
Remember me


Breast cancer (BC) is the most prevalent and lethal malignancy in women, with a growing global incidence. In Portugal, approximately 7,000 patients are diagnosed with BC each year, resulting in 1,800 annual deaths.1 Although most patients present with localized disease, nearly 30% will eventually develop metastatic lesions, often months or years later. Metastasis can occur in different locations, with the most affected sites being the bone, lung, liver, and brain.2 Gastrointestinal (GI) tract metastases are detected in less than 5% of patients with BC, and simultaneous gastric and colonic metastasis is extremely rare.3
CASE REPORTA 59-year-old woman with no relevant medical history had a suspicious nodule in her right breast identified in a screening mammography. A core needle biopsy identified an invasive lobular carcinoma. She underwent quadrantectomy plus axillary lymph node dissection. The pathology report confirmed a 2 × 1.2 × 1.4 cm invasive lobular carcinoma, with metastasis in 9 of 16 axillary lymph nodes and no evidence of neurovascular invasion. Immunohistochemistry tests revealed a positive estrogen receptor status and negative progesterone and human epidermal growth factor receptor-type 2 receptor status. Computed tomography scans of the thorax, abdomen, and pelvis and bone scintigraphy showed no signs of metastatic disease. The patient received adjuvant chemotherapy (doxorubicin 60 mg/m2 plus cyclophosphamide 600 mg/m2, discontinued after 3 cycles because of hematological intolerance), followed by radiotherapy and hormonotherapy (letrozole 2.5 mg daily). She maintained regular follow-up visits.
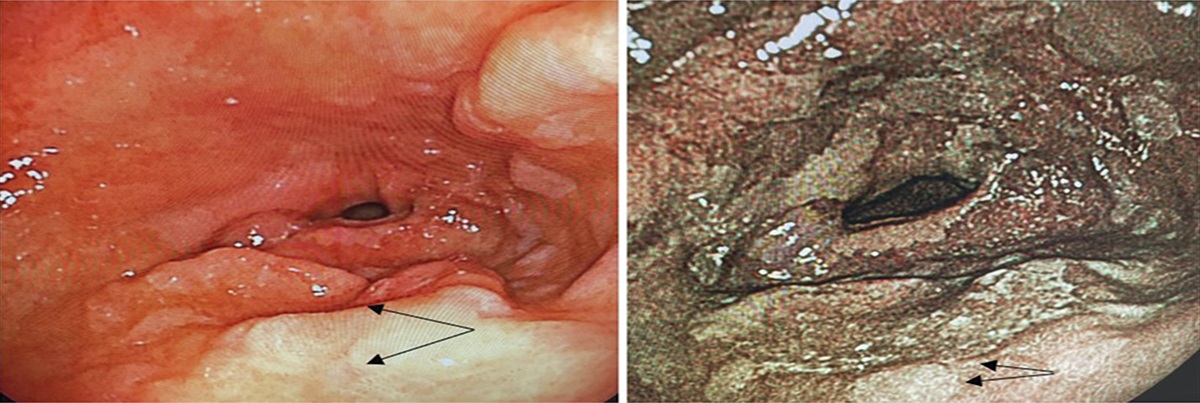
Around 2 years later, routine blood tests detected an increase in CEA levels from 2.5 to 17.5 ng/mL, prompting further investigation. Other serum markers, namely carbohydrate antigen (CA) 19-9 and CA 15-3, were within normal range, and the patient was asymptomatic. There were no signs of relapse on breast ultrasound and radiography. Computed tomography scans of the thorax, abdomen, and pelvis and bone scintigraphy revealed multiple bone lesions suggestive of metastatic lesions in the dorsolumbar spine and sacroiliac bones. Esophagogastroduodenoscopy showed thickened gastric folds in the fundus and corpus and 2 ulcers measuring 8–9 mm with a clean base and regular borders at the greater curvature in the fundus-corpus transition, which were biopsied (Figure 1). Colonoscopy showed a region of mucosal irregularity with erosions adjacent to the ileocecal valve, which was also biopsied (Figure 1). The histopathology report revealed a gastric and colonic carcinoma with suspected breast origin on immunohistochemical study (Figure 2). Both tissue samples presented a CK7-positive and CK20-negative pattern. The gastric sample was positive for GATA-binding factor 3 (GATA3) and negative for Caudal Type Homeobox 2 (CDX2). The colonic sample was positive for GATA3 and negative for SATB Homeobox 2 (SATB2). Both samples were negative for hormonal and human epidermal growth factor receptor-type 2 receptors. The patient was initially started on chemotherapy (fulvestrant 500 mg monthly plus palbociclib 125 mg daily), but it was discontinued 3 months later because of hepatic toxicity. There was a rapid clinical deterioration because of disease progression, and the patient required hospitalization with best supportive care until her death, which occurred approximately 6 months after the initial recurrence suspicion.
