
Remember me


The gastrointestinal tract is a well-known extranodal site of lymphomas. B-cell lymphomas are the predominant lineage, and the T-cell lineage comprises only 13%–15% of lymphomas.1 Intestinal T-cell lymphomas consist of various entities, including enteropathic T-cell lymphoma (EATL), monomorphic epitheliotropic intestinal T-cell lymphoma (MEITL), intestinal T-cell lymphoma, not otherwise specified (NOS), and indolent T/natural killer cell (NK) lymphoproliferative disorders.2 These malignancies are primarily found in the stomach and/or small intestine, with colon involvement being rare.3 In most distant organ metastases from colorectal malignancy, the liver and lungs are commonly involved. Metastasis to the brain and other extraintestinal sites is uncommon.4 Primary metastasis is exceedingly rare with only a few case reports describing this presentation in patients with colorectal cancer and gastrointestinal malignancies involving the stomach and small bowel. We present an elderly patient who presented with confusion and lethargy found to have cerebellar and leptomeningeal carcinomatosis. A sigmoid colon mass revealed the diagnosis of intestinal T-cell lymphoma, NOS. Interestingly, the patient also had a suspicious muscular lesion in her psoas, demonstrating 2 uncommon sites of metastasis with an uncommon site of primary malignancy.
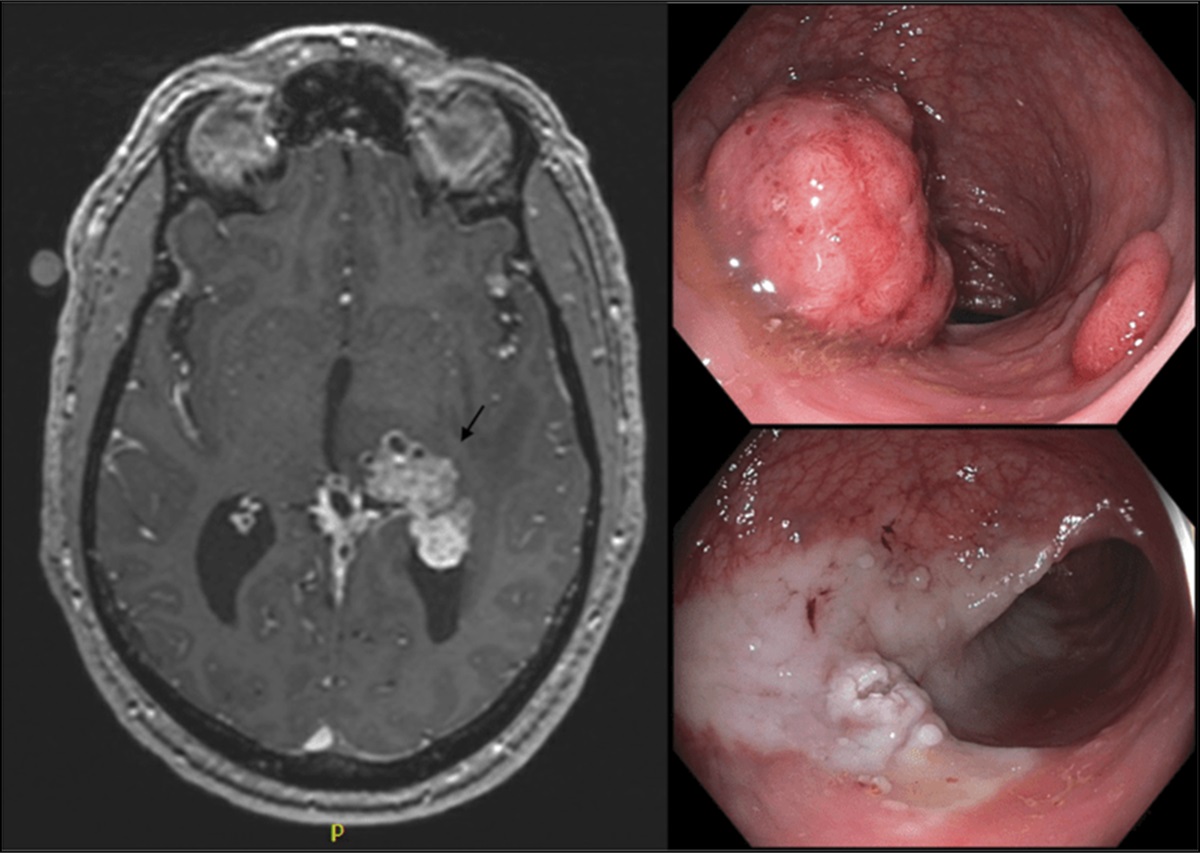
CASE REPORTA 75-year-old woman with a history of primary biliary cholangitis initially presented to an outside facility for an elective L3-4 laminectomy and fusion which was complicated by an inferior ST-segment elevation myocardial infarction and seizure. Neurology workup at that time included magnetic resonance imaging (MRI) demonstrating leptomeningeal and parenchymal enhancement with signal abnormality in the medial cerebellar hemispheres, greater in the left. Lumbar puncture was negative for infectious etiology. Continuous electroencephalogram did not show epileptiform activity. Her mentation was reported to be at her baseline, and she was discharged home, although re-presented the next day with confusion and lethargy.
