
Remember me


Complete esophageal obstruction (CEO) is characterized by progressive dysphagia and the inability to tolerate secretions because of severe esophageal lumen stenosis. Diagnosis is established via endoscopic and esophagram visualization of a “blind” esophageal pouch.1 There are few studies investigating the incidence of CEO; however, Lawson et al2 found that approximately 5% of patients undergoing head and neck radiation therapy will subsequently experience CEO. Piotet et al3 found 90% of esophageal and pharyngeal strictures were because of organic etiologies of which 45% were benign (eg, peptic, corrosive ingestion, and eosinophilic esophagitis). Squamous cell carcinoma of the esophagus was the most frequent malignant etiology (38%), followed by esophageal or gastric adenocarcinoma (20%). Although enteral feeding can limit malnutrition, the quality of life is substantially affected.4 Endoscopic procedures such as balloon dilation or esophageal stenting can successfully treat stenosis; however, there are no guideline-based treatment strategies of CEO, given its scarcity.5
Zollinger-Ellison syndrome (ZES) is characterized by gastric acid hypersecretion via gastrin-secreting neuroendocrine tumors and has an incidence of 1.7 per 100,000 people in the United States, of which 80% occur sporadically and 20% are associated with multiple neuroendocrine neoplasia type 1 (MEN1).6,7 Diagnosis of ZES is established with elevated gastrin levels (>10 times normal limit) and low gastric pH (pH < 2) in patients off of proton pump inhibitors. Patients with negative screening tests but strong suspicion can also undergo secretin stimulatory