
Remember me


Cancer of the appendix is an uncommon malignancy that is rarely diagnosed on colonoscopy. We present a case of incidentally discovered goblet cell adenocarcinoma (GCA) of the appendix and the subsequent management of the malignancy.
CASE REPORTAn 81-year-old man with a medical history of coronary artery disease, atrial fibrillation, and diverticulosis presented to a gastroenterology clinic for persistent epigastric pain and acid reflux. Symptoms had been worsening for several years and were refractory to medical therapy. He denied unintentional weight loss, nausea, dysphagia, or melena. He reported a family history of gastric cancer (grandmother) but denied family history of colorectal cancer. Additional history included 9 colonoscopies between 1999 and 2016 for rectal bleeding, determined to be secondary to hemorrhoids and diverticulosis. He also had a history of tubular adenomas removed, last of which being found in 2016 for which he was now due for follow-up screening. Bidirectional endoscopy was deemed appropriate and performed. During the colonoscopy, the appendiceal orifice was noted to have a “heaped-up” appearance and was biopsied with cold forceps (Figure 1). The pathology report noted clusters of cells with goblet cell morphology that had infiltrated the normal colonic glands (Figures 2 and 3). Immunohistochemistry (IHC) staining was performed and demonstrated cells positive for cytokeratin AE1/AE3, weakly positive for chromogranin, and negative for synaptophysin (Figures 4 and 5). The combination of these findings were consistent with GCA. Computed tomography imaging of the chest, abdomen, and pelvis was obtained, showing a mildly enlarged appendix, no lymphadenopathy, and no evidence of metastasis (Figure 6). The patient underwent a laparoscopic right hemicolectomy 2 months later. Pathologic evaluation showed that carcinoma extended from the appendix to the mesoappendix and cecum with extensive lymphovascular and perineural invasion. The resection margins and 19 resected lymph nodes were negative for malignancy. Staging after surgery was T4aN0M0 (IIB). The patient recovered from surgery uneventfully. Follow-up colonoscopy 1 year later revealed a healthy ileocolonic anastomosis and postsurgical changes with no signs of polyps or other masses. Surveillance computed tomography imaging showed no active disease.
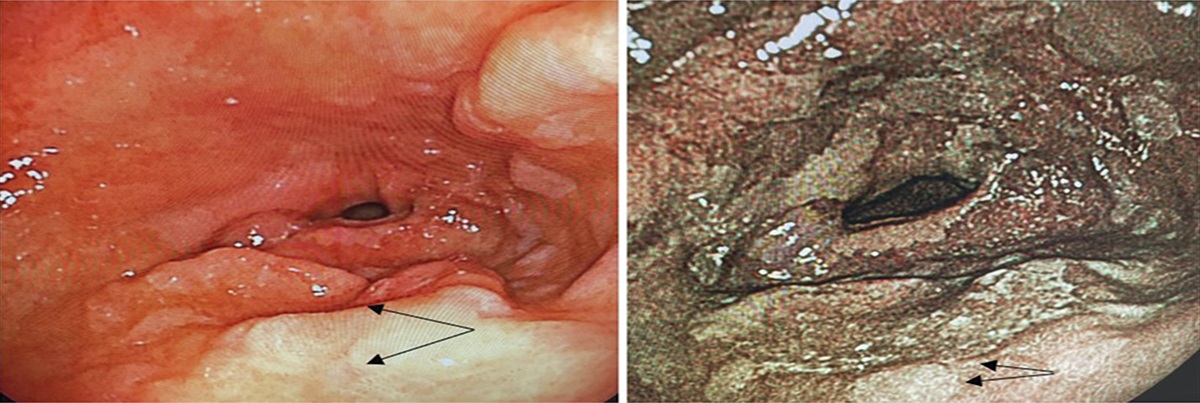
 Figure 1.:
Figure 1.: Appendiceal orifice with “heaped-up” appearance.