Repeat MRI showed worsening of the cerebellar lesions and leptomeningeal enhancement in the posterior fossa with a new left parietal lobe lesion and leptomeningeal enhancement in the basal cisterns and left cerebral convexity. Computed tomography of the chest, abdomen, and pelvis revealed a 5.5 × 3.9 cm aneurysmal thickening of the proximal sigmoid colon near the junction of the descending colon as seen in Figure 1. There was no evidence of malignancy or metastatic disease in the chest or other areas of the abdomen and pelvis. MRI spine demonstrated diffuse leptomeningeal enhancement of the spinal cord and cauda equina suspicious for leptomeningeal carcinomatosis with incidental soft tissue mass in the right psoas muscle measuring 2.9 cm concerning for muscular metastasis.
 Figure 1.:
Figure 1.: Aneurysmal thickening of the proximal sigmoid colon, measuring 5.5 x 3.8 cm, near the junction of the descending colon.
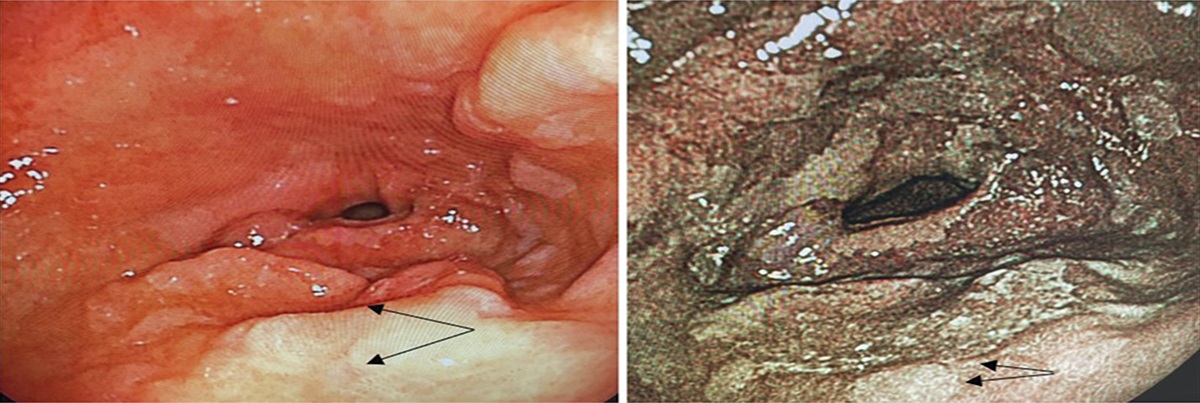
Carcinoembryonic antigen was elevated at 12.1 ng/mL. Flexible sigmoidoscopy revealed a fungating, infiltrative, polypoid, and ulcerated obstructing mass at the sigmoid colon (Figure 2). The mass was partially circumferential and measured 9 cm in length. Cold forceps biopsy was sent for histology. Pathology showed ulcerated and necrotic tissues composed of a monotonous infiltrate of atypical lymphocytes. Large irregular nuclear contour was noted with prominent nucleoli as seen in Figure 3. Immunostains found the atypical cells to be positive for CD43, CD45, C2, CD30, and CD56 (Figure 4), whereas negative for CD3, CD4, CD5, granzyme B, PAX5, CD20, CD15, ALK 1, and Epstein-Barr encoding region in situ hybridization. Based on immunostains and a negative history of enteropathy, including celiac disease, a final diagnosis of intestinal T-cell lymphoma NOS was made.