test or chromogranin A level.7 Unfortunately, the mean time to diagnosis is 6 years, which is mostly attributed to masked symptoms from antisecretory medications and decreased testing.8 ZES is often well-controlled with high dose proton pump inhibitors and sporadic gastrinomas without metastatic spread can also be eradicated with surgical resection.9
Owing to advancements in antisecretory medications, abdominal pain (47.1%), nausea (45.6%), reflux (41.2%), and vomiting (30.9%) are the most common symptoms associated with ZES, and mortality trends have shifted from those because of acid hypersecretion to being principally related to underlying comorbidity.9–11 Therefore, this case documents the sequala of CEO in a modern-day patient with ZES.
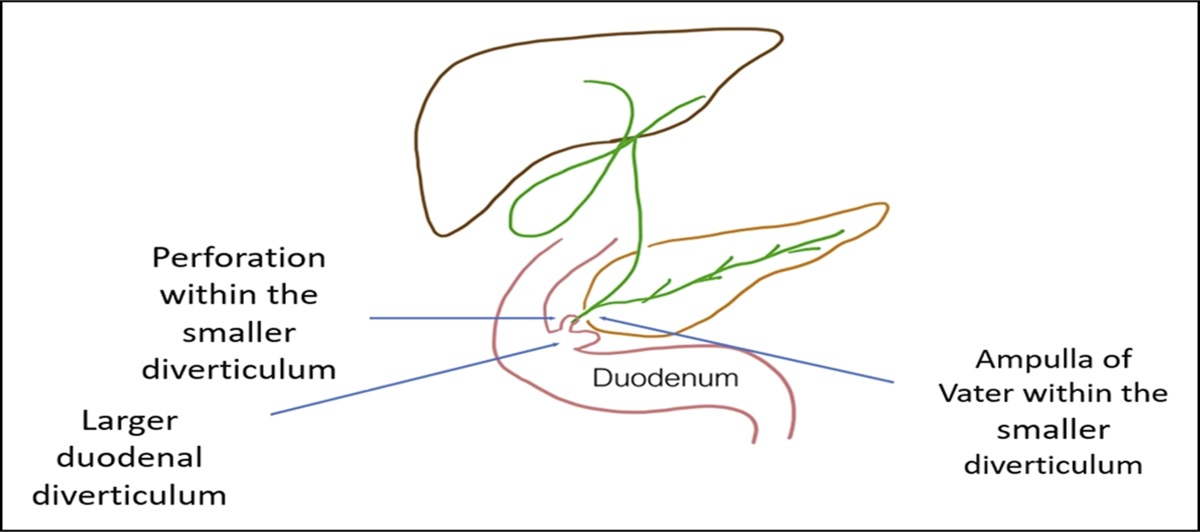
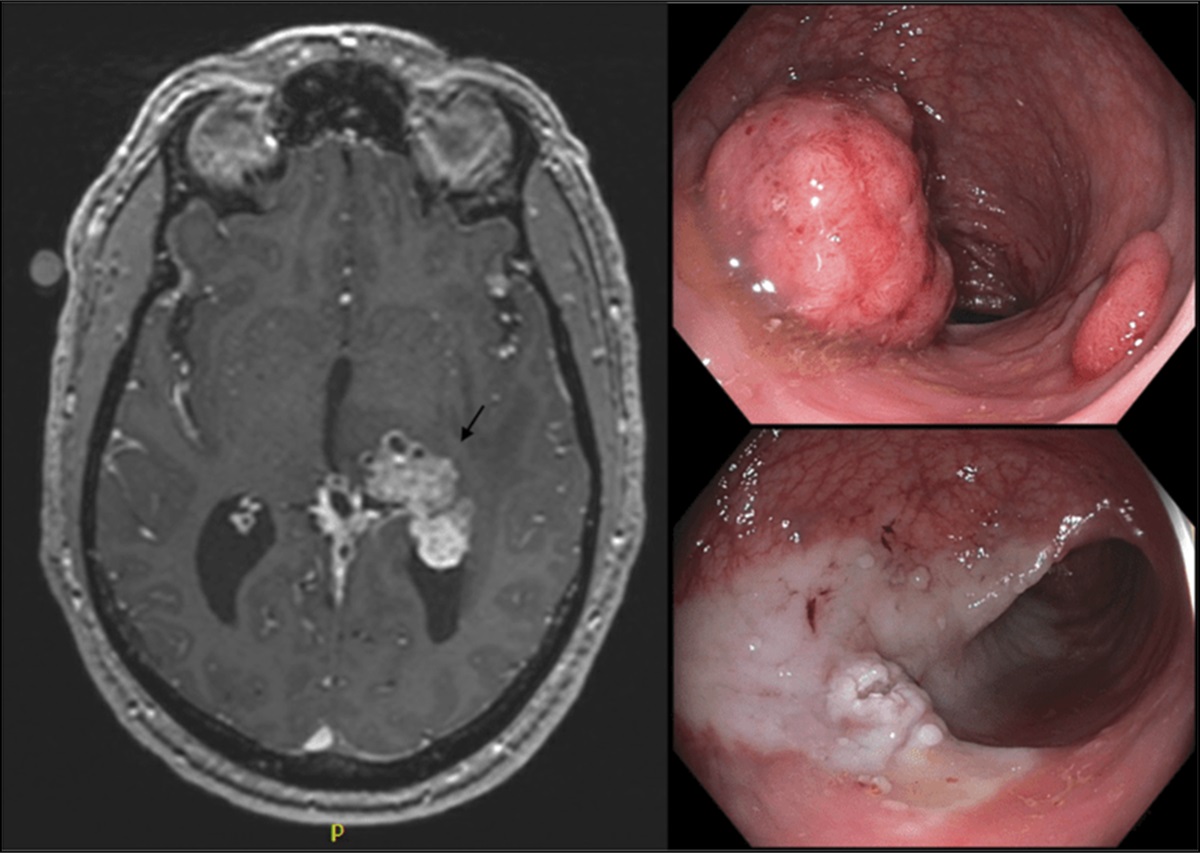
CASE REPORTA 73-year-old man with a history of human immunodeficiency virus on highly active antiretroviral therapy, gastroesophageal reflux disease, and ZES presented with inability to tolerate solids, liquids, or secretions. Two years earlier, he was diagnosed with ZES after recurrent episodes of abdominal pain, nausea, and melena with esophagogastroduodenoscopy (EGD) demonstrating severe erosive esophagitis with multiple, deep duodenal ulcers. Diagnostic testing revealed a gastrin level of 927 pg/mL and gastric pH of 7 on twice daily pantoprazole 40 mg. Subsequent serum chromogranin A level was elevated at 1,836, and gastrinoma was confirmed after a PET scan demonstrated a DOTATATE avid mass in the first portion of the duodenum with evidence of local lymph node metastasis (Figure 1). MEN1 screening was negative.