 Figure 1.:
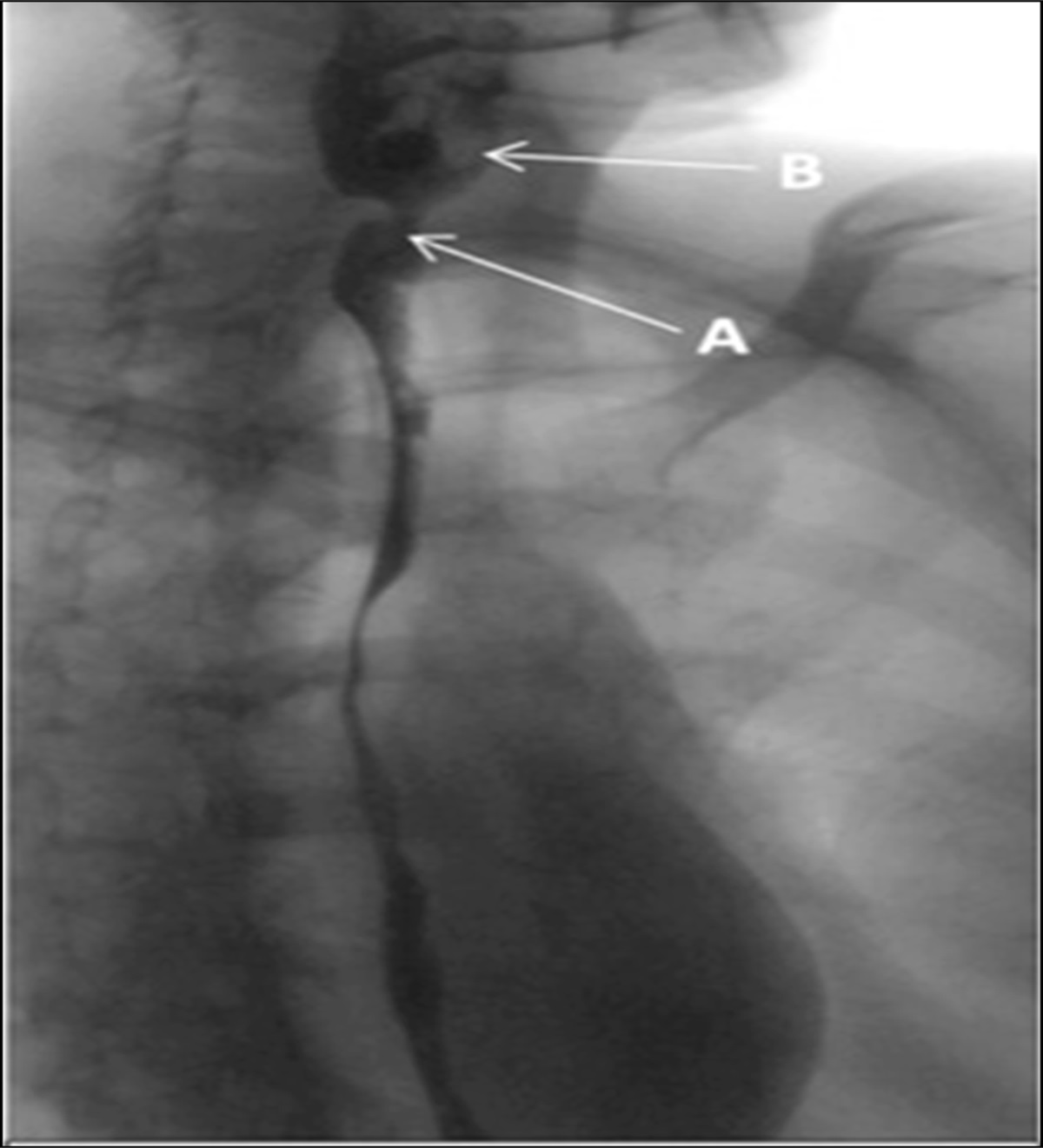
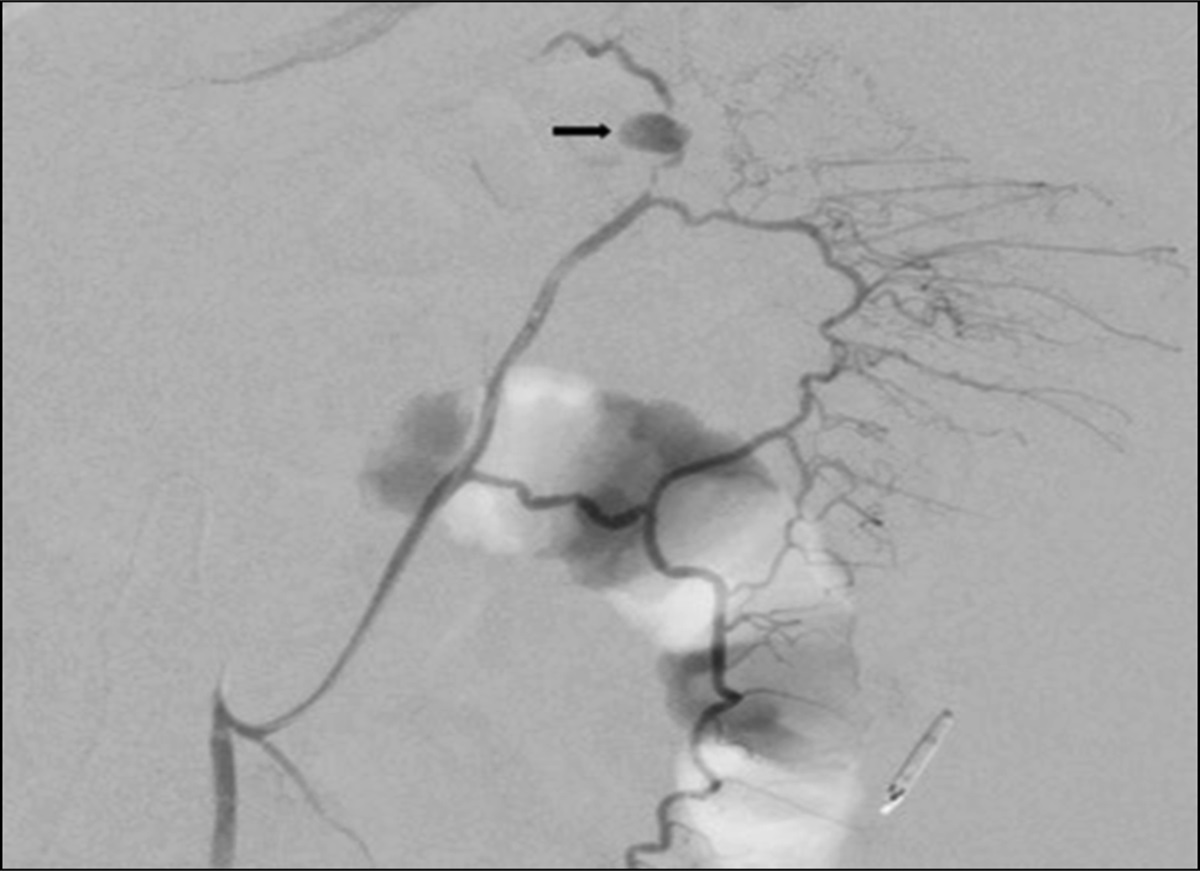
Figure 1.: Endoscopic findings. (A) Upper gastrointestinal endoscopy revealed thickened gastric folds and an ulcer with a clean base and regular borders at the fundus-corpus transition at the greater curvature. (B) Colonoscopy with an area of mucosal irregularity and small erosions adjacent to the ileocecal valve.
