
Remember me


Approximately 1% of colorectal cancers can be attributed to metastatic neoplasms originating from other primary sources. Primary sources of metastasis to the colon are typically the lung, ovary, breast, prostate, kidney, and skin. Most metastasis spreads to the colon through peritoneal seeding, although distant metastasis tends to spread through the lymphatic or hematogenous systems.1 Metastasis to the colon from the thyroid is exceedingly rare.
CASE REPORTA 76-year-old man with a history of papillary thyroid carcinoma (PTC) and known pulmonary metastasis presented to the hospital with melena. Hemoglobin on presentation was noted to be 8 from a baseline of 12–13. He had no history of gastrointestinal bleed and no previous endoscopic workup. Treatment of his PTC consisted of a total thyroidectomy, radioactive iodine, and external beam radiotherapy in 2012. He was started on dabrafenib in January 2023 because of increased lung metastases that had been stable on surveillance imaging for years.
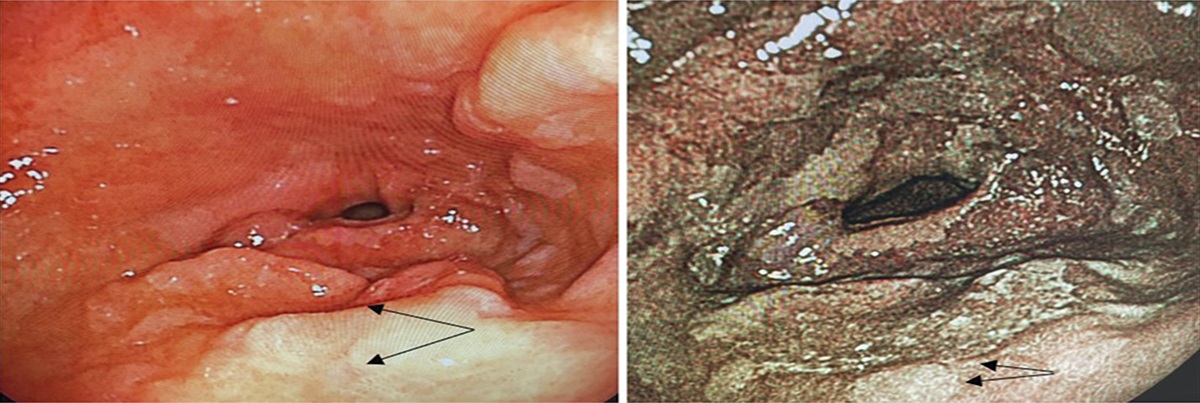
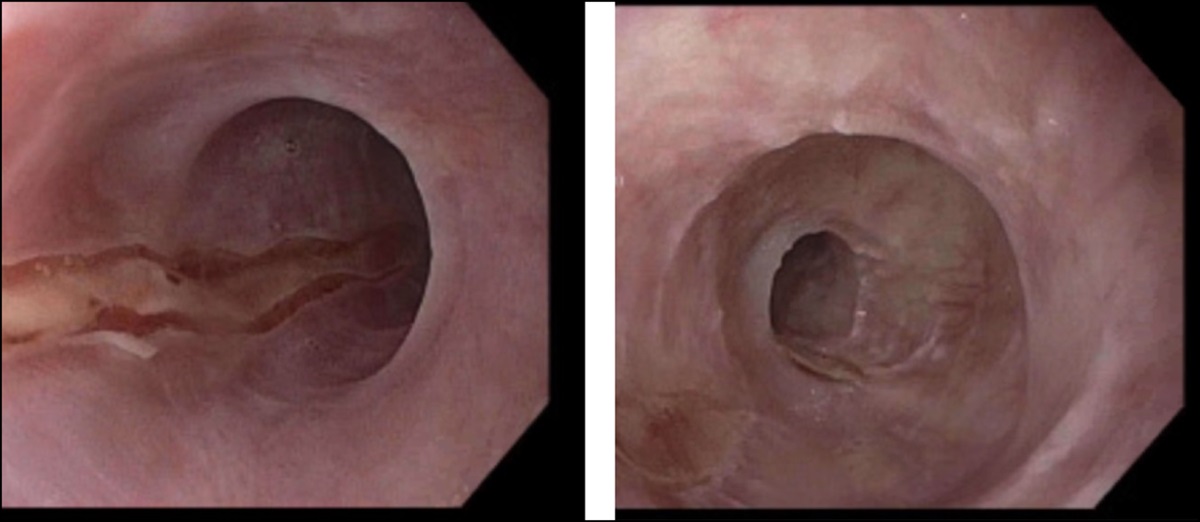
On admission, endoscopy demonstrated mild esophagitis, gastritis, and a healing ulcer in the gastric body. Colonoscopy showed 2 angioectasias in the cecum to which argon plasma coagulation and 2 hemostatic clips were applied. One 10-mm ulcerated polyp was found at 40 cm from the anal verge. Two side-by-side polyps were found at 20 cm from the anal verge. These polyps were the Paris classification Isp with an irregular pit and vascular pattern under narrow band imaging examination. The ulcerated polyp at 40 cm was resected by hot snare for representative biopsy. Pathology from the resected polyp was consistent with metastatic carcinoma compatible with metastasis from his PTC. Immunostains are diffusely positive for BRAF VE1 (Figure 1).
