The first main finding of this study was that the risk factors of recurrent cough and isolated chronic cough were essentially the same. The second main finding was that the consequences of recurrent cough, such as depressive symptoms, quality of life, and healthcare use, were comparable to those of isolated chronic cough.
Because recurrent cough lacks an established definition in adults, it was defined by the authors considering the frequency and duration of common cold-associated cough. Adults catch approximately 2–3 colds annually [24]. Thus, recurrent cough was defined as ≥ 3 cough episodes during the past year. The definition of ≥ 1 week for episode duration was chosen because common cold-associated cough usually resolves in 1 week [24], although transient increase in cough reflex sensitivity may last up to 4 weeks [25]. We hypothesised that ≥ 3 cough episodes of more than 1-weeks` duration within a year indicates abnormality, irrespective of the presence of an URTI.
The classic triad of chronic cough background disorders, CRS, asthma, and GERD, was associated with both recurrent cough and isolated chronic cough. Episodic cough in CRS and asthma is understandable given their vulnerability to exacerbations due to infections or environmental factors, whereas GERD has previously been associated mostly with prolonged or chronic, continuous cough [2, 15]. The episodic nature of reflux-cough could be attributable to changes in diet and lifestyle since the benefits of anti-acid drugs alone are limited. Because all background disorders of isolated chronic cough were also risk factors for recurrent cough, fluctuating control of the background disorders seems like a logical explanation for the relapsing and remitting course of cough. Cold temperature could also contribute to seasonal changes in cough among subjects with increased cough reflex sensitivity [26]. The results also suggest that the typical background disorders of chronic cough may exist in recurrent episodes of only 1 weeks` length, however the episode durations could not be specified in this study. Considering that most people do not seek medical advice for current cough of any length [27, 28], and that healthcare resourcing may limit early access to doctor`s evaluation, a routine question about the history of recurrent cough could help to reach the undiagnosed background disorders.
Despite the noticeable similarity of the risk factors in recurrent and isolated chronic cough, there were some specific risk factors for recurrent cough in this elderly population. Surprisingly, those were male gender, younger age, and analgesic intolerance. The cough reflex is reported to be more sensitive in women than in men [29], and the patients in cough clinics are predominantly females [30]. In this context, the reason for the association of male gender with recurrent cough is unclear. Smoking does not seem to explain it, because very few subjects were current smokers, and the association was independent from ever-smoking in the multivariate analysis. The protective association of age with recurrent cough could at least partly be attributable to decreasing URTI-incidence towards the higher age, as previously reported [31]. Intolerance to analgesics was also associated with recurrent cough, for an unknown reason. Overall, these are atypical risk factors of cough and warrant future research.
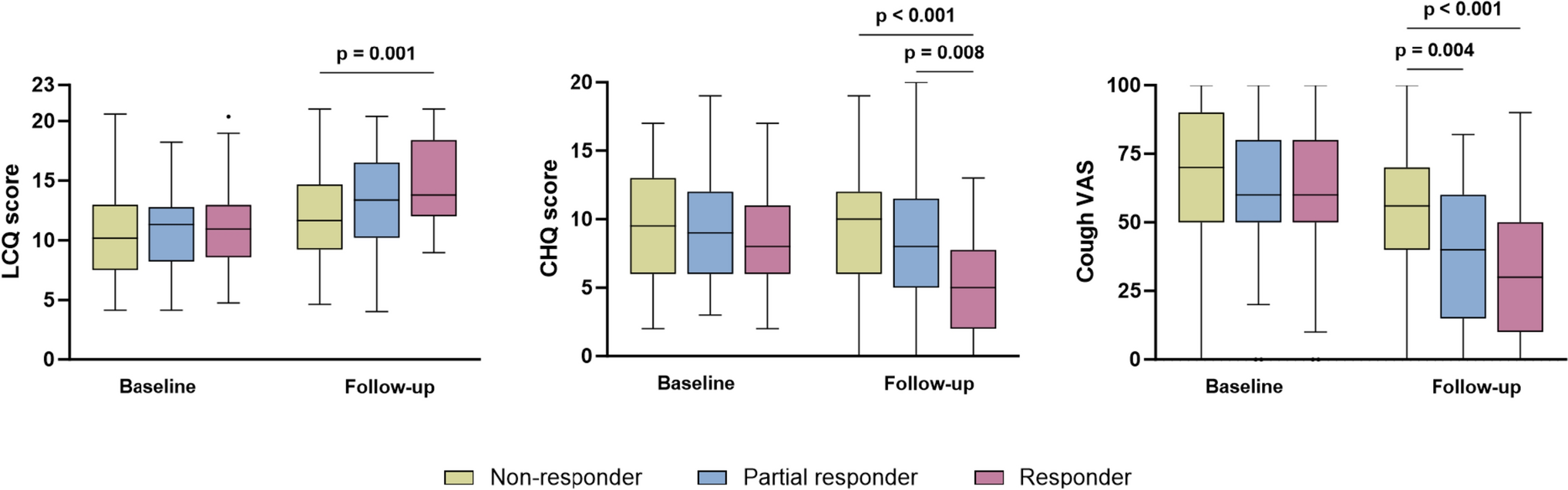
Chronic cough can predispose to impairment in the quality of life [27], depression [32, 33], and repeated healthcare use [28, 34]. All quality-of-life scores by LCQ were statistically significantly lower in subjects with recurrent cough than in those with isolated chronic cough. However, LCQ total scores did not reach the clinically meaningful difference of 1.3 points [35, 36]. Depressive symptoms were more common among subjects with recurrent cough, although not statistically significantly. Furthermore, recurrent cough led to more doctor`s visits than isolated chronic cough. In this elderly population, the personal and socioeconomic impact of recurrent cough was at least as substantial as of isolated chronic cough.