 Figure 2.:
Figure 2.: (A and B) Flexible sigmoidoscopy revealed a fungating, infiltrative, polypoid and ulcerated partially obstructing large mass found in the sigmoid colon 40 cm from the anal verge. The mass measured 9 cm in length and was partially circumferential.
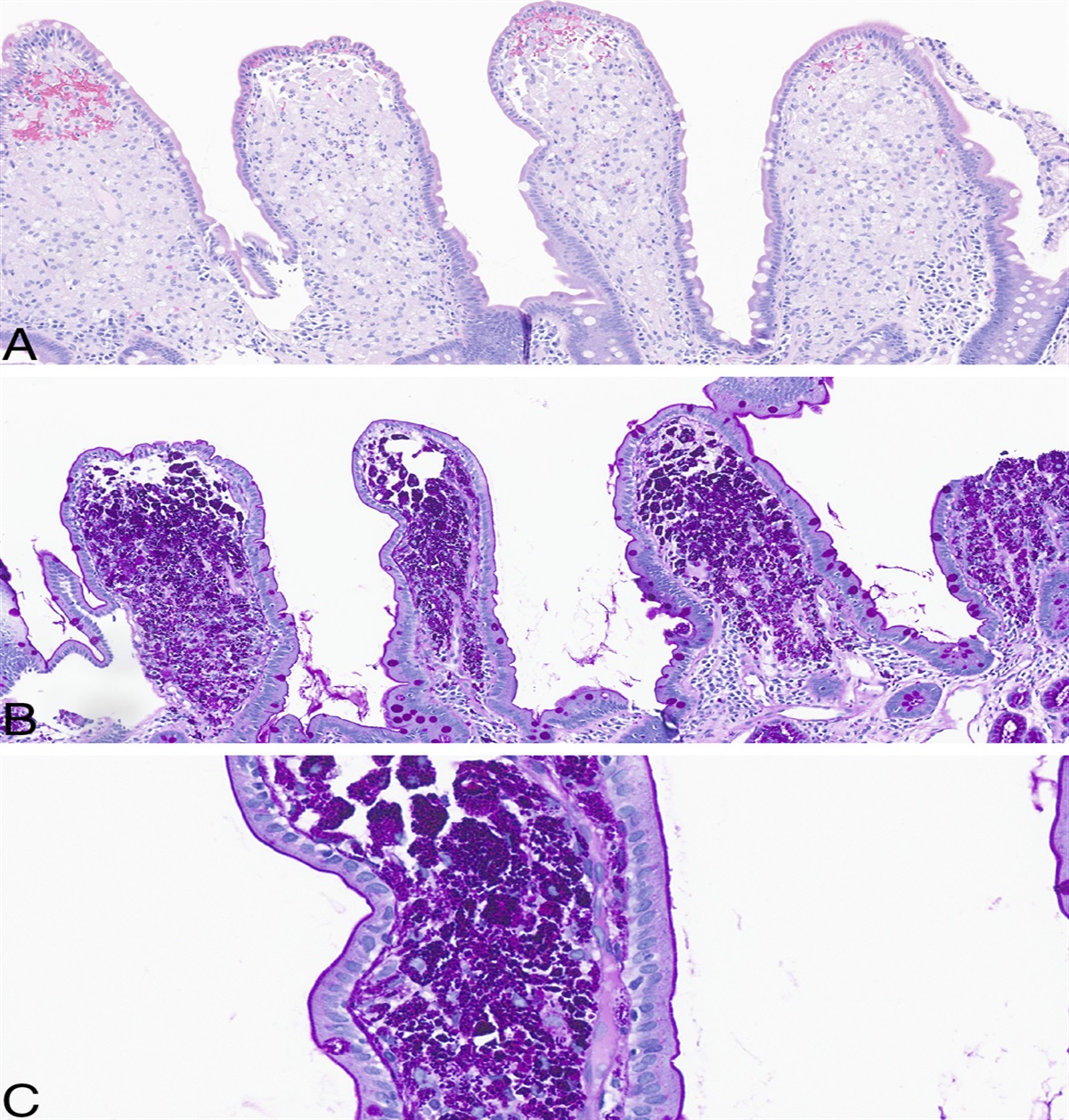
 Figure 3.:
Figure 3.: Histological images with hematoxylin & eosin stains of colonic specimens obtained by endoscopic biopsy. (A) Low power view (4x) displays necrotic tissue containing a monotonous infiltrate of atypical large lymphocytes; (B) at intermediate power (20x), can see infiltrate of atypical large lymphocytes with irregular nuclear contours and prominent nucleoli; (C) at high power (60x) and (D) (100x) can see irregular nuclear contours and prominent nucleoli with mitotic forms.
