
Remember me


Ectopic varices are dilatated portosystemic collateral veins found outside the gastroesophageal regions and are responsible for 5% of variceal bleeding.1 A rare subset of ectopic varices is colonic varices. Colonic varices can be secondary to a variety of etiologies, including acquired venous anomalies, portal hypertension, portal vein thrombosis, splenic vein thrombosis, mesenteric vein obstruction, and congestive heart failure. Colonic varices caused by portal hypertension have been well-described in both cirrhotic and noncirrhotic populations, and the most common site in these populations has been the rectum.2–4 Isolated right colonic varices in patients with pancreatic cancer are rare, and the prevalence rate is largely unknown because colonic varices are not well-described because of the paucity of published studies and underdiagnosis. We present a case of newly diagnosed pancreatic adenocarcinoma with findings of isolated right-sided colonic varices and a literature review of pancreatic cancer-related colonic varices.
CASE REPORTA 64-year-old man with recently diagnosed pancreatic cancer was transferred from an outside hospital for hematochezia. The patient reported abdominal pain for approximately 6 months before presentation associated with 30 pound weight loss. He was evaluated multiple times for this abdominal pain and had a computed tomography (CT) scan showing a pancreatic mass with occlusion of the portal vein. He underwent an esophagogastroduodenoscopy with endoscopic ultrasound, with fine-needle biopsy results consistent with pancreatic adenocarcinoma. Before being able to establish care with an oncologist, he presented to the hospital with hematochezia. He underwent esophagogastroduodenoscopy that showed diffuse gastropathy and duodenitis, but no ulcers or varices. A subsequent colonoscopy showed old blood throughout the colon and pandiverticulosis. Blood was noted upon intubation of the terminal ileum. It was unclear whether this was reflux from the cecum because there was no active bleeding site noted. He had colonoscopy that noted some polyps few years ago. His hemoglobin dropped from 13 to 6 mg/dL over the course of the hospitalization with ongoing episodes of hematochezia, requiring blood transfusion. He had a tagged red blood cell scan that was positive in the right lower quadrant, raising concern for bleeding in the distal ileum. He was transferred to our facility for consideration of deep balloon enteroscopy.
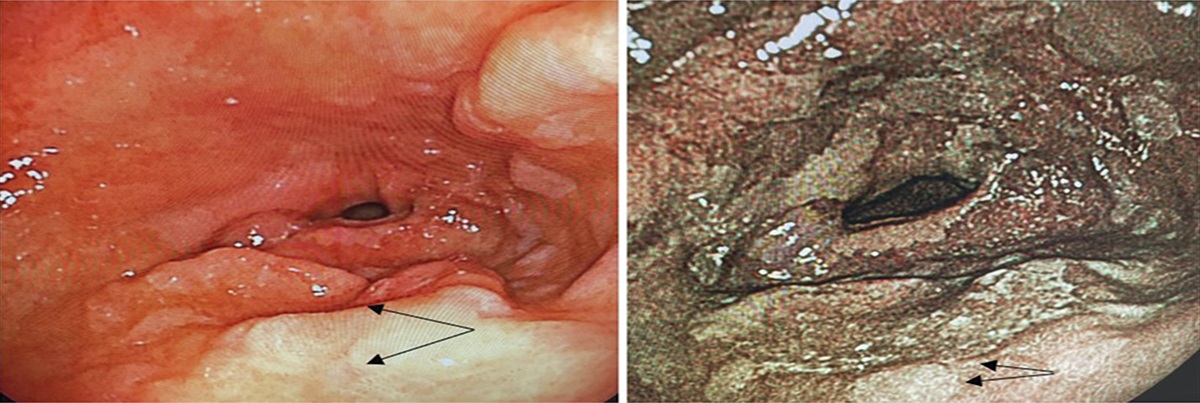
The patient underwent repeat colonoscopy for the evaluation of hematochezia, which revealed an isolated ascending colon and hepatic flexure varices (Figure 1). On further evaluation, no bleeding or abnormalities were noted in the distal ileum. On withdrawal of the colonoscope, he was noted to have oozing from the colonic varices. This was not felt to be amenable to endoscopic intervention because sclerotherapy was not immediately available. A CT angiogram was subsequently obtained for better characterization of the colonic varices. The scan showed that the pancreatic head/neck mass was encasing the celiac axis, superior mesenteric artery, and portal confluence with occlusion of the superior mesenteric vein resulting in extensive collateral vessels in the upper abdomen and submucosal venous collateral vessels involving the hepatic flexure/ascending colon (Figures 2 and 3). The bleeding eventually stopped with supportive care alone. The case was discussed in a multidisciplinary conference with interventional radiology and surgical oncology regarding potential treatment options given the ongoing risk of recurrent bleeding. Unfortunately, given the extensive involvement of the vasculature by the pancreatic mass, no viable interventions were identified. The patient elected to pursue hospice care after discussing goals of care with a palliative team.
