
Remember me


Gastric point-of-care ultrasound has become an increasingly popular method for gastric assessment and risk stratification of pulmonary aspiration.1 Qualitative gastric point-of-care ultrasound relies on pattern recognition, with 50 supervised scans required for competency.2 We present a 75-year-old with hypertension who presented for uncontrolled epistaxis which was the likely cause of her gastric thrombus. She had nothing by mouth for over 24 hours with no delayed gastric emptying comorbidities.
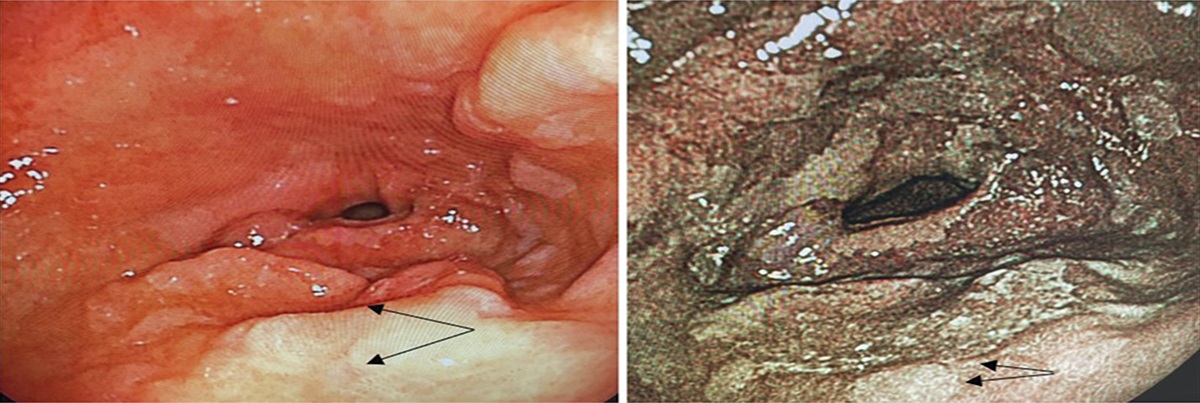
The images below highlight the similarities and differences between gastric contents and a gastric thrombus. The images are almost indistinguishable, with only minor distinctions. The left image is from the patient with epistaxis and represents a thrombus in her antrum. The image on the right is from a healthy patient who had eaten a full meal 5 hours earlier. As seen in Figure 1, one might notice that the thrombus has a more irregular echogenicity with a honeycomb appearance that does not extend to the hypoechoic, muscularis propria. Finally, the ultrasonographic pattern of thrombi has been described as having an appearance similar to hepatic tissue, which is evident in the left image.3
 Figure 1.:
Figure 1.: Gastric thrombus vs a full stomach on gastric ultrasonography. Left image demonstrates the gastric thrombus while the right image demonstrates the classic full stomach appearance.
To our knowledge, this is the first description of gastric thrombus and its similar appearance to gastric contents.
DISCLOSURESAuthor contributions: E. Heinz, R. Pla, and P. Patel were responsible for the conceptualization and image acquisition. E. Heinz, J. Davis, and P. Patel were responsible for drafting the article. E. Heinz, P. Patel, R. Pla, and J. Davis all shared editing and reviewing responsibilities. E. Heinz is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Perlas A, Arzola C, Van de Putte P. Point-of-care gastric ultrasound and aspiration risk assessment: A narrative review. Can J Anaesth. 2018;65(4):437–48. 2. Kruisselbrink R, Gharapetian A, Chaparro LE, et al. Diagnostic accuracy of point-of-care gastric ultrasound. Anesth Analg. 2019;128(1):89–95. 3. Jasudavisius A, Arellano R, Martin J, McConnell B, Bainbridge D. A systematic review of transthoracic and transesophageal echocardiography in non-cardiac surgery: Implications for point-of-care ultrasound education in the operating room. Can J Anaesth. 2016;63(4):480–7.
Comments (0)