 Figure 1.:
Figure 1.: Ga-68 DOTATATE scan demonstrating avid uptake in the first part of the duodenum.
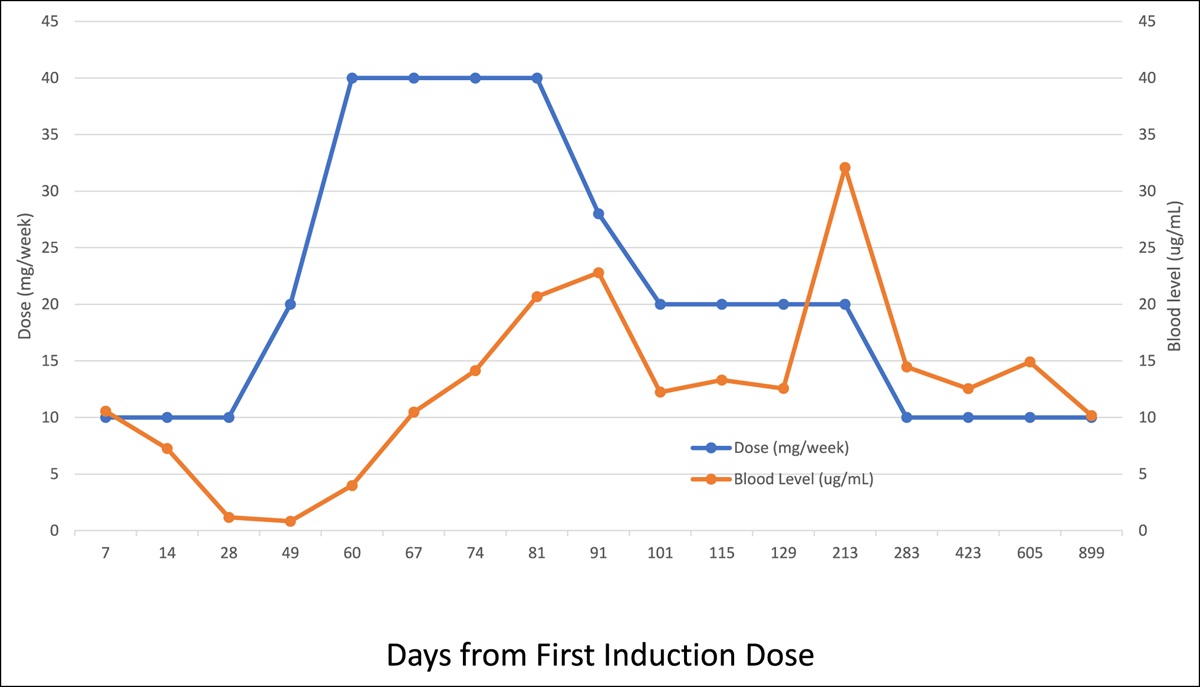
After diagnosis, his gastrin level continued to increase, peaking at 1,941 pg/mL, although his medical therapy was maximized to omeprazole 180 mg/d and famotidine 80 mg/d. Fortunately, his symptoms mildly improved, and he was able to tolerate a clear liquid diet before tumor resection with distal gastrectomy, resection of first portion of duodenum, Roux-en-Y hepaticojejunostomy, and truncal vagotomy after which gastrin normalized to 87 pg/mL. Unfortunately, the patient's esophageal peptic strictures caused significant dysphagia requiring recurrent esophageal stents which provided temporary relief, often lasting 2–3 weeks. In total, he underwent 21 EGDs and 7 esophageal stents because he was deemed a poor candidate for esophageal reconstruction by jejunal or colonic interposition because of poor nutritional status after losing 77 pounds despite enteral and total parenteral nutrition.