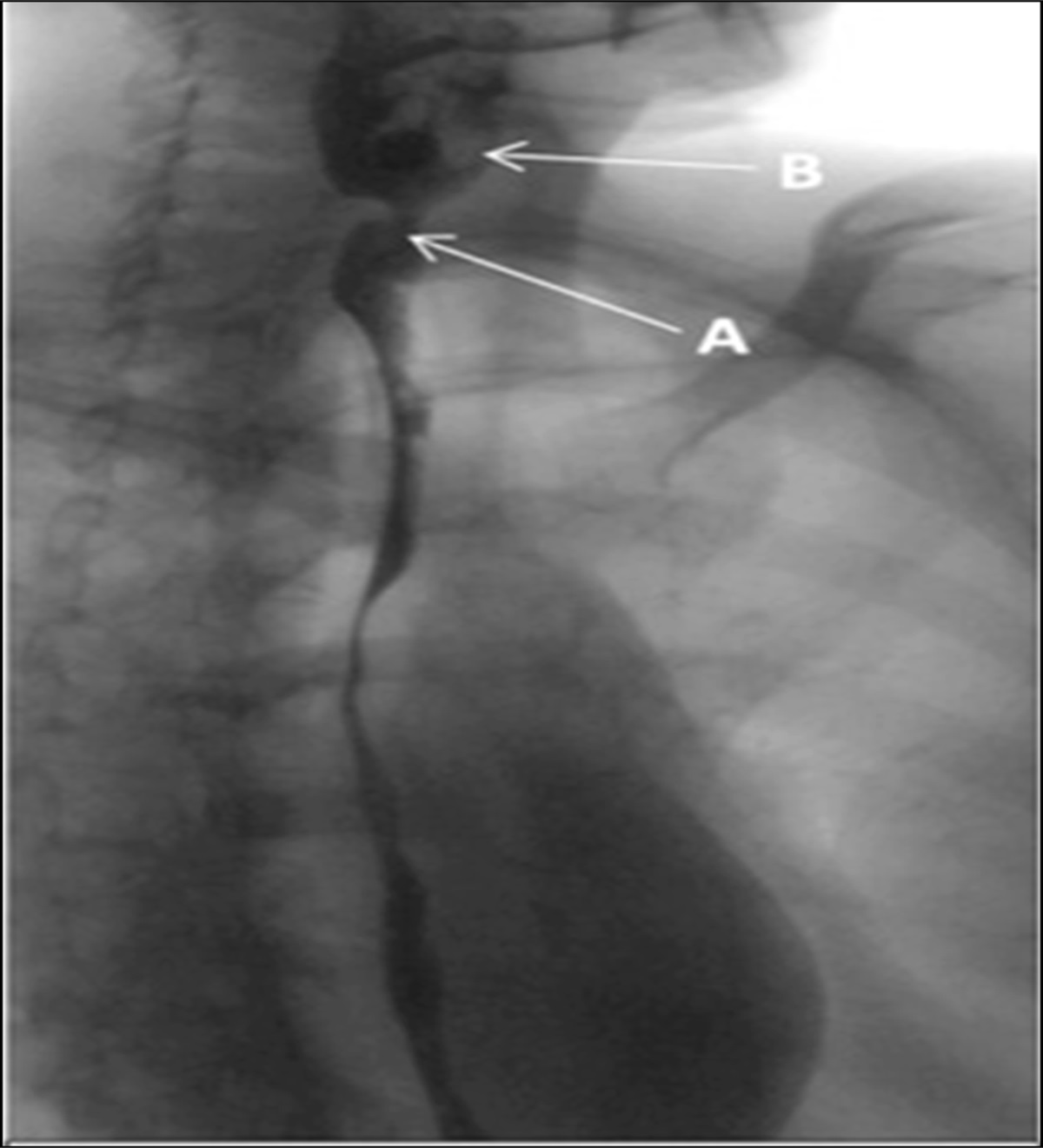
 Figure 1.:
Figure 1.: Isolated ascending colon varices (yellow arrow pointing to the varices).
