
Remember me


It is estimated that acute esophageal necrosis (AEN), also known as black esophagus, has an incidence between 0.01% and 0.2%, according to single-center studies. When esophagogastroduodenoscopy (EGD) is performed, the distal esophagus exhibits a black mucosa with a sharp transition to the gastroesophageal junction.
Endoscopic findings may also include ulcerations in the esophagus and/or duodenum, as well as obstruction of the gastric outlet. The most common manifestation of AEN is an upper gastrointestinal bleed (UGIB). It is believed that AEN results from chronic hypoperfusion and loss of protection of the esophageal mucosa, after an acute event or “trigger.” In addition to hematemesis and melena, other clinical features include abdominal pain, fever, nausea, vomiting, dysphagia, and syncope.1,2 Hemodynamic instability and cachexia are commonly observed physical findings. Treatment involves management of the underlying conditions, aggressive intravenous proton pump inhibitor therapy, rehydration, nutrition, and bowel rest.2,3 This case report discusses an unusual case of an individual with AEN, without any evident signs of UGIB.
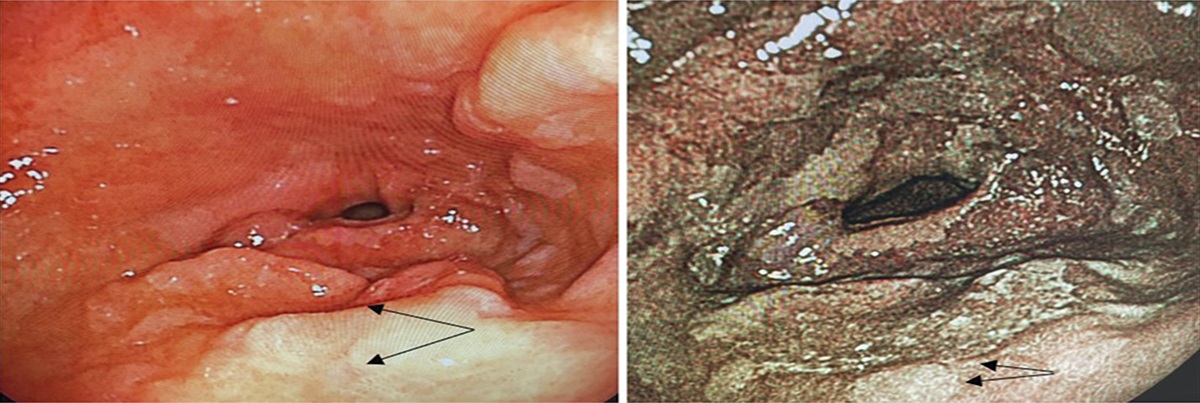
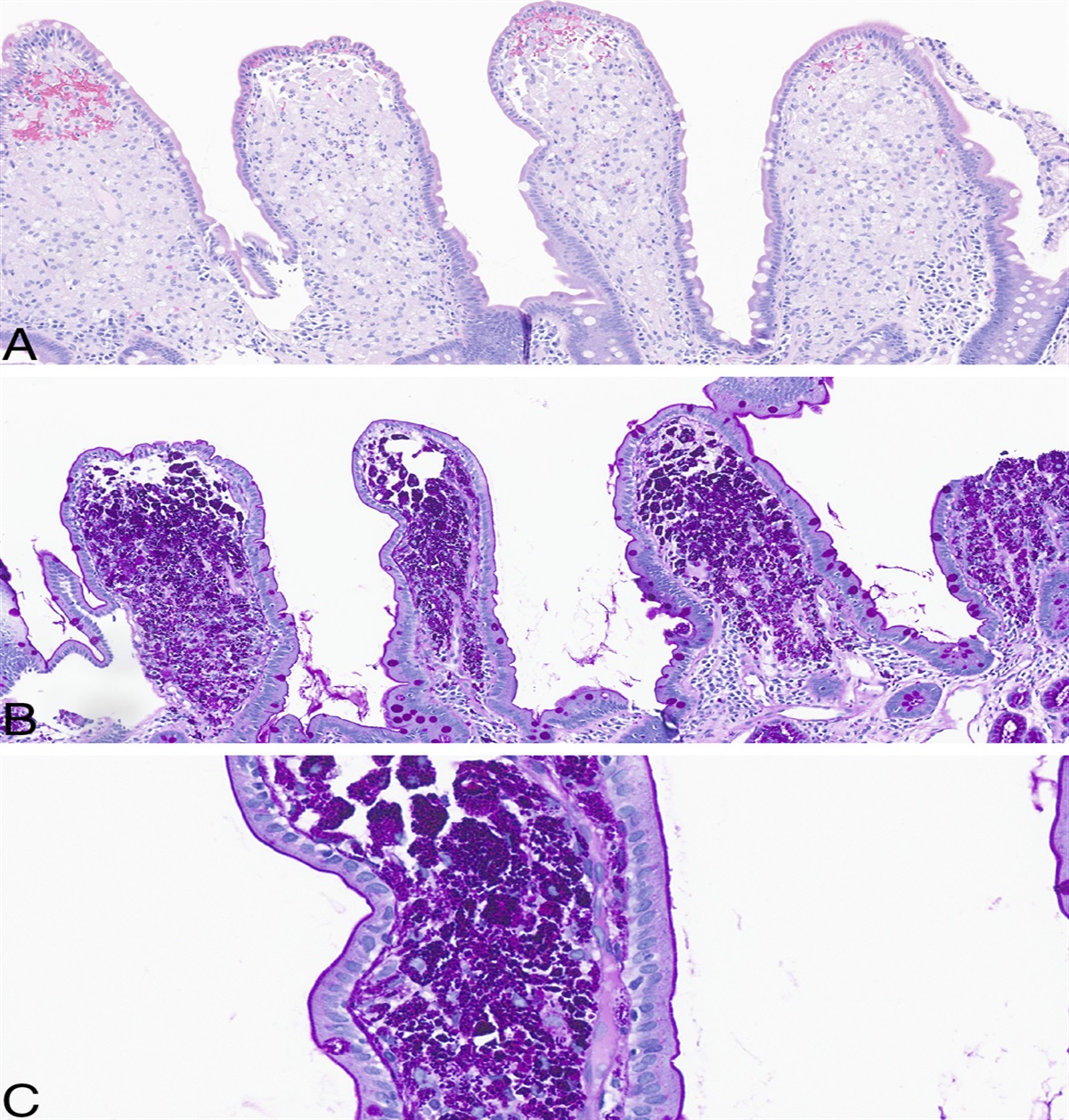
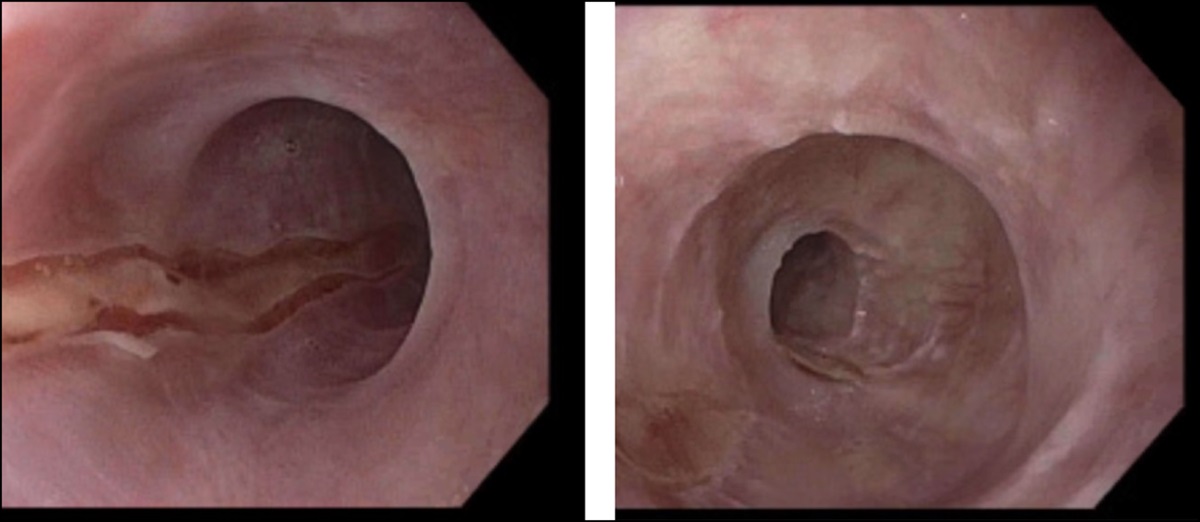
CASE REPORTA 67-year-old man with chronic obstructive pulmonary disease, peripheral vascular disease, and hypertension presented for escalation of care because of acute respiratory failure and triple vessel coronary artery disease. After 7 days of mechanical ventilation, the patient developed oropharyngeal dysphagia and failed a swallow evaluation. A Dobhoff tube was attempted enterally without success, prompting the need for gastroenterology consultation for endoscopic placement. The patient was tachycardic, normotensive, afebrile, and saturating well on 4 L nasal of cannula oxygen. Laboratory data revealed a hemoglobin level of 12 g/dL, a blood urea nitrogen level of 12 mg/dL, and a creatinine level of 0.64 mg/dL. The patient denied experiencing abdominal