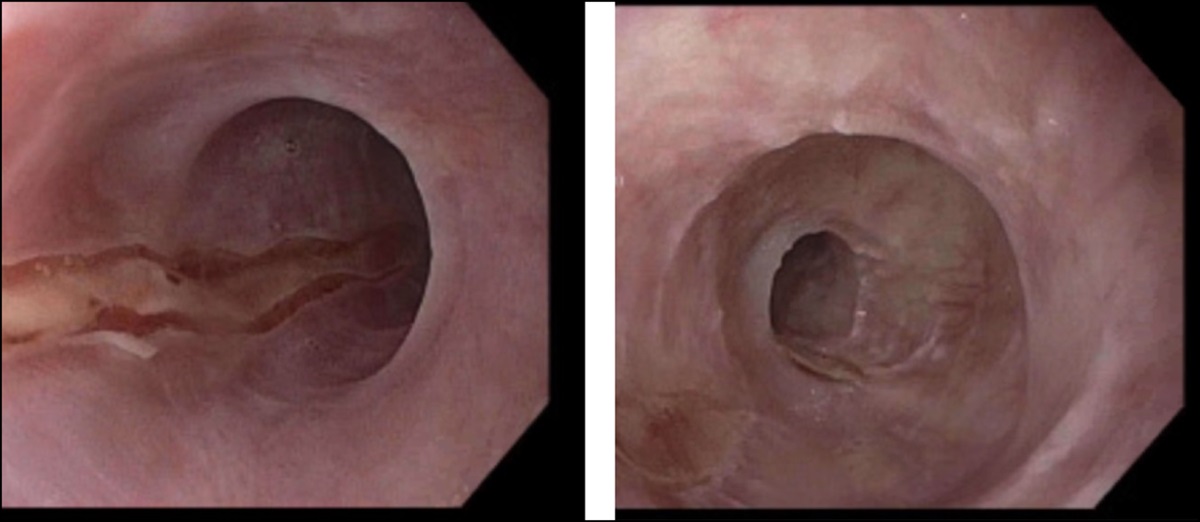
CASE REPORTA 22-year-old woman presented to her primary care provider while working in the Mediterranean and Italy with 6 months of nausea, vomiting, abdominal pain, and weight loss. On physical examination, she had tachycardia and epigastric abdominal tenderness. Laboratory evaluation demonstrated an absolute eosinophil count of 659 cells/μL, and a computed tomography scan noted thickening of the gastric and duodenal mucosa. Reflux esophagitis and a clean-based duodenal ulcer were identified on esophagogastroduodenoscopy (EGD), although no biopsies were obtained. Her initial management was treatment with a proton-pump inhibitor and antibiotics for a suspected Helicobacter pylori infection. She returned from overseas, and her symptoms persisted. A repeat EGD and colonoscopy showed traversable pyloric stenosis but otherwise normal-appearing mucosa (Figure 1). Biopsies demonstrated mild chronic inflammation and increased eosinophils found in the esophagus, stomach, duodenum, terminal ileum, and large intestine. The number of eosinophils was not reported by pathology.
 Figure 1.:
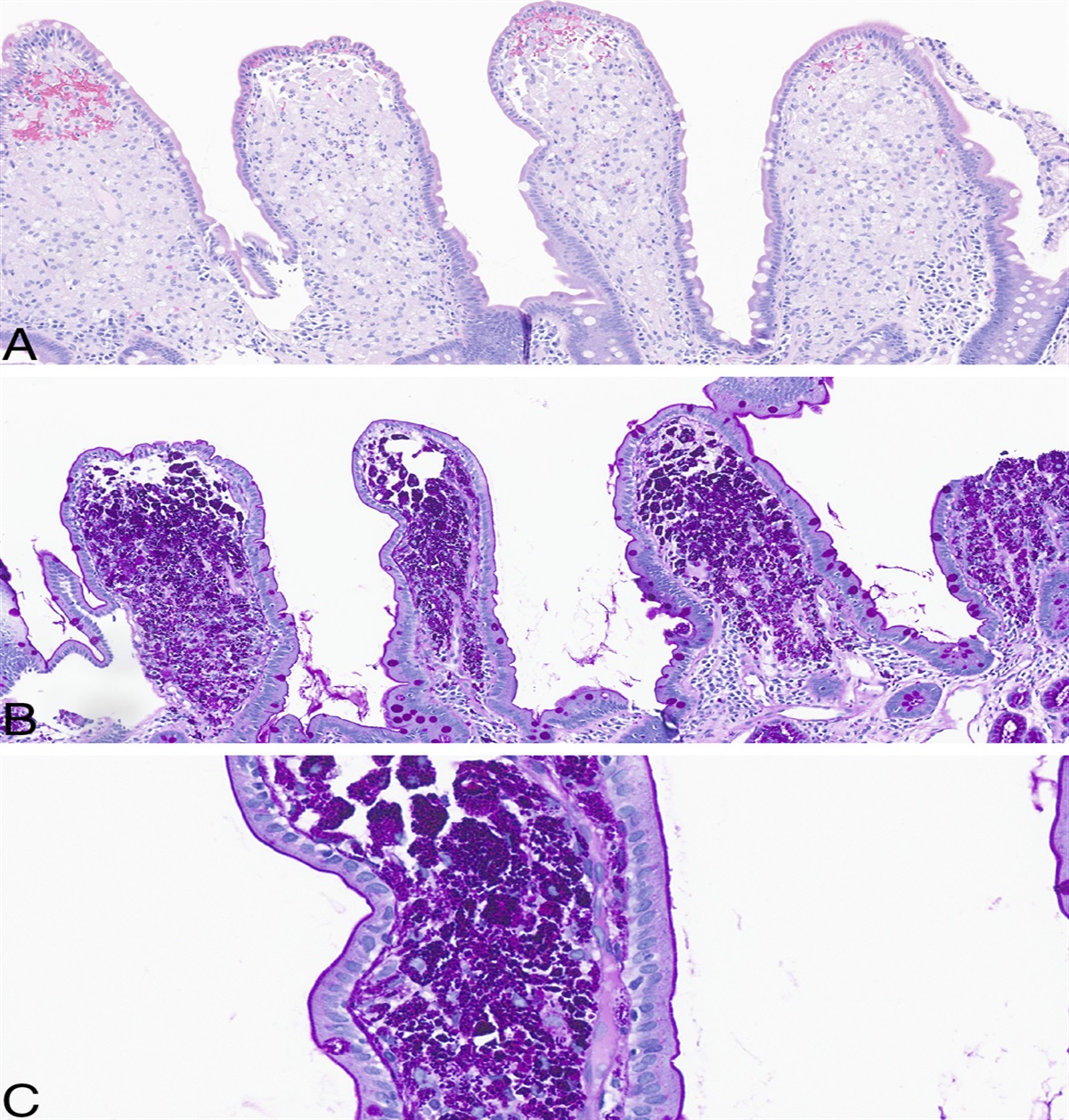
Figure 1.: (A) Stomach before treatment demonstrating diffuse collections of eosinophils and intraepithelial eosinophils, magnification 400×, stained with hematoxylin and eosin (H&E). (B) Pretreatment esophagus with diffuse eosinophils and eosinophilic microabscesses (arrows), stained with hematoxylin and eosin (H&E), magnification 