The prevalence of recurrent cough was 3.8%. This was in the circumstances of the early pandemic, when the incidence of COVID-19 infections in this population [16], and URTIs in Finland [37], were low. Considering this, URTI-associated cough episodes were likely fewer than in the current time. However, no comparative data could be found on the prevalence of recurrent cough in community-based adult populations. From another perspective, recurrent cough did not disappear during low URTI-incidence, which may suggest other reasons for cough recurrence. Among subjects with recurrent and current cough, 34% reported that the current episode was triggered by an URTI. This suggests that most current acute or subacute episodes were triggered by something else. However, the current episode was expectedly more often URTI-related in subjects with recurrent cough than in those with isolated chronic cough. Of note, the prevalence of isolated chronic cough was 4.6%. Because of the mutually exclusive definitions, isolated chronic cough included only continuous chronic coughers who did not report overlapping recurrent cough. In contrast, according to the currently recommended definition of ≥ 8 weeks, the total prevalence of chronic cough was much higher among all respondents of this survey (13.5%) [16]. This means that most cases of chronic cough involved either precursing recurrent cough or episodic exacerbations of chronic cough.
There were several shortcomings in this study. Despite of the rather low response rate, the age and gender distributions of the target population and the respondents were highly comparable. However, the subjects with particularly problematic cough may have been more willing to participate than others. The population consisted of elderly persons who were able to respond to an email survey. Therefore, younger and disabled persons were excluded, and the generalisability of the results should be studied in other populations. However, studying cough specifically in the elderly can be regarded also as a strength, considering the globally ageing populations. Important background disorders of cough, namely bronchiectasis and chronic obstructive pulmonary disease, could not be included in the final risk factor analyses due to low prevalence in the study population. The STOP-questionnaire may overestimate the prevalence of OSA [21]. Current smokers and thus the impact of smoking was underrepresented in the results. Angiotensin-converting-enzyme inhibitor use was not investigated separately from other antihypertensive drugs and was not included in the analyses. Recall bias may somewhat affect the reporting of recurrent cough episodes. The study design does not allow confirmation of causality. Also, all data was self-reported and hence include variation in how the subjects experience and report symptoms [38]. However, this was controlled with the variable “symptom sum”. A strength of the study is that it was conducted with a comprehensive questionnaire which was designed to study specifically the epidemiology and consequences of cough. It included validated questionnaires to investigate cough-related quality of life and several cough background disorders, which may help to include symptomatic background disorders that are yet undiagnosed. This study was the first one to define risk factors and consequences for recurrent cough in adults, a phenomenon that is recognisable in the clinical setting but so far little studied.




Comments (0)