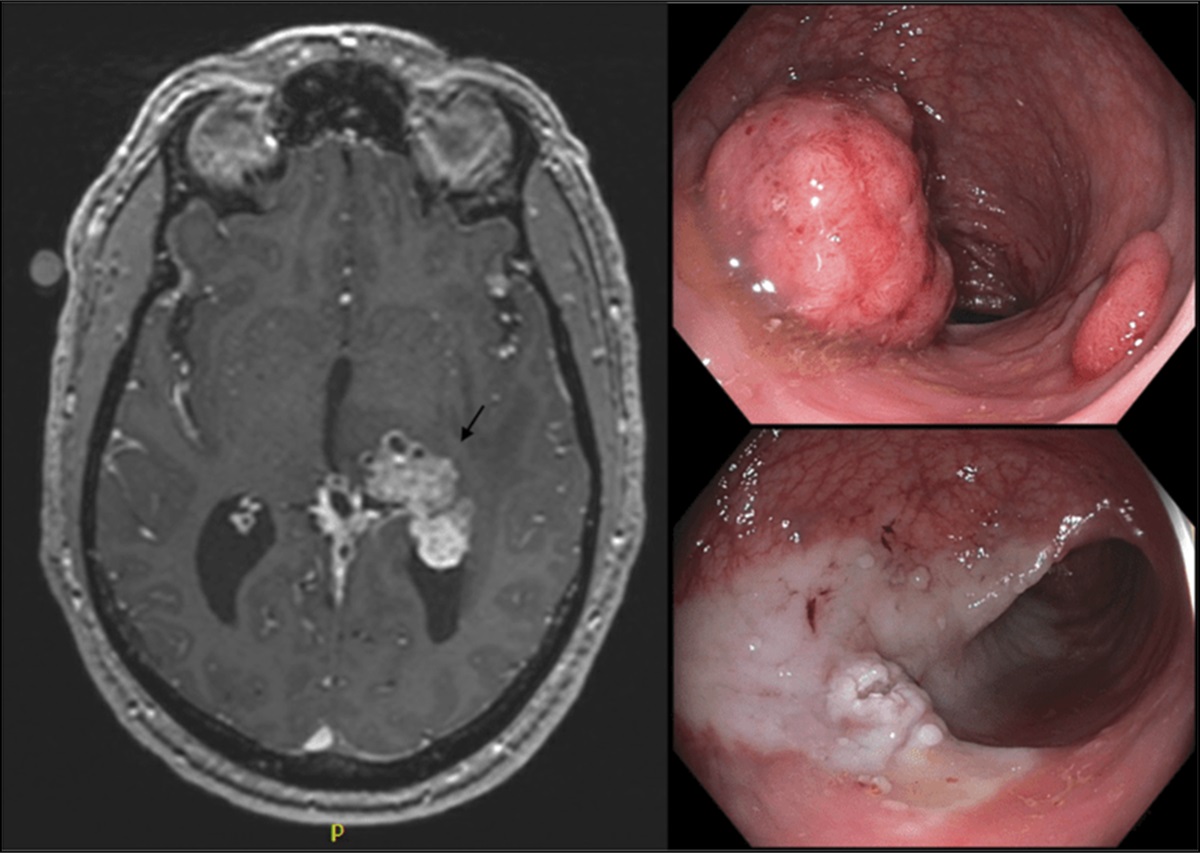
 Figure 2.:
Figure 2.: Pancreatic head/neck mass (axial view). Arrows point to pancreatic head mass.