400×. (C) Esophagus post-treatment with rare intraepithelial eosinophils, stained with H&E, magnification 200×. (D) Pylorus before dupilumab treatment, visualized with endoscopy. (E) Pylorus post-treatment with dupilumab, visualized with endoscopy.
Evaluation for infections, vasculitis, and malignancy to include stool ova and parasites, viral hepatitis A, B, and C, H. pylori, human immunodeficiency virus, toxocariasis, strongyloidiasis, ANCA, and peripheral flow cytometry was negative. She was treated for EGID with prednisone with initial symptomatic improvement with cessation of pain, nausea, emesis, and weight loss. All these symptoms returned 4 months after cessation of therapy. A repeat EGD showed gastric biopsies with > 40 eosinophils/high-powered field (hpf) and esophagus biopsies with > 50 eosinophils/hpf. She was admitted to the hospital with a perforated duodenal ulcer, weight loss, and inability to tolerate food. She was started on total parenteral nutrition. Because of concern about the use of steroids with a perforated ulcer, there was a multidisciplinary discussion with the allergy, gastroenterology, and general surgery services, and she was initiated on dupilumab. Her symptoms resolved, and she returned to a regular diet. A repeat EGD 8 weeks after initiation of dupilumab showed a small area of erythema in the gastric cardia with focally increased eosinophils of 30 cells/hpf, but the remaining gastric mucosa biopsies were negative for increased eosinophils (Figure 1).