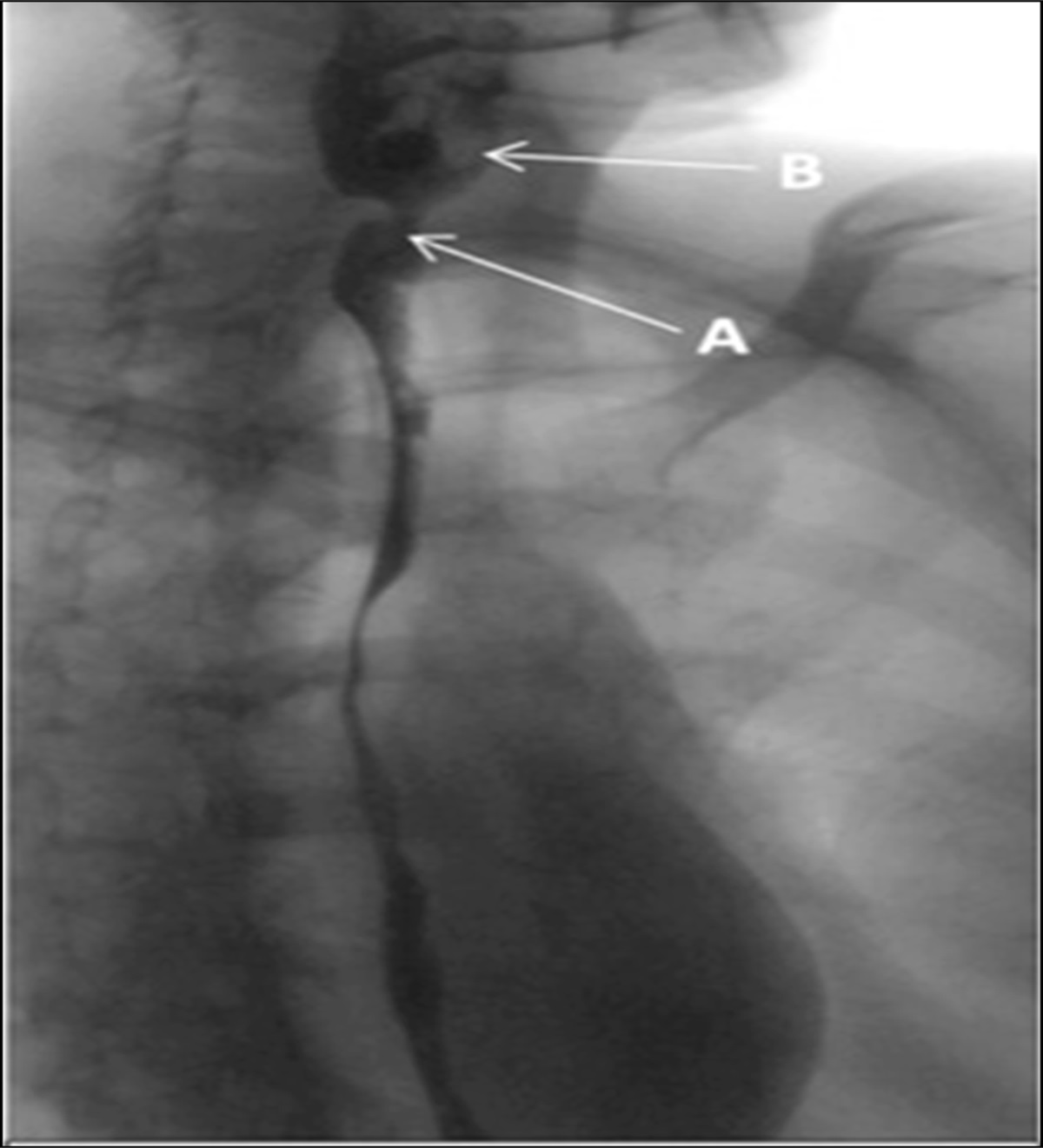
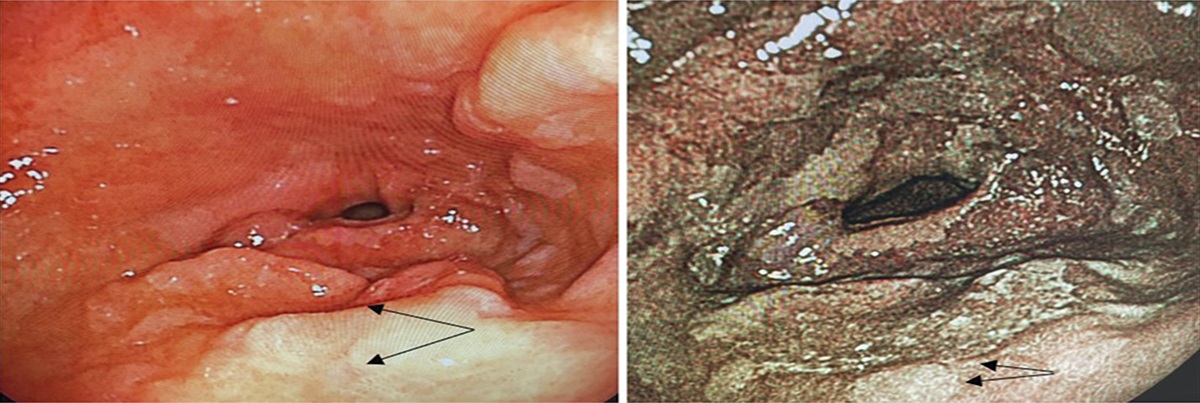
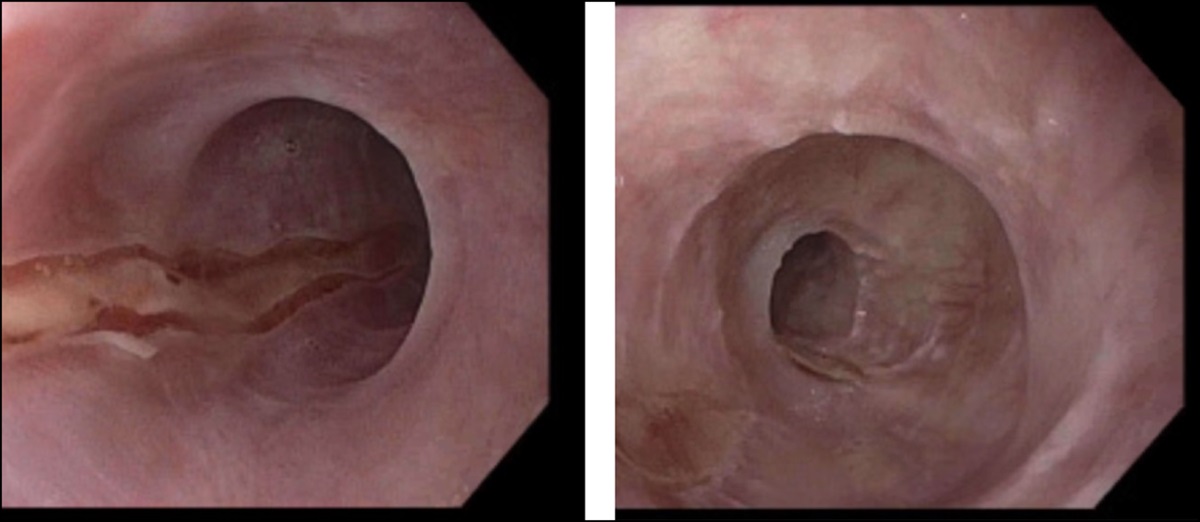
At the time of presentation, he was unable to swallow his secretions and had profound weakness because of malnutrition. Barium esophagram revealed high-grade focal luminal narrowing of the midthoracic esophagus with a luminal diameter of 5 mm, followed by a high-grade narrowing in distal-thoracic esophagus with no traversing of contrast after 20 minutes (Figure 2). EGD was performed and revealed a 7-mm stricture that was dilated using a through-the-scope balloon with mild postdilation mucosal bleeding (Figure 3). An ultraslim endoscope was then advanced to a second high-grade stricture at approximately 35 cm from incisors resulting in a blind pouch (Figure 4).