 Figure 2.:
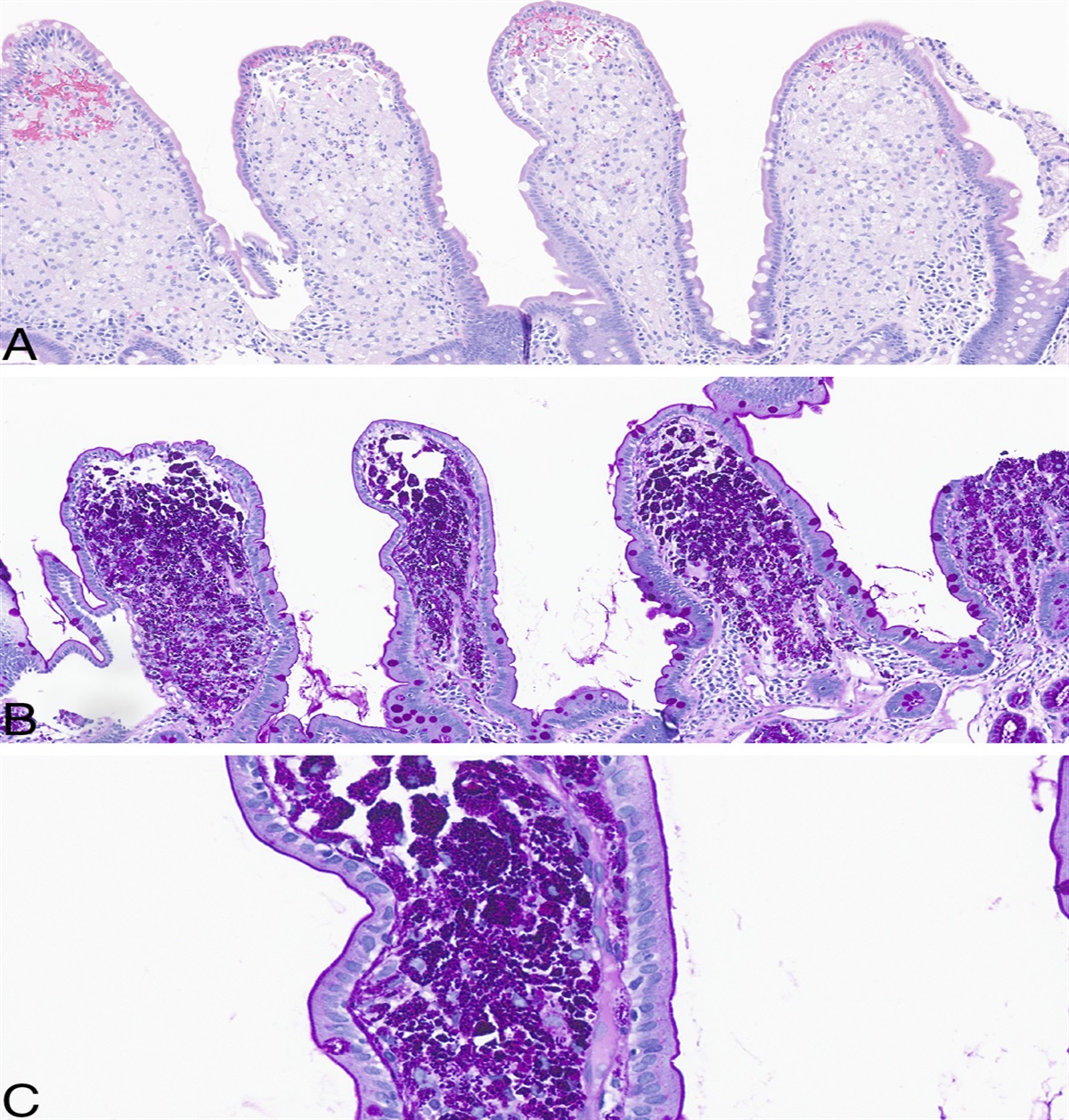
Figure 2.: Histopathology. (Biopsy A) Colonic mucosa expanded by neoplastic infiltration, within the lamina propria, composed of dispersed cells with ill-defined limits, eosinophilic cytoplasm, and round-to-oval hyperchromatic nuclei (arrows); immunohistochemical study showed positivity for cytokeratin (CK) 7 and GATA-3; CK20 and SATB Homeobox 2 were negative, which favors a mammary gland origin. (Biopsy B) Pyloric mucosa expanded by neoplastic infiltration morphologically identical to that described in the colon; immunohistochemical study showed positivity for pancytokeratin AE1/AE3 and GATA-3. GATA3, GATA-binding factor 3.