pain, vomiting, melena, or hematochezia. The endoscopy revealed normal mucosa in the upper third of the esophagus and a black mucosa in the middle-lower third of the esophagus (Figure 1). The biopsy revealed ulcer exudate and granulation tissue with acute inflammation and no evidence of cytomegalovirus, herpes simplex virus, or fungal organisms (Figure 2). Parenteral nutrition was initiated for the patient while he was placed on strict bowel rest. Four days later, the patient unfortunately expired of a ventricular arrhythmia.
 Figure 1.:
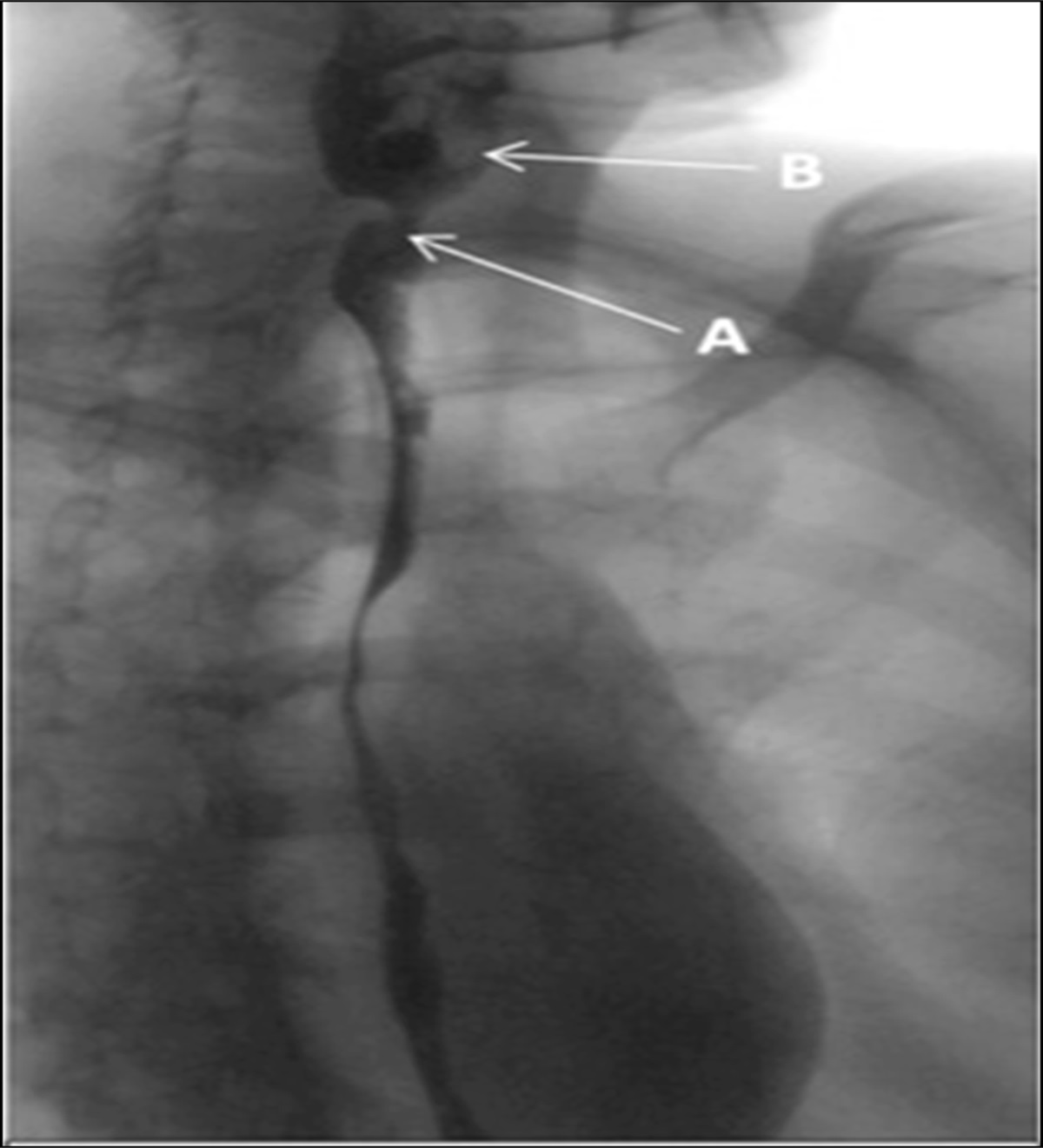
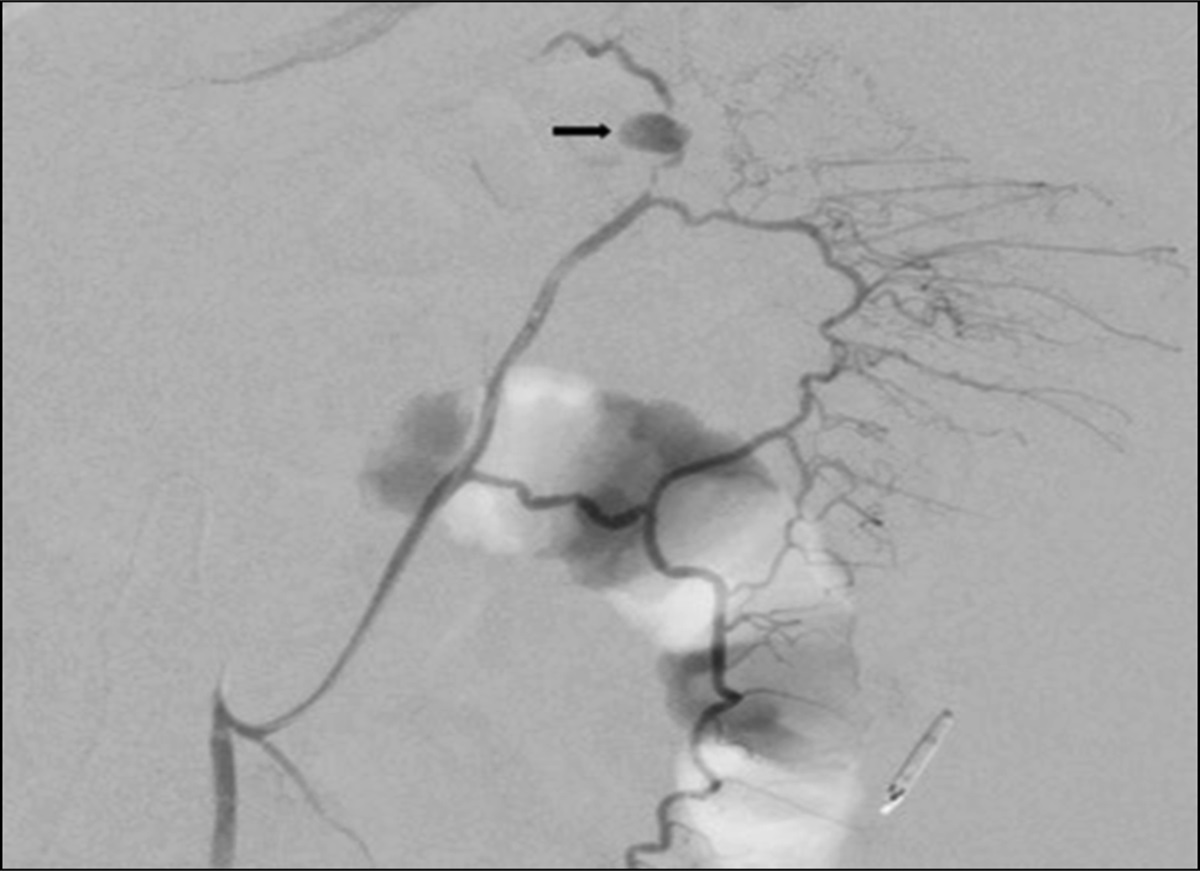
Figure 1.: Endoscopic findings. All images represent different sections of the distal third of the esophagus. Image (A), (C), and (D) demonstrate a diffuse, circumferential blackening of the mucosa. Image (B) demonstrates black mucosa with pink gastric mucosa distally, consistent with findings of an abrupt transition at the gastroesophageal junction commonly described in acute esophageal necrosis.
 Figure 2.:
Figure 2.: Biopsy of distal esophagus. This histology slide demonstrates findings of granulation tissue, as well as ulcer exudate and acute inflammation.
DISCUSSIONAEN was first described by Goldenberg et al in 1990.4 According to retrospective and prospective studies, it mostly affects males with a mean age of 67 years at the time of diagnosis.5–7 An analysis of EGDs in patients with UGIB, over a period of 3 years, revealed a prevalence of 6% of AEN, suggesting the likelihood that its incidence might have been underestimated.8 In such cases, emergent endoscopy is typically delayed because of hemodynamic instability. Consequently, AEN may remain undetected because some patients may have achieved mucosal healing before endoscopic evaluation.
AEN is believed to occur as a result of what is known as the “2-hit hypothesis.” This hypothesis suggests that chronic comorbidities increase susceptibility to esophageal hypoperfusion, loss of the protective mucosal barrier, and increased reflux of gastric secretions, which leads to injury of the esophageal mucosa. There is then a trigger event, such as hemodynamic instability, resulting in further hypoperfusion of the esophagus, as well as an increase in gastric secretions, further damaging the mucosa.2,9 The main risk factors for AEN are listed in Table 1.
Table 1. - Etiology of acute esophageal necrosis Risk factors Male sex Coronary heart disease Diabetes mellitus Peripheral artery disease Hypertension Congestive heart failure Dyslipidemia Chronic kidney disease Alcohol abuse Liver cirrhosis Gastroesophageal reflux disease Immunosuppression Triggers Hemodynamic compromise Infectious esophagitis Sepsis Chemotherapy Cardiac arrest Percutaneous coronary intervention Hypovolemia Pneumonia Trauma Gastric volvulus Diabetic ketoacidosis Achalasia Surgery Hepatitis (alcoholic, drug induced, etc.)A “2-hit” hypothesis has been described as the culprit for acute esophageal necrosis in which chronic comorbidities (risk factors), in association with an acute event (triggers) lead to the disease.