 Figure 1.:
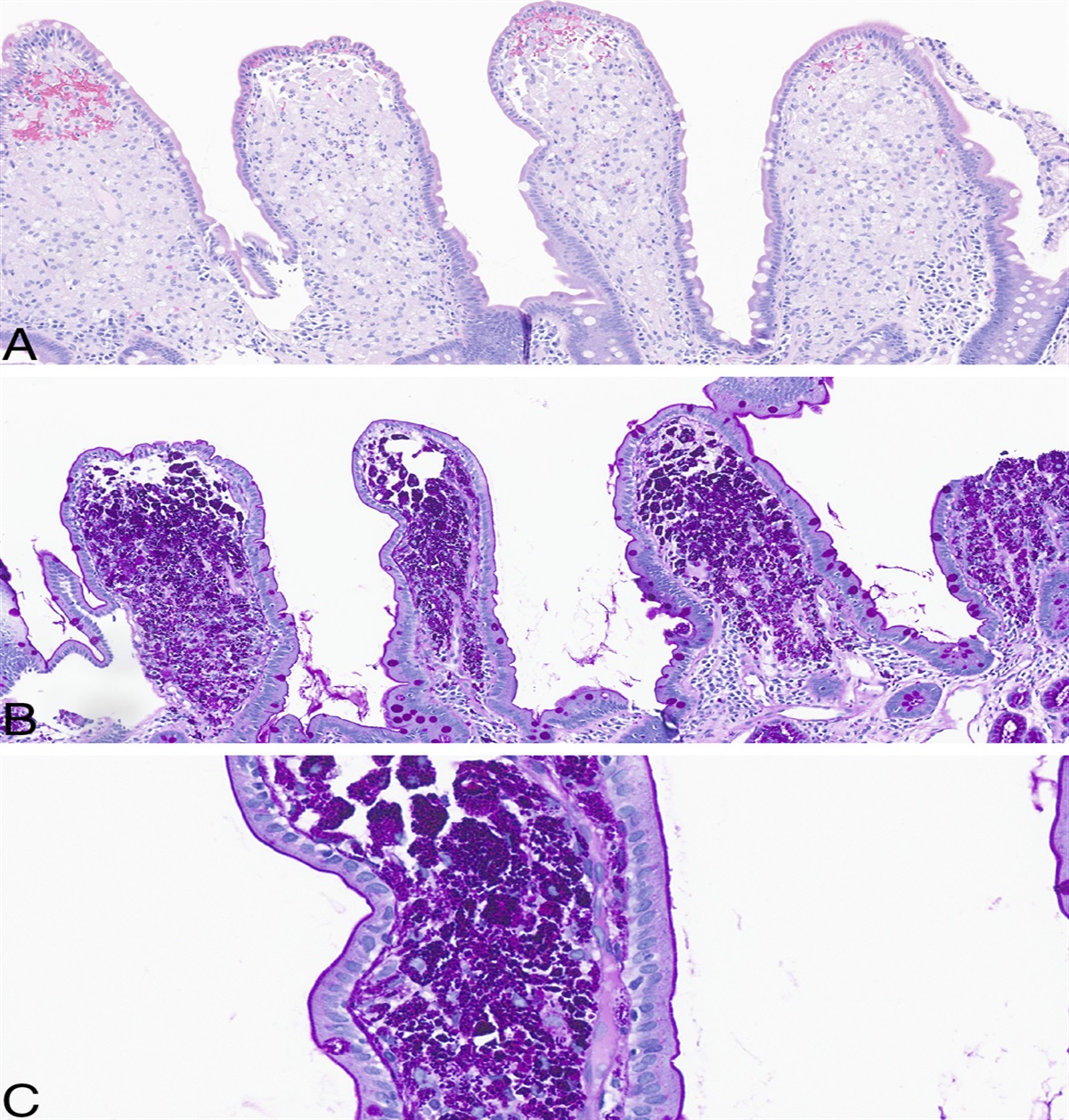
Figure 1.: (A) Two 10-mm polyps at 20 cm from the anal verge. (B) One ulcerated, 10-mm polyp at 40 cm from the anal verge. This was resected with hot snare for biopsy. (C) Low-power view of sigmoid colon polyp showing colonic crypts surrounded by the lamina propria that is replaced and expanded by malignant cells that are diffusely positive for BRAF VE1 (left). High-power view of markedly pleomorphic and atypical malignant cells in the lamina propria (right).
