
Remember me


Intraductal papillary mucinous neoplasm (IPMN) is a premalignant lesion defined as a grossly visible, predominantly papillary noninvasive mucin-producing epithelial neoplasm arising in the main pancreatic duct or branch duct.1 One of its possible manifestations is acute pancreatitis. The prevalence of acute pancreatitis or recurrent acute pancreatitis (RAP) caused by IPMN varies and ranges from 12% to 67%.2 More specifically, the intestinal and pancreaticobiliary subtypes of IPMN were more closely associated with acute pancreatitis.3 A higher pancreatic volume, based on computed tomography scans, in patients with IPMN was also associated with higher frequency of acute pancreatitis.3
IPMN usually presents as dilated main pancreatic duct (MPD), cystic lesions with septations, calcifications, or mural nodules on imaging tests.4 Most patients would typically have findings on computed tomography scan, magnetic resonance cholangiopancreatography, or endoscopic ultrasound. However, in this case report, significant findings to diagnose IPMN were initially absent. The diagnosis was performed by direct visualization with peroral pancreatoscopy. We discuss the case of a 49-year-old woman presenting with recurrent acute pancreatitis caused by IPMN with high-grade dysplasia.
CASE REPORTA 49-year-old nonsmoker, nondrinker woman presented with recurrent abdominal pain. She has been admitted at 4 different hospitals in the span of 3 years because of recurrent acute pancreatitis with an unknown cause. She was then referred to our hospital for further evaluation.
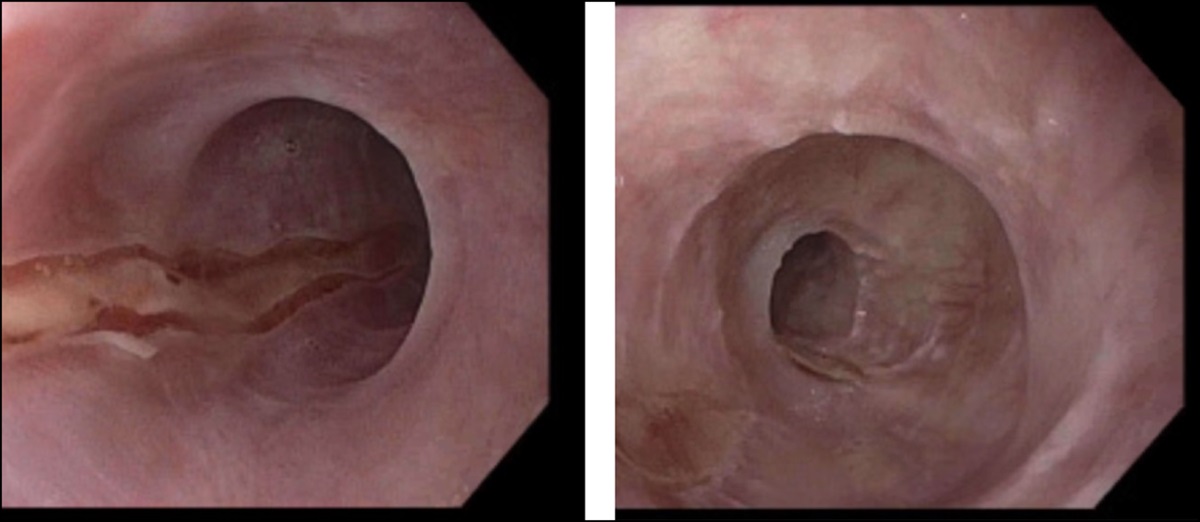
Initial magnetic resonance cholangiopancreatography was unremarkable (Figure 1). Carbohydrate antigen 19-9 was also normal. After 2 months, the patient again had another episode of acute pancreatitis. CT scan then showed a dilated main pancreatic duct of approximately 5 mm (Figure 1). After resolution of acute pancreatitis, an endoscopic retrograde cholangiopancreatography (ERCP) and intraductal ultrasound were performed to further evaluate the cause of MPD dilation and rule out malignancy. ERCP did not show any lesions (Figure 2). Pancreatic juice cytology only showed chronic inflammation.
 Figure 1.:
Figure 1.: (A) Initial magnetic resonance cholangiopancreatography did not show any significant lesions. (B) Computed tomography scan showing a slightly dilated main pancreatic duct without any stones, mass, or cystic lesions.