 Figure 2.:
Figure 2.: Barium esophagram revealing a high-grade stricture in midthoracic esophagus, followed by another stricture leading to complete esophageal obstruction without passage of contrast.
 Figure 3.:
Figure 3.: Endoscopic view of postdilation of first severe stricture located approximately 25 cm from incisors.
 Figure 4.:
Figure 4.: Endoscopic view of second stricture that resulted in blind pouch at approximately 35 cm from incisors.
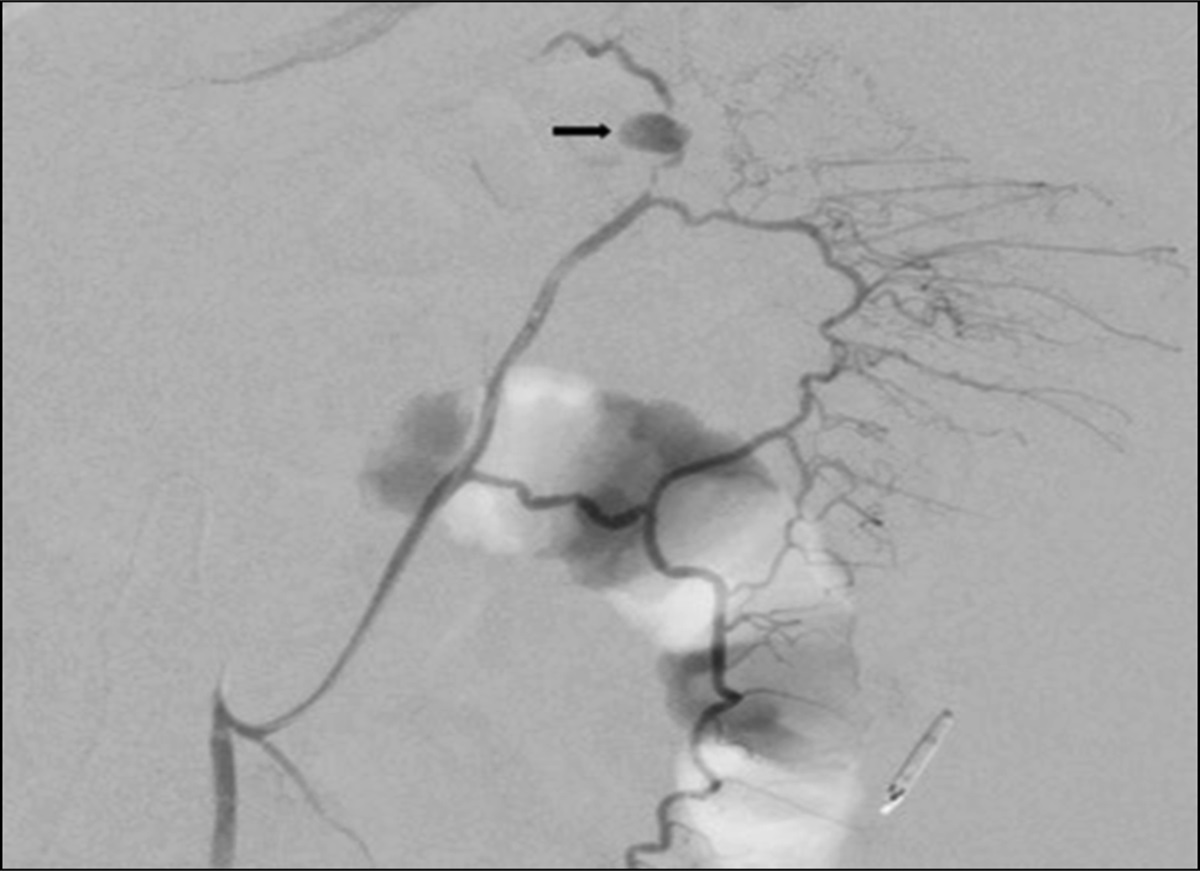
During subsequent EGD, esophageal lumen restoration was attempted using an adult endoscope that was introduced into the mouth and advanced to the blind lumen while a second ultraslim endoscope, operated by a second endoscopist, was advanced retrograde from the PEG site into the proximal esophagus. Because the 035 Biliary wire could not be advanced anterograde into stomach despite endoscopic and fluoroscopic guidance, the lumen was then attempted with fluoroscopic guidance of an EUS echo tip ultra. This was unable to puncture through the distal limb of stricture. Finally, an anterograde passing of a Savary guidewire was attempted but was unsuccessful because the 2 blind loops were 6 cm apart in a different alignment (Figure 5). Patient continues enteral feeding.
 Figure 5.:
Figure 5.: Fluoroscopic imaging displaying attempt at combined anterograde and retrograde dilation.
DISCUSSIONSevere peptic ulcer disease was once the number one cause of morbidity and mortality in patients with ZES,12 and the development of effective acid suppressive therapy has decreased complications from gastric acid hypersecretion and the rates of total gastrectomy.10 This