DISCUSSIONDuctal subtype represents the majority (around 80%) of invasive BC while the lobular subtype accounts for only 5%–15%.4 However, lobular BC is responsible for around 64% of GI tract metastasis.5 The reason for this discrepancy is poorly understood. Some authors suggest a particular tropism of lobular cells for these organs, possibly related to the loss of E-cadherin expression.6 Metastasis to the GI tract is a multifactorial process involving specific cytokines, leading to increased inflammation, tumor cell migration, and chemotaxis to these organs. The relationship between Helicobacter pylori colonization and gastric metastasis is still unproven.7
After malignant melanoma, BC is the second most common malignancy to metastasize to the GI tract. Nevertheless, simultaneous gastric and colonic BC metastasis is extremely rare, with only 7 cases reported in the literature.8–14
The diagnosis of GI tract metastasis can be challenging and requires a high index of clinical suspicion. Symptoms are usually nonspecific and can arise after a long disease-free period, be misdiagnosed as treatment-related adverse effects, or even be absent.7 Serum markers, such as CEA and CA 15-3, are not specific for GI tract metastasis.3 An interesting case report described an increase in CA 19-9 as the sole evidence of intestinal metastasis, but this finding has not been consistently reproduced in other studies.15
Endoscopic features of BC metastasis vary significantly and may include ulcers, mucosal thickening, mucosal friability, linitis plastica-like inflammation, polyps, strictures, or obstructing masses.16 Given the broad spectrum of presentation, gastroenterologists performing endoscopic procedures in patients with a known history of BC, particularly of the lobular subtype, should remain vigilant for the possibility of metastatic disease and consider biopsy of any suspicious endoscopically visible lesion.
Tissue sampling and immunohistochemistry are crucial to confirm the diagnosis. The expression of cytokeratins (CK) 7 and 20 is often used to determine the primary origin of the metastatic cancer. A CK7-positive and CK20-negative pattern is usually found in the lung, breast, thyroid, salivary gland, and female genital tract organs.17 GATA3, along with gross cystic disease fluid protein-15 and mammaglobin, has a sensitivity of 90% in determining BC as the primary origin of metastatic cancer. Hormonal receptors, specifically estrogen receptors, have lower sensitivity and specificity rates in the setting of metastatic BC and may not match the primary tumor pathology, as seen in our case.18 One hypothesis is that systemic therapies, such as hormonal therapy, can influence the emergence of different subpopulations of heterogeneous clones.19 In gastric samples, the CDX2 marker suggests a primary gastric origin while the SATB2 marker suggests a primary colonic origin in colonic samples.20 Therefore, CK7+/CK20−, GATA3+/CDX2−, and GATA3+/SATB2− profiles are suggestive of BC metastasis. Accurate histopathological diagnosis is critical because treatment options for primary GI carcinoma and metastatic BC differ significantly.
In conclusion, this case report highlights the importance of close surveillance after BC diagnosis and the need for a comprehensive GI tract evaluation in cases of suspected recurrence due to imaging, laboratory test, or clinical manifestations. Given the prevalence of BC, it is essential for gastroenterologists to be aware of potential GI metastasis, particularly in women with a history of invasive lobular carcinoma. All endoscopically visible lesions should be biopsied and evaluated by an expert pathologist.