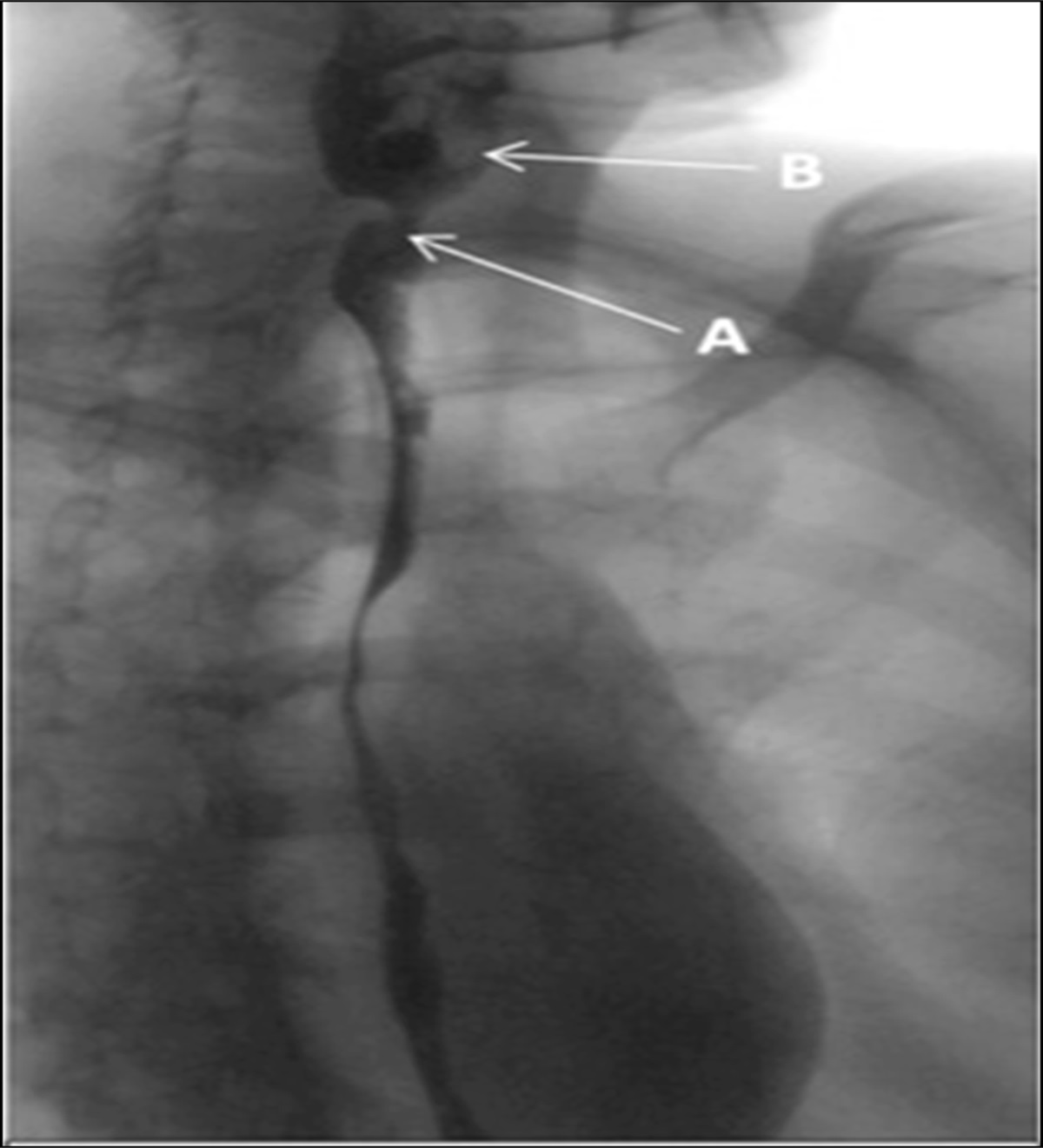
 Figure 2.:
Figure 2.: Endoscopic retrograde cholangiopancreatography fluoroscopy did not show any tumors or cystic lesions.