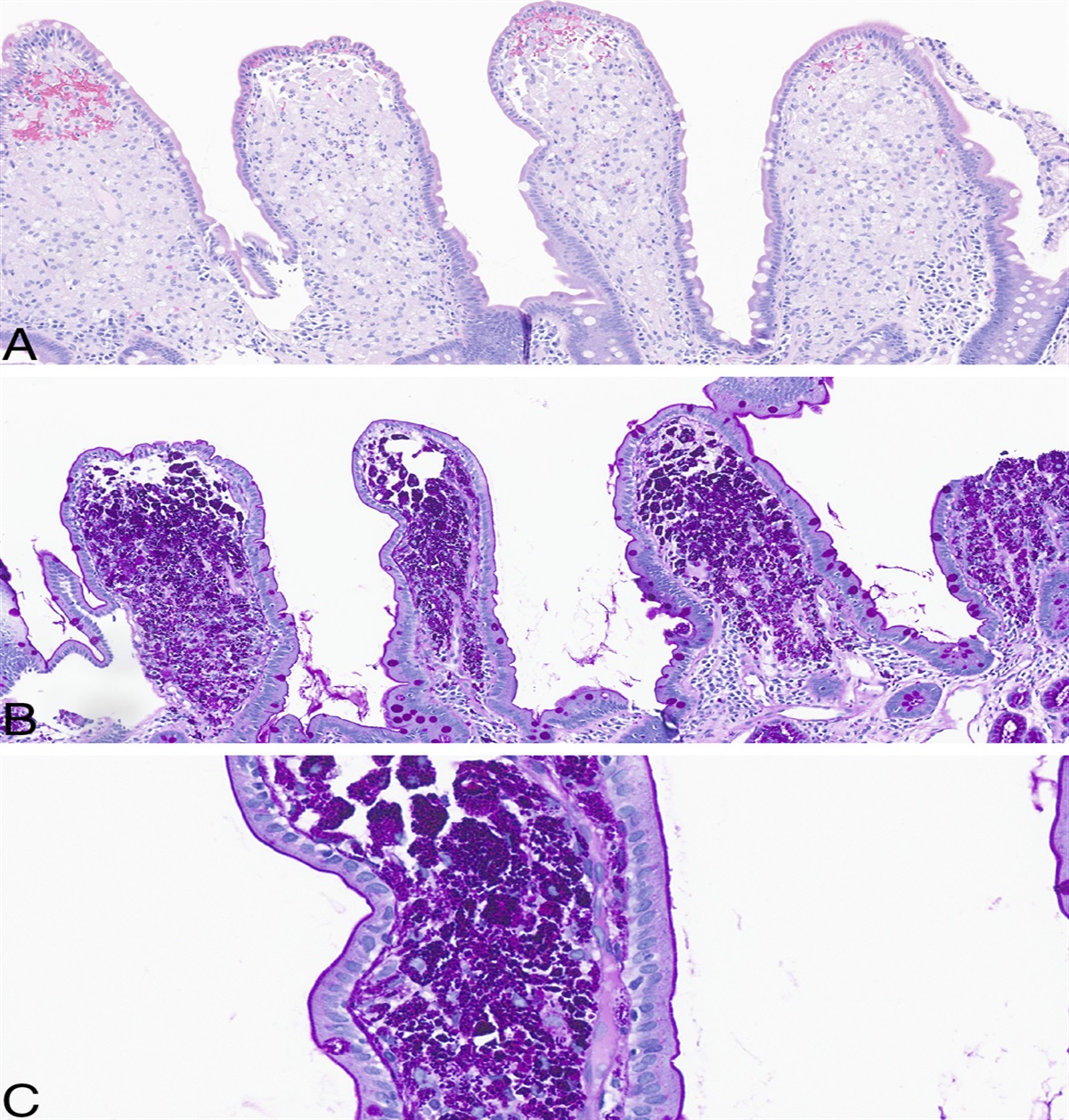
 Figure 2.:
Figure 2.: Clusters of goblet-like mucinous cells with invasion into and through the lamina propria (10×).
 Figure 3.:
Figure 3.: High-power view of cohesive groups of goblet-like mucinous cells. Nuclear atypia is mild, and mitotic figures are inconspicuous (20×).
 Figure 4.:
Figure 4.: Cytokeratin AE1/AE3 highlights the colonic mucosa and the infiltrative goblet cell tumor (10×).