 Figure 4.:
Figure 4.: Immunohistochemical staining (IHC) with positive (brown) membranous staining in cells of interest. Blue counter stain is hematoxylin. (A) IHC: CD2; (B) IHC: CD43; (C) IHC: CD 30; (D) IHC: CD56.
Given her clinical deterioration, the high likelihood of malignancy with no surgical option, the family elected to pursue hospice and the patient was discharged to home hospice.
DISCUSSIONThe gastrointestinal tract is a common site of extranodal non-Hodgkin lymphoma, accounting for 30%–40% of cases. Most lymphomas are comprised of B cell origin. T-cell lymphomas of the gastrointestinal tract as a primary site is rare, comprising 10%–15% of all non-Hodgkin lymphoma and 1%–4% of all gastrointestinal malignancies.3,5
Primary gastrointestinal T-cell lymphomas are divided further into EATL, MIETL, and intestinal T-cell lymphoma NOS. The distinction between these subtypes is made on clinical history and immunohistochemical expression.6 EATL is the most common and associated with celiac disease and expressions of CD3, cytotoxic-granule-associated proteins, and T cell receptor αβ.6 MEITL immunohistochemical expression includes CD3, CD8, and CD56, with tumor cells derived from γδ cells.6 Intestinal T-cell lymphoma NOS does not have a specific immunohistochemical expression pattern and is typically a diagnosis of exclusion.6 Indolent T/NK lymphoproliferative disorders typically display CD3 and CD4 positivity.7
Location of these malignancies is predominantly in the stomach, with approximately 50% found in this organ. The next most common is the small bowel, registering approximately 20%–40% of cases, whereas the colon is a rare site at approximately 5%.3,8 Our case demonstrated an intestinal T-cell lymphoma in the sigmoid colon, a rare location for this type of malignancy. Our patient lacked CD3, CD4, and EBER-ISH staining on pathologic review. The morphology of the cells along with her negative history of celiac disease or other enteropathies led to the diagnosis of intestinal T-cell lymphoma NOS and exclusion of EATL, MEITL, and T/NK lymphoproliferative disorders.
It is estimated that colorectal cancer results in brain metastasis in 0.6%–3.2% of cases. This is typically found in the latter disease and is not normally seen as a primary site of metastasis. Patients with lung metastasis have a higher association of developing brain metastasis, whereas mutations in KRAS and rectal location have also been discussed as a risk factor.9,10
Brain metastasis originating from the colon is an exceptionally rare occurrence, with only a few case reports documenting such presentations. Among these cases, the described colonic cancers predominantly manifest as adenocarcinoma.11–14 Central nervous system involvement including metastasis in intestinal T-cell lymphoma have been described via case reports in the past. To our knowledge, 6 cases have been described, although all were revealed to be EATL with primary site of malignancy being the stomach or small bowl.15–20
Our case represents the first documented case of a colonic intestinal T-cell lymphoma with primary brain metastasis. Furthermore, our patient was found to have a sigmoid colon mass, not known to be associated with the increased risk of metastasis to the brain. Although exceedingly rare, colonic lesions do present as a possible primary source for metastasis in patients presenting with brain lesions.