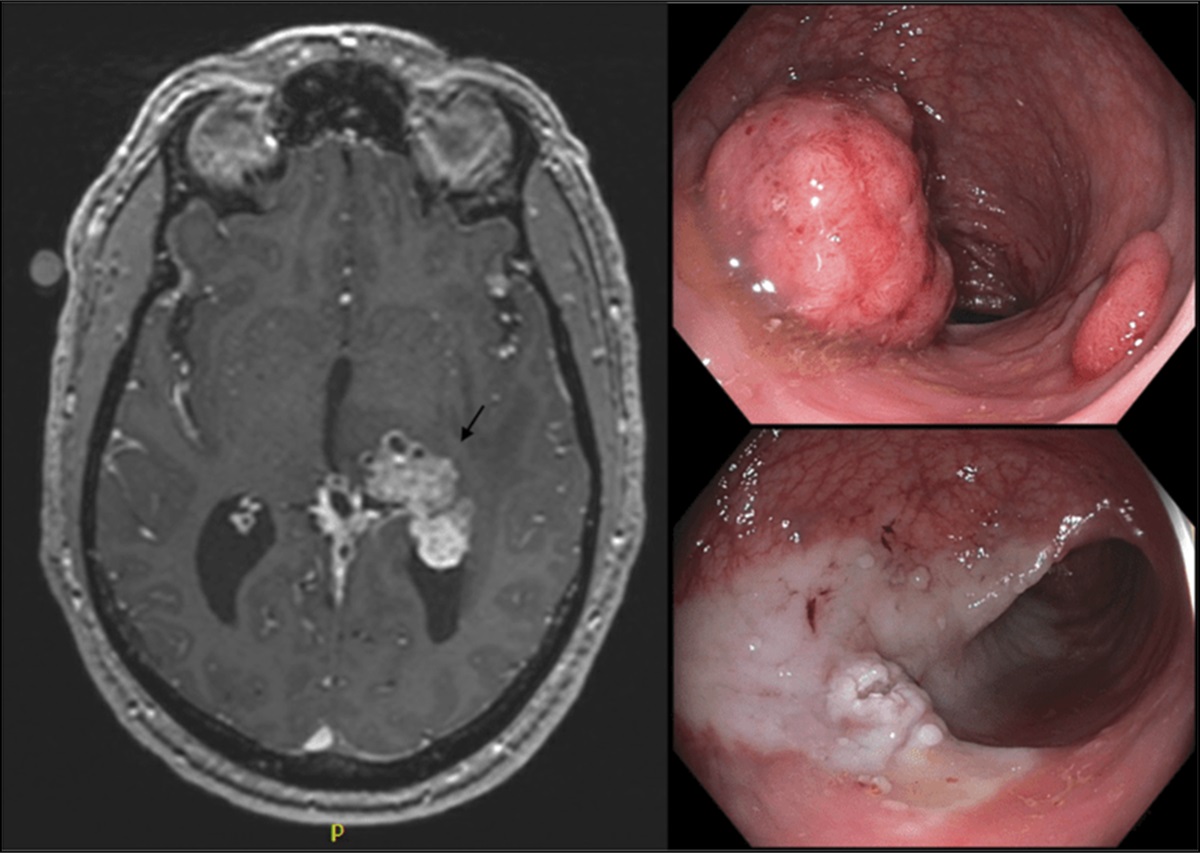
A computed tomography (CT) after colonoscopy demonstrated definitive heterogeneous tumor in the left lung base, diffuse lymphangitic spread of the tumor in the lower lungs, and bilateral malignant pleural effusions. Heterogeneity of the pancreatic body was noted as well. Brain CT showed greater than 20 metastases with confirmation by magnetic resonance imaging. Surveillance positron emission tomography CT 6 months before demonstrated known though stable lung metastases; however, these conventional CT studies in the patient confirmed further metastases. He was scheduled to start on palliative whole-brain radiation therapy; however, he died at home shortly after discharge from the hospital.