case demonstrates a patient with ZES who developed CEO despite management with maximal acid suppressive therapy, surgical resection, multiple balloon dilations, and numerous esophageal stents. Interestingly, Hoffman et al13 found a 3-fold increased risk of esophageal strictures and 5-fold increased risk of Barrettes esophagus in MEN1-associated compared with sporadic ZES. A large prospective study and comparative literature review of patients with MEN1-associated ZES reported zero deaths from gastric acid hypersecretion in studies after 1995.14 An extensive literature review did not reveal any reports of CEO in patients with ZES.
Surgery for severe esophageal stricture and CEO is typically reserved when balloon dilation and stent placement is ineffective or unfeasible.15 Unfortunately, frailty from malnutrition can limit surgical candidacy, leaving few endoscopic lumen restoration options. Combined anterograde and retrograde dilation and per-oral endoscopic tunneling for the restoration of the esophagus are 2 endoscopic recanulation techniques that have been shown to be successful but are challenging in complex strictures greater than 3 cm.1,16–19
DISCLOSURESAuthor contributions: All authors made substantial contributions to the design of the work, interpretation of data, and manuscript revisions. S. Clayton gave the final approval of the work to be published. F. Chanaa is the article guarantor.
Financial disclosure: None to report.
Previous presentation: Previously presented at the American College of Gastroenterology Annual Scientific Meeting 2022; October 24, 2022; Charlotte, NC.
Informed consent was obtained for this case report.