 Figure 5.:
Figure 5.: Chromogranin highlights scattered endocrine cells (10×).
 Figure 6.:
Figure 6.: CT of the abdomen/pelvis with contrast demonstrating mild soft-tissue thickening at the appendiceal orifice and a diameter of 0.68 cm of the appendix, with no periappendiceal inflammatory changes. CT, computed tomography.
DISCUSSIONAppendiceal cancer is categorized into 2 main types: epithelial and neuroendocrine. Epithelial appendiceal cancer originates in the epithelial cells that line the appendix. IHC staining will show cells that stain positive for cytokeratin AE1/AE3, markers used to identify epithelial tumors.1 By contrast, neuroendocrine appendiceal cancer originates from enterochromaffin cells, the dominant type of intestinal epithelial enteroendocrine cell.2 Cells will stain positive for chromogranin and synaptophysin on IHC staining. GCA is an aggressive subtype of appendiceal cancer that histologically has features of both epithelial and neuroendocrine types, as seen in Figures 4 and 5. Incidence is rare, reported to be 0.01 to 0.05 per 100,000 per year.3 Although there are no established risk factors for GCA, some cases have shown an association with schistosomiasis and a proclivity for the White race.4 Clinical presentation is varied, ranging from abdominal discomfort to appendicitis to ovarian masses, but can also be asymptomatic. It is common for appendiceal cancer to have metastasized nodally or intraperitoneally by time of discovery because of the thin wall of the appendix, thus prognosis can be poor.5 The 5-year survival rate for GCA ranges from approximately 91% for Stage I cancer to a dismal 19% for Stage IV cancer, using the Tumor, Node, Metastasis staging system for appendiceal carcinomas.3 This tumor is usually an incidental finding after an appendectomy for an acute appendicitis and is uncommonly found through colonoscopy, as in our patient. The appendiceal orifice is a key landmark that should be identified on all colonoscopies (unless the patient does not have a cecum) to ensure completeness of the procedure, with low threshold to biopsy abnormal-appearing tissue. Although GCAs are rare and evidence-based guidelines are not available, current management is similar to that of colon cancer with a right hemicolectomy for localized disease with possible adjuvant chemotherapy based on the surgical pathology, followed by post-treatment surveillance.6 This case highlights the importance of identification of the appendiceal orifice in all colonoscopies and tissue sampling in cases of atypical-appearing anatomy.
DISCLOSURESAuthor contributions: R. Reese drafted the manuscript. K. Kozacek and L. Jeffrey critically revised the manuscript for important intellectual content. P. Voorhees provided pathological samples for the case report. All authors approved the final version of the paper for publication. K. Kozacek is the article guarantor.
Financial disclosure: None to report.
Previous presentation: Maryland ACP Mulholland-Mohler Residents Meeting; May 5, 2022; Baltimore, MD; The American College of Gastroenterology Annual Scientific Meeting 2022; October 24, 2022; Charlotte, NC.
Disclaimer: The views expressed in this article are those of the authors and do not reflect the official policy of the Department of Defense or the U.S. Government.
Informed consent was obtained for this case report.
REFERENCES 1. Bockstal MR. Stains and CD Markers, Cytokeratin AE1/AE3. Pathology Outlines. (https://www.pathologyoutlines.com/topic/stainsae1ae3.html). Last updated June 16, 2022. Accessed May 24, 2023. 3. Melnitchouk N, Meyerhardt JA. Epithelial tumors of the appendix. UpToDate. (https://www.uptodate.com/contents/epithelial-tumors-of-the-appendix). Last updated February 22, 2022. Accessed January 23, 2023. 4. Kelly KJ. Management of appendix cancer. Clin Colon Rectal Surg. 2015;28(4):247–55. 5. Lambert LA. Appendiceal Cancer and Tumors. National Organization for Rare Disorders. (https://rarediseases.org/rare-diseases/appendiceal-cancer-tumors/). Last updated November 25, 2019. Accessed May 24, 2023. 6. Tsang ES, McConnell YJ, Schaeffer DF, et al. Outcomes of surgical and chemotherapeutic treatments of goblet cell carcinoid tumors of the appendix. Ann Surg Oncol. 2018;25(8):2391–9.
Comments (0)