DISCUSSIONPTCs are the most common malignancy of the thyroid, affecting roughly 13.5 per 100,000 people. Follicular and papillary thyroid cancers are considered differentiated. The 10-year survival rate in patients with differentiated thyroid cancer is over 95% if the patient is younger than 40 years. Patients aged between 40 and 59 years have an 80% 10-year survival rate. However, once these differentiated carcinomas become metastatic the 10-year survival rate decreases to 10%. Roughly 2%–10% of patients with PTC have metastasis at the time of diagnosis. Areas of metastasis are most commonly pulmonary or skeletal and less frequently brain, kidney, liver, and adrenals. These tend to spread by lymphatic extension.2,3 Activating BRAF V600E or RET/PTC mutations are the most common pathways resulting in differentiated carcinoma. PTC is largely considered an indolent diagnosis and metastatic disease can usually be attributed to a more aggressive variant of PTC. These variants are diffuse sclerosing variant, tall cell variant (TCV), columnar cell variant, solid variant, and hobnail variant. These variants are notoriously resistance to RAI therapy and have higher rates of metastases and recurrence.
Diffuse sclerosing variant is largely attributed to high levels of radiation and will often present with cervical or pulmonary metastasis. Solid variant has also been linked to radiation exposure, although it is also more commonly seen in the pediatric population regardless of radiation history. Columnar cell variant of PTC is known for its rapid growth rate and association with early local invasion and high rate of recurrence. Hobnail variant is defined as the differentiated PTC with the most aggressive behavior and significant mortality. The classification of TCV is debated because tall cell areas (cells with at least a 3:1 height to width ratio) are present in conventional PTCs, although its diagnosis is usually given when 10%–30% of cells are the TCV. Some studies have demonstrated a linear relationship to tall cell percentage and presence of distant metastasis.4
There is also the recently recognized cribriform-morular variant (CMV) of PTC which has been linked with familial adenomatous polyposis (FAP). One study found that slightly over half of patients diagnosed with CMV-PTC had concurrent FAP. This relationship suggests that a diagnosis of this variant of PTC be followed by screening for FAP and colon cancer in both that patient and their family.5
Even among these more aggressive variants of PTC, however, metastasis to the colon, as seen in this patient, is rarely seen. Although the variants present with distant metastasis, only CMV-PTC has been documented in the literature to present in the colon.
The pathology from the resected colonic polyps in this patient was consistent with PTC of the tall cell variant. Roughly 4% of PTCs are the tall cell variant, seen in this patient. These are most commonly associated with activating BRAF mutations, also seen in this patient with a BRAF V600E mutation. Although the tall cell variant is notorious for distant metastasis, it is the first documented presentation of metastases to the colon.4
The findings in this report emphasize the importance of close follow-up in patients with a thyroid cancer diagnosis regardless of cell variant subtype. In particular, patients with metastasis at presentation of thyroid cancer should undergo regular colorectal cancer screening. Given the novelty of the findings discussed, the link between colorectal cancer and thyroid disease requires further investigation.
DISCLOSURESAuthor contributions: EB Lewine is the article guarantor. Feedback and editorial changes were made by Z. Patel, J. Forman, and A. Manvar who all presided over this patient's hospitalization. I. Hanna provided expertise as a pathologist.
Financial disclosure: None to report.
Previous presentation: This case was presented at the American College of Gastroenterology Annual Scientific Meeting; October 20-25, 2023; Vancouver, Canada.
Informed consent was obtained for this case report.
REFERENCES 1. Galanopoulos M, Gkeros F, Liatsos C, et al. Secondary metastatic lesions to colon and rectum. Ann Gastroenterol. 2018;31(3):282–7. 2. Powers AE, Marcadis AR, Lee M, Morris LGT, Marti JL. Changes in trends in thyroid cancer incidence in the United States, 1992 to 2016. JAMA. 2019;322(24):2440–1. 3. Portela RA, Choby GW, Manni A, Campbell D, Crist H, Goldenberg D. Unusual sites of metastasis of papillary thyroid cancer: Case series and review of the literature. Ear Nose Throat J. 2015;94(8):E43–7. 4. Coca-Pelaz A, Shah JP, Hernandez-Prera JC, et al. Papillary thyroid cancer-aggressive variants and impact on management: A narrative review. Adv Ther. 2020;37(7):3112–28. 5. Lam AK, Saremi N. Cribriform-morular variant of papillary thyroid carcinoma: A distinctive type of thyroid cancer. Endocr Relat Cancer. 2017;24(4):R109–21.
Comments (0)