REFERENCES 1. Perbtani Y, Suarez AL, Wagh MS. Emerging techniques and efficacy of endoscopic esophageal reconstruction and lumen restoration for complete esophageal obstruction. Endosc Int Open. 2016;4(2):E136–42. 2. Lawson JD, Otto K, Grist W, Johnstone PA. Frequency of esophageal stenosis after simultaneous modulated accelerated radiation therapy and chemotherapy for head and neck cancer. Am J Otolaryngol. 2008;29(1):13–9. 3. Piotet E, Escher A, Monnier P. Esophageal and pharyngeal strictures: Report on 1,862 endoscopic dilatations using the Savary-Gilliard technique. Eur Arch Otorhinolaryngol. 2008;265(3):357–64. 4. de Boer MF, Pruyn JF, van den Borne B, Knegt PP, Ryckman RM, Verwoerd CD. Rehabilitation outcomes of long-term survivors treated for head and neck cancer. Head Neck. 1995;17(6):503–15. 5. Fusco S, Kratt T, Gani C, et al. Rendezvous endoscopic recanalization for complete esophageal obstruction. Surg Endosc. 2018;32(10):4256–62. 6. Boyce M, Thomsen L. Gastric neuroendocrine tumors: Prevalence in Europe, USA, and Japan, and rationale for treatment with a gastrin/CCK2 receptor antagonist. Scand J Gastroenterol. 2015;50(5):550–9. 7. Metz DC, Cadiot G, Poitras P, Ito T, Jensen RT. Diagnosis of Zollinger-Ellison syndrome in the era of PPIs, faulty gastrin assays, sensitive imaging and limited access to acid secretory testing. Int J Endocr Oncol. 2017;4(4):167–85. 8. Roy PK, Venzon DJ, Shojamanesh H, et al. Zollinger-Ellison syndrome. Clinical presentation in 261 patients. Medicine (Baltimore). 2000;79(6):379–411. 9. Rossi RE, Elvevi A, Citterio D, et al. Gastrinoma and Zollinger Ellison syndrome: A roadmap for the management between new and old therapies. World J Gastroenterol. 2021;27(35):5890–907. 10. Quatrini M, Castoldi L, Rossi G, Cesana BM, Peracchi M, Bardella MT. A follow-up study of patients with Zollinger-Ellison syndrome in the period 1966–2002: Effects of surgical and medical treatments on long-term survival. J Clin Gastroenterol. 2005;39(5):376–80. 11. Wilcox CM, Seay T, Arcury JT, Mohnen J, Hirschowitz BI. Zollinger-ellison syndrome: Presentation, response to therapy, and outcome. Dig Liver Dis. 2011;43(6):439–43. 12. Meko JB, Norton JA. Management of patients with Zollinger-Ellison syndrome. Annu Rev Med. 1995;46:395–411. 13. Hoffmann KM, Gibril F, Entsuah LK, Serrano J, Jensen RT. Patients with multiple endocrine neoplasia type 1 with gastrinomas have an increased risk of severe esophageal disease including stricture and the premalignant condition, Barrett's esophagus. J Clin Endocrinol Metab. 2006;91(1):204–12. 14. Ito T, Igarashi H, Uehara H, Berna MJ, Jensen RT. Causes of death and prognostic factors in multiple endocrine neoplasia type 1: A prospective study: Comparison of 106 MEN1/Zollinger-Ellison syndrome patients with 1613 literature MEN1 patients with or without pancreatic endocrine tumors. Medicine (Baltimore). 2013;92(3):135–81. 15. van Boeckel PG, Siersema PD. Refractory esophageal strictures: What to do when dilation fails. Curr Treat Options Gastroenterol. 2015;13(1):47–58. 16. Bueno R, Swanson SJ, Jaklitsch MT, Lukanich JM, Mentzer SJ, Sugarbaker DJ. Combined antegrade and retrograde dilation: A new endoscopic technique in the management of complex esophageal obstruction. Gastrointest Endosc. 2001;54(3):368–72. 17. Babich JP, Diehl DL, Entrup MH. Retrograde submucosal tunneling technique for management of complete esophageal obstruction. Surg Laparosc Endosc Percutan Tech. 2012;22(4):e232–235. 18. Maple JT, Petersen BT, Baron TH, Kasperbauer JL, Wong Kee Song LM, Larson MV. Endoscopic management of radiation-induced complete upper esophageal obstruction with an antegrade-retrograde rendezvous technique. Gastrointest Endosc. 2006;64(5):822–8. 19. Wagh MS, Draganov PV. Per-oral endoscopic tunneling for restoration of the esophagus: A novel endoscopic submucosal dissection technique for therapy of complete esophageal obstruction. Gastrointest Endosc. 2017;85(4):722–7.
Comments (0)