DISCUSSIONEGID beyond the esophagus involving infiltration of the mucosal, serosa, or muscular layer of the GI tract with eosinophils is a rare diagnosis. EGID can result in severe symptoms including pain, malnutrition, intestinal fibrosis, or strictures.7 Although EGID localized to the esophagus, eosinophilic esophagitis, have been widely studied with several approved therapies, treatment for more diffuse EGID is often more challenging.6 Corticosteroids are commonly used, but prolonged use risks significant side effects, and their efficacy can be mixed. A food elimination diet, also frequently used as a therapy for EGID, is often difficult to maintain and frequently unsuccessful. There is limited evidence for treatment of persistent or refractory disease. Case reports and small case series have investigated the effects of therapies such as vedolizumab, omalizumab, and benralizumab with varying success.4,7,8 These treatments are hampered by an incomplete understanding of the underlying pathophysiology of EGID. Dupilumab targets the interleukin-4 receptor alpha subunit, antagonizes IL-4 and -13, with impact on IgE production and alternatively activated macrophages.9,10 It was studied, and FDA approved for use in refractory eosinophilic esophagitis with case reports of clinical success in EGID.6,11 In addition, dupilumab has been used as treatment of eosinophilic esophagitis and demonstrated efficacy beyond the distal esophagus in pediatric population.6
In this case, mainstays of typical treatment failed, and eosinophilic disease persisted. With the novel use of dupilumab, our patient was able to return to an asymptomatic state off corticosteroids and dietary modification. Although more research is needed to evaluate this treatment modality more fully, we hope our case adds to the literature as an example of successful treatment of EGID with an interleukin-4 and -13 antagonist. The successful use of dupilumab contrasts with the discouraging results of eosinophil-targeted interleukin-5 agents and emphasizes the current, incomplete understanding of the underlying endotypic drivers of EGID.12-14 This case also demonstrates a need for further research into maintenance treatment of EGID to avoid the complications of prolonged steroid use, restrictive diet modification, or long-term complications of eosinophilic infiltration on the GI tract. Successful treatment of EGID as presented in this case will be invaluable to progress treatment and avoid the consequences of long-term steroid use and surgical options in a disease increasing in prevalence.4
DISCLOSURESAuthor contributions: J. Johnson, N. Harris, B. Sadowski, T. Banks, and A. Bush: contributing authors. C. Arnold is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Pesek RD, Reed CC, Muir AB, et al. Consortium of eosinophilic gastrointestinal disease researchers (CEGIR). Increasing rates of diagnosis, substantial co-occurrence, and variable treatment patterns of eosinophilic gastritis, gastroenteritis, and colitis based on 10-year data across a multicenter consortium. Am J Gastroenterol. 2019;114(6):984–94. 2. Zhang M, Li Y. Eosinophilic gastroenteritis: A state-of-the-art review. J Gastroenterol Hepatol. 2017;32(1):64–72. 3. Gonsalves N. Eosinophilic gastrointestinal disorders. Clin Rev Allergy Immunol. 2019;57(2):272–85. 4. Kim HP, Reed CC, Herfarth HH, Dellon ES. Vedolizumab treatment may reduce steroid burden and improve histology in patients with eosinophilic gastroenteritis. Clin Gastroenterol Hepatol. 2018;16(12):1992–4. 5. Kubo K, Kimura N, Mabe K, Matsuda S, Tsuda M, Kato M. Eosinophilic gastroenteritis-associated duodenal ulcer successfully treated with crushed budesonide. Intern Med. 2020;59(18):2249–54. 6. Dellon ES, Rothenberg ME, Collins MH, et al. Dupilumab in adults and adolescents with eosinophilic esophagitis. N Engl J Med. 2022;387(25):2317–30. 7. Gomes M, Mendes A, Ferreira F, Branco J, Tonin FS, Pedro ME. The role of benralizumab in eosinophilic immune dysfunctions: A case report-based literature review. Case Rep Med. 2023;2023:8832242. 8. Foroughi S, Foster B, Kim N, et al. Anti-IgE treatment of eosinophil-associated gastrointestinal disorders. J Allergy Clin Immunol. 2007;120(3):594–601. 9. Uppal V, Kreiger P, Kutsch E. Eosinophilic gastroenteritis and colitis: A comprehensive review. Clin Rev Allergy Immunol. 2016;50(2):175–88. 10. Harb H, Chatila TA. Mechanisms of dupilumab. Clin Exp Allergy. 2020;50(1):5–14. 11. AAP News: FDA Approves Dupixent for Eosinophilic Esophagitis; Expands Indication for Atopic Dermatitis. Media release, copyright 2022 American College of Pediatrics (https://www.fda.gov/media/161413/download) (2022). Accessed April 11, 2023. 12. Roufosse F. Targeting the interleukin-5 pathway for treatment of eosinophilic conditions other than asthma. Front Med (Lausanne). 2018;5:49. 13. D'Ippolito D, Pisano M. Dupilumab (dupixent): An interleukin-4 receptor antagonist for atopic dermatitis. P T. 2018;43(9):532–5. 14. Jensen ET, Martin CF, Kappelman MD, Dellon ES. Prevalence of eosinophilic gastritis, gastroenteritis, and colitis: Estimates from a national administrative database. J Pediatr Gastroenterol Nutr. 2016;62(1):36–42.
Comments (0)