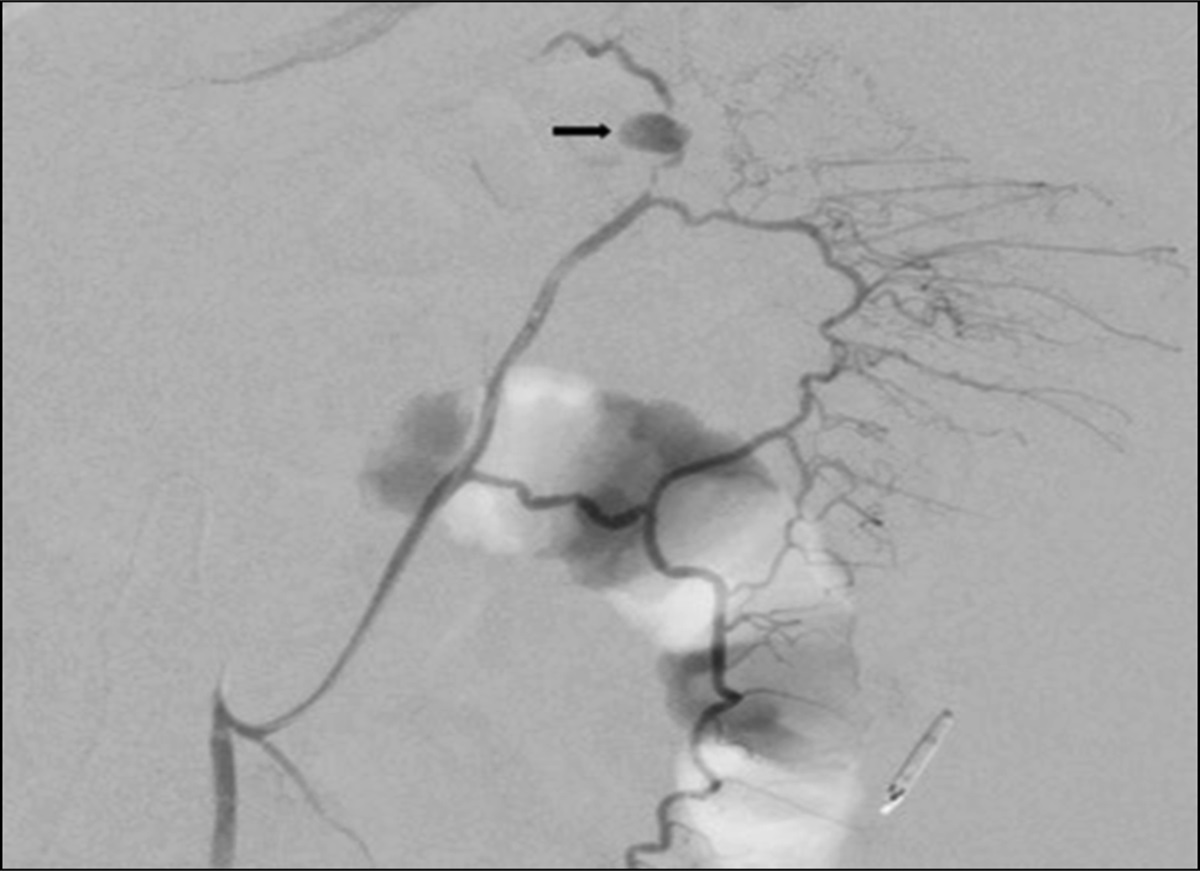
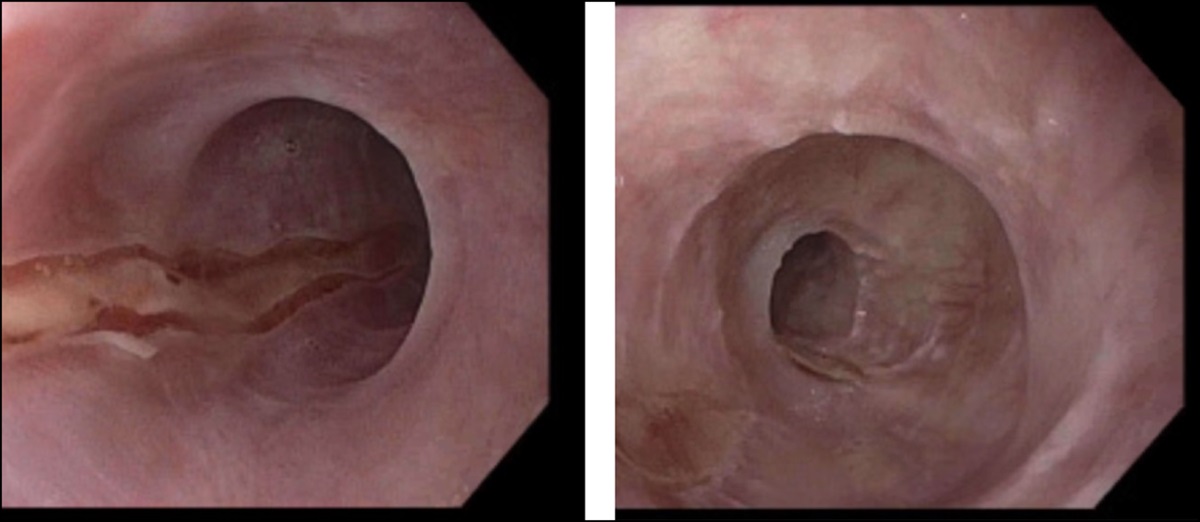
 Figure 3.:
Figure 3.: Dilated venous vessels involving the right colon distal to the superior mesenteric vein (axial view). Arrows point to colonic varcies.
DISCUSSION PathophysiologyThe literature review of case reports of isolated colonic varices related to pancreatic cancer are summarized in Table 1. Colonic varices secondary to pancreatic cancer are rarely described in the literature. In the case of our patient, there was involvement of the superior mesenteric vein resulting in left-sided portal hypertension (LSPH). LSPH as an entity is a rare type of portal hypertension often secondary to occlusion or thrombosis of the superior mesenteric vein or splenic vein.5 Although pancreatic cancer can also cause splenic vein thrombosis, in the few cases described in the literature and in our patient, the mass encased the superior mesenteric vein resulting in LSPH. Despite the differences in the involvement of the vasculature, they similarly developed isolated right-sided colonic varices.
Table 1. - Baseline characteristics and demographic information of case reports of colonic varices in pancreatic cancer Author Year Age Sex Presentation Etiology Location Feeder Treatment Cirrhosis Murakami et al 2020 55 M Hematochezia Pancreatic CA stage III with invasion of SMV AC Branch of the ileocolonic vein Laparoscopic ligation NoAC, ascending colon; CA, cancer; HF, hepatic flexure; IMV, inferior mesenteric vein; SMV, superior mesenteric vein; TC, transverse colon.