DISCLOSURESAuthor contributions: I. Botto is the guarantor of the article. I. Botto and RM Cruz were responsible for writing the manuscript. All authors approved the final version of the article, including the authorship list.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Cancro da mama. Liga Portuguesa Contra O Cancro (https://www.ligacontracancro.pt./cancro-da-mama/). Accessed February 1, 2023. 2. Redig AJ, McAllister SS. Breast cancer as a systemic disease: A view of metastasis. J Intern Med. 2013;274(2):113–26. 3. Bolzacchini E, Nigro O, Inversini D, Giordano M, Maconi G. Intestinal metastasis from breast cancer: Presentation, treatment and survival from a systematic literature review. World J Clin Oncol. 2021;12(5):382–92. 4. Gainer SM, Lodhi AK, Bhattacharyya A, Krishnamurthy S, Kuerer HM, Lucci A. Invasive lobular carcinoma predicts micrometastasis in breast cancer. J Surg Res. 2012;177(1):93–6. 5. McLemore EC, Pockaj BA, Reynolds C, et al. Breast cancer: Presentation and intervention in women with gastrointestinal metastasis and carcinomatosis. Ann Surg Oncol. 2005;12(11):886–94. 6. Moll R, Mitze M, Frixen UH, Birchmeier W. Differential loss of E-cadherin expression in infiltrating ductal and lobular breast carcinomas. Am J Pathol. 1993;143(6):1731–42. 7. José Carlos Villa Guzmán JC, Espinosa J, Cervera R, Delgado M, Patón R, Cordero JM. Gastric and colon metastasis from breast cancer: Case report, review of the literature, and possible underlying mechanisms. Breast Cancer (Dove Med Press). 2016;9:1–7. 8. Critchley AC, Harvey J, Carr M, Iwuchukwu O. Synchronous gastric and colonic metastases of invasive lobular breast carcinoma: Case report and review of the literature. Ann R Coll Surg Engl. 2011;93(5):e49–e50. 9. Horimoto Y, Hirashima T, Arakawa A, Miura H, Saito M. Metastatic colonic and gastric polyps from breast cancer resembling hyperplastic polyps. Surg Case Rep. 2018;4(1):23. 10. Kobayashi M, Tashima T, Nagata K, Sakuramoto S, Osaki A, Ryozawa S. Colorectal and gastric metastases from lobular breast cancer that resembled superficial neoplastic lesions. Clin J Gastroenterol. 2021;14(1):103–8. 11. Yu H, Kim E, Seo MJ, et al. Stomach and colon metastasis from breast cancer. Ewha Med J. 2014;37(2):98–104. 12. Savanis G, Simatos G, Tzaida O, et al. Gastrointestinal tract metastasis as first presentation of breast cancer. J BUON. 2006;11(1):79–81. 13. Malhotra A, Guturu P, Basim MS, Raju GS. A rare case of breast cancer metastasis presenting as linitis plastica of the stomach and colon (with videos). Gastroint Endosc. 2009;70(3):552–3. 14. Takeuchi H, Hiroshige S, Yoshikawa Y, Kusumoto T, Muto Y. A case of synchronous metastasis of breast cancer to stomach and colon. Anticancer Res. 2012;32(9):4051–5. 15. Santini D, Altomare A, Vincenzi B, et al. An increase of CA 19.9 as the first clinical sign of ileocecal valve metastasis from breast cancer. In Vivo. 2006;20(1):165–8. 16. Zhang B, Copur-Dahi N, Kalmaz D, Boland BS. Gastrointestinal manifestations of breast cancer metastasis. Dig Dis Sci. 2014;59(9):2344–6. 17. Dum D, Menz A, Völkel C, et al. Cytokeratin 7 and cytokeratin 20 expression in cancer: A tissue microarray study on 15,424 cancers. Exp Mol Pathol. 2022;126:104762. 18. Gown AM, Fulton RS, Kandalaft PL. Markers of metastatic carcinoma of breast origin. Histopathology. 2016;68(1):86–95. 19. Macfarlane R, Seal M, Speers C, et al. Molecular alterations between the primary breast cancer and the subsequent locoregional/metastatic tumor. Oncologist. 2012;17(2):172–8. 20. Wong HH, Chu P. Immunohistochemical features of the gastrointestinal tract tumors. J Gastrointest Oncol. 2012;3(3):262–84.
Comments (0)