AEN is characterized by a diffuse black discoloration of the distal esophagus, which transitions abruptly at the gastroesophageal junction. At least 66% of cases present with hematemesis and generally manifest as UGIB requiring emergency hospitalization.1–3 Other signs and symptoms include melena (33%), acute abdominal pain (28%), and dysphagia (12%).10 There are cases of AEN presenting exclusively with dysphagia.11 Asymptomatic AEN, although rare, has been reported previously.12 Physical findings include cachexia, hypotension, tachycardia, and pallor. Laboratory findings are nonspecific: anemia from blood loss, leukocytosis from esophageal inflammation, and lactic acidosis from tissue ischemia.2 Diagnosis is made by visualizing AEN findings through EGD. Endoscopic findings include bleeding, blood clots, ulcers in the esophagus, duodenum, or gastric outlet, or obstruction of the gastric outlet. The diagnosis is not dependent on a biopsy, although it can be helpful in excluding other diagnoses, such as malignant melanoma, esophageal melanosis, acanthosis nigricans, or esophageal infection.3
AEN has a poor prognosis, with a mortality rate up to 32%.2 Early diagnosis with EGD prevents the devastating consequences of this disease. Considering this pathology's wide range of presentations, maintaining a high index of suspicion is essential.
Despite clear histological evidence of tissue necrosis, the absence of any hematemesis, melena, or evidence of blood loss anemia in the past, oropharyngeal dysphagia was the only presenting symptom of AEN in this case. In the setting of critical illness, deconditioning, and recent extubation, it would be reasonable to consider this patient's dysphagia multifactorial. However, dysphagia is present in many cases of AEN, and can even be the sole symptom, as evidenced in database studies previously.10 Hopefully, this case illustrates the importance of assessing acute dysphagia before enteral tube placement and maintaining a broad differential diagnosis in critically ill patients, especially those who have multiple vascular risk factors and tenuous hemodynamics.
DISCLOSURESAuthor contributions: PE Ziegler is responsible for overall composition, edits, and submission and is the article guarantor. DR Lora performed literature review, composition, as well as table and figure creation. M. DeMeo was main attending under case who oversaw the editorial process and suggested changes as appropriate and was also primary endoscopist in this case.
Financial disclosure: None to report.
Informed consent could not be obtained for this case report.
REFERENCES 1. Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG. Acute esophageal necrosis: A rare syndrome. J Gastroenterol. 2007;42(1):29–38. 2. Gurvits GE. Black esophagus: Acute esophageal necrosis syndrome. World J Gastroenterol. 2010;16(26):3219–25. 3. Dias E, Santos-Antunes J, Macedo G. Diagnosis and management of acute esophageal necrosis. Ann Gastroenterol. 2019;32(6):529–40. 4. Goldenberg SP, Wain SL, Marignani P. Acute necrotizing esophagitis. Gastroenterology. 1990;98(2):493–6. 5. Augusto F, Fernandes V, Cremers MI, et al. Acute necrotizing esophagitis: A large retrospective case series. Endoscopy. 2004;36(5):411–5. 6. Ramos R, Mascarenhas J, Duarte P, Vicente C, Casteleiro C. Acute esophageal necrosis: A retrospective case series [in Spanish]. Rev Esp Enferm Dig. 2008;100(9):583–5. 7. Ben Soussan E, Savoye G, Hochain P, et al. Acute esophageal necrosis: A 1-year prospective study. Gastrointest Endosc. 2002;56(2):213–7. 8. Yasuda H, Yamada M, Endo Y, Inoue K, Yoshiba M. Acute necrotizing esophagitis: Role of nonsteroidal anti-inflammatory drugs. J Gastroenterol. 2006;41(3):193–7. 9. Khan H, Ahmed M, Daoud M, Philipose J, Ahmed S, Deeb L. Acute esophageal necrosis: A view in the dark. Case Rep Gastroenterol. 2019;13(1):25–31. 10. Abdullah HM, Ullah W, Abdallah M, Khan U, Hurairah A, Atiq M. Clinical presentations, management, and outcomes of acute esophageal necrosis: A systemic review. Expert Rev Gastroenterol Hepatol. 2019;13(5):507–14. 11. Rejchrt S, Douda T, Kopácová M, et al. Acute esophageal necrosis (black esophagus): Endoscopic and histopathologic appearance. Endoscopy. 2004;36(12):1133. 12. Gurvits GE, Cherian K, Shami MN, et al. Black esophagus: New insights and multicenter international experience in 2014. Dig Dis Sci. 2015;60(2):444–53.
Comments (0)