Often when varices are found in any location, the predominant concern is for cirrhosis and portal hypertension. However, it is important to note that colonic varices can also be seen with other diseases that cause portal vein occlusion, such as pancreatic cancer.6–9 The gold standard for diagnosis is CT or selective mesenteric angiography, which can also be therapeutic with embolization in some cases. Often, these varices are diagnosed during colonoscopy for evaluation of lower gastrointestinal bleeding. Unfortunately, they can be missed if they flatten with insufflation or if visualization of colonic mucosa is precluded by active bleeding, as was the case in our patient's initial colonoscopy.
TreatmentColonic varices are rare, and there is a lack of established guidelines on management. Most of the recommended treatment options are reported in case reports or case series (Table 1). If colonic varices are not bleeding, they are managed with supportive care.6 Laxative use to soften stool and iron supplementation can help varices that are slowly bleeding.10 Active variceal bleeding can be controlled endoscopically with sclerotherapy, injections of cyanoacrylate, venous obliteration, and band ligation.9 However, banding would not be a feasible option for right-sided colonic varices because the banding kit would not be able to attach to the colonoscope, making these varices even more challenging. If the varices bleed significantly, endovascular embolization, in addition to laparoscopic ligation or colectomy, may be required. Transjugular intrahepatic portosystemic shunt placement considered in patients with liver cirrhosis for portal decompression along with CT angiography of the bowel with embolization to control bleeding may be beneficial.11
Isolated colonic varices are rare complications of pancreatic cancer that can result in life-threating gastrointestinal bleeding. Management remains controversial and can be challenging in patients with significant bleeding. A multidisciplinary approach for treatment of such cases is recommended and should be guided by local expertise.
DISCLOSURESAuthor contributions: All authors contributed equally to the creation of this article.
Financial disclosure: None to report.
Informed patient consent was obtained for case report.
REFERENCES 1. Kinkhabwala M, Mousavi A, Iyer S, Adamsons R. Bleeding ileal varicosity demonstrated by transhepatic portography. AJR Am J Roentgenol 1977;129(3):514–6. 2. Rabinovitz M, Schade RR, Dindzans VJ, Belle SH, Van Thiel DH, Gavaler JS. Colonic disease in cirrhosis. An endoscopic evaluation in 412 patients. Gastroenterology 1990;99(1):195–9. 3. Ganguly S, Sarin SK, Bhatia V, Lahoti D. The prevalence and spectrum of colonic lesions in patients with cirrhotic and noncirrhotic portal hypertension. Hepatology 1995;21(5):1226–31. 4. Bresci G, Gambardella L, Parisi G, et al. Colonic disease in cirrhotic patients with portal hypertension: An endoscopic and clinical evaluation. J Clin Gastroenterol 1998;26(3):222–7. 5. Tzeng YD, Liu SI, Tsai CC. An unusual cause of haematemesis: Left-sided portal hypertension due to a large pancreatic tumour. Dig Liver Dis 2012;44(6):e12. 6. Ho YP, Lin CJ, Su MY, Tseng JH, Chiu CT, Chen PC. Isolated varices over hepatic flexure colon indicating superior mesenteric venous thrombosis caused by uncinate pancreatic head cancer--a case report. World J Gastroenterol 2005;11(12):1886–9. 7. Pinto-Pais T, Fernandes SS, Proença L, et al. Variceal hemorrhage of the colon secondary to pancreatic cancer. Endoscopy 2014;46(Suppl 1 UCTN):E500–1. 8. Kuwabara S, Matsumoto J, Tojima H, et al. Colonic varices treated with embolization after pancreatoduodenectomy with portal vein resection: A case report. Surg Case Rep 2020;6(1):126. 9. Murakami M, Fujimori N, Nagao Y, et al. Colonic varices: A rare complication of pancreatic cancer. Clin J Gastroenterol 2020;13(6):1355–9. 10. FELDMAN M Sr, Smith VM, Warner CG. Varices of the colon. Report of three cases. JAMA 1962;179:729–30. 11. Izsak EM, Finlay JM. Colonic varices. Three case reports and review of the literature. Am J Gastroenterol 1980;73(2):131–6.
Comments (0)