DISCLOSURESAuthor contributions: M. Bourmaf conducted literature review and drafting of the manuscript. KK Motwani: corresponding author, procurement of images, and drafting of the manuscript. I. McCool, Z. Singh, M. Kallen, and M. Koka: procurement and commentary on pathology slides and revision of the article for important intellectual content. U. Wong: revision of the article for important intellectual content and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Nishimura MF, Nishimura Y, Nishikori A, Yoshino T, Sato Y. Primary gastrointestinal T-cell lymphoma and indolent lymphoproliferative disorders: Practical diagnostic and treatment approaches. Cancers (Basel). 2021;13(22):5774. 2. van Vliet C, Spagnolo DV. T- and NK-cell lymphoproliferative disorders of the gastrointestinal tract: Review and update. Pathology. 2020;52(1):128–41. 3. Kohri M, Tsukasaki K, Akuzawa Y, et al. Peripheral T-cell lymphoma with gastrointestinal involvement and indolent T-lymphoproliferative disorders of the gastrointestinal tract. Leuk Res. 2020;91:106336. 4. Mongan JP, Fadul CE, Cole BF, et al. Brain metastases from colorectal cancer: Risk factors, incidence, and the possible role of chemokines. Clin Colorectal Cancer. 2009;8(2):100–5. 5. Bautista-Quach MA, Ake CD, Chen M, Wang J. Gastrointestinal lymphomas: Morphology, immunophenotype and molecular features. J Gastrointest Oncol. 2012;3(3):209–25. 6. Jaffe ES, Chott A, Ott G, et al. Intestinal T-cell lymphoma. In: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th edn. IARC, World Health Organization: Lyon, 2017, pp 372–80. 7. Sanguedolce F, Zanelli M, Zizzo M, et al. Indolent T-cell lymphoproliferative disorders of the gastrointestinal tract (iTLPD-GI): A review. Cancers (Basel). 2021;13(11):2790. 8. Psyrri A, Papageorgiou S, Economopoulos T. Primary extranodal lymphomas of stomach: Clinical presentation, diagnostic pitfalls and management. Ann Oncol. 2008;19(12):1992–9. 9. Christensen TD, Spindler KLG, Palshof JA, et al. Systematic review: Brain metastases from colorectal cancer—Incidence and patient characteristics. BMC Cancer. 2016;16(260):1–14. 10. Müller S, Köhler F, Hendricks A, et al. Brain metastases from colorectal cancer: A systematic review of the literature and meta-analysis to establish a guideline for daily treatment. Cancers. 2021;13(4):900. 11. Tagayasu Y, Miyamoto Y, Sawayama H, et al. Rectal cancer diagnosed after resection of isolated brain metastasis. Surg Case Rep. 2022;8(52):1–5. 12. Garg PK, Bohidar NP, Sharma MP, et al. Isolated cerebellar metastasis from carcinoma of the colon. Postgrad Med J. 1999;75(880):119–20. 13. Kimura M, Tanishima H, Tatsubayashi T, et al. A case with solitary brain metastatic tumor from colon cancer. Gan To Kagaku Ryoho. 2017;44(12):1388–90. 14. Shaikh AS, Pavurala R, Gou E. Brain metastasis in a young patient: Consider the rectum. Cureus. 2021;13(11):e20055. 15. Chuah YY, Tashi T, Lee YY, Fu TY, Shih CA. Enteropathy-associated T-cell lymphoma (EATL) with intracranial metastasis: A rare and dismal condition. Acta Gastroenterol Belg. 2020;83(1):77–80. 16. Defillo A, Zelensky A, Simmons BH, Nussbaum ES. Supratentorial metastatic enteropathy-associated T-cell lymphoma: A case report and literature review. Surg Neurol Int. 2012;3:144. 17. Gobbi C, Buess M, Probst A, et al. Enteropathy-associated T-cell lymphoma with initial manifestation in the CNS. Neurology. 2003;60(10):1718–9. 18. Tutt AN, Brada M, Sampson SA. Enteropathy associated T cell lymphoma presenting as an isolated CNS lymphoma three years after diagnosis of coeliac disease: T cell receptor polymerase chain reaction studies failed to show the original enteropathy to be a clonal disorder. Gut. 1997;40(6):801–3. 19. Shams PN, Waldman A, Dogan A, MacKenzie JM, Plant GT. Ataxia in the setting of complicated enteropathy: Double jeopardy. J Neurol Neurosurg Psychiatry. 2002;72(4):527–9. 20. Berman EL, Zauber NP, Rickert RR, Diss TC, Isaacson PG. Enteropathy-associated T cell lymphoma with brain involvement. J Clin Gastroenterol. 1998;26(4):337–41.
Comments (0)