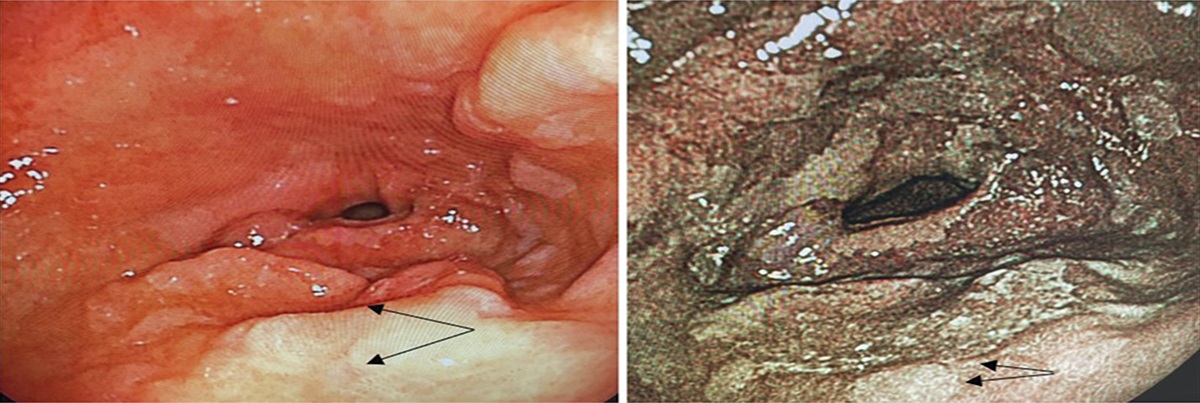
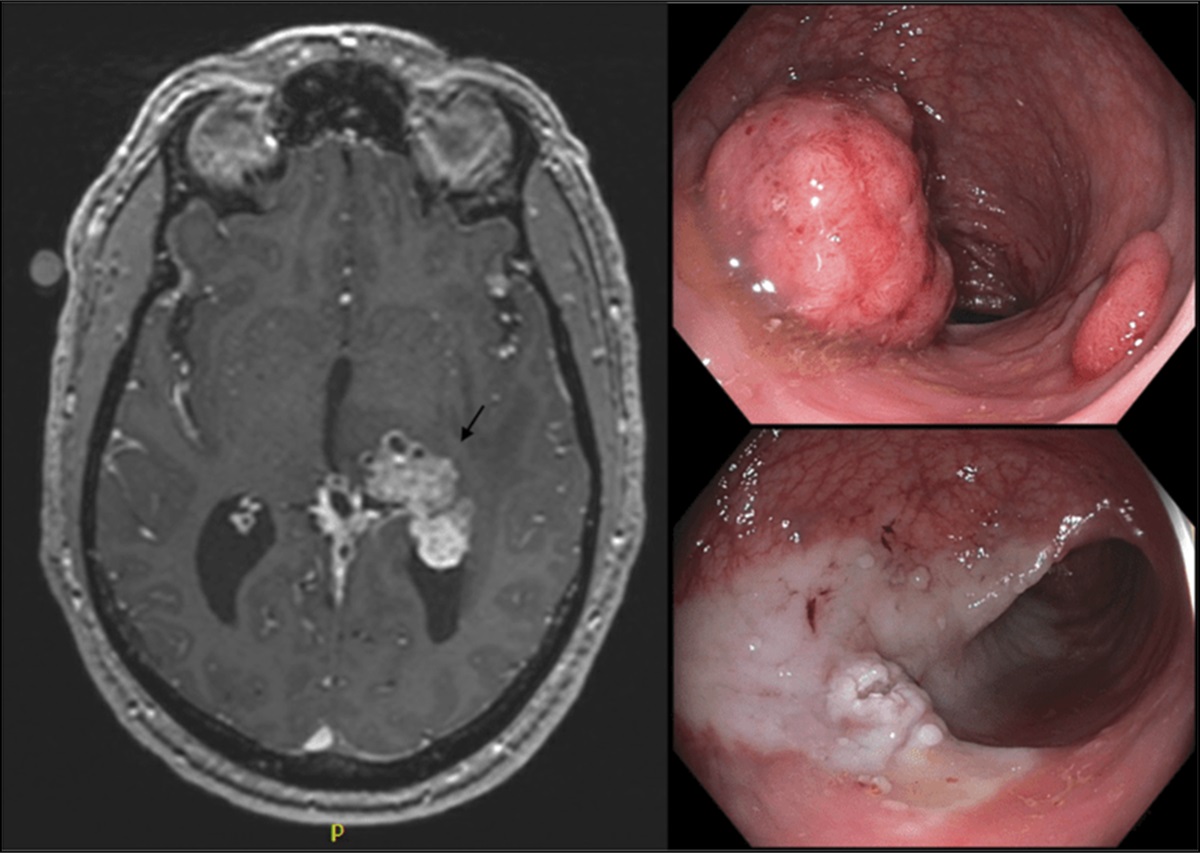
Five months after initial consultation, the patient still had intermittent, mild epigastric pain. Follow-up blood tests only showed mild elevation of transaminases less than 2 times the upper limit of normal. Bilirubin, amylase, lipase, and carbohydrate antigen 19-9 were within the normal range. Dupan-2 and Span-1, which are also tumor markers for pancreatic cancer, were normal. An esophagogastroduodenoscopy was performed, which did not show any other lesions that could cause abdominal pain. However, the papilla was noted to be patulous with clear mucoid secretion, a typical finding in patients with IPMN (Figure 3). Endoscopic ultrasound (EUS) also did not show any ampullary or pancreatic tumor (Figure 4). Owing to increasing MPD dilation in the repeat CT scan and new endoscopic finding of patulous ampulla, a repeat ERCP with peroral pancreatoscopy using SpyGlass DS Ⅱ (Boston Scientific, Tokyo, Japan) to evaluate the main-duct IPMN (MD-IPMN) showed intraductal papillary tumor at the pancreatic head (Figure 5). No other lesions were seen aside from the one in the pancreatic head during POPS. Biopsy results showed IPMN wherein there were some changes positively leading to malignancy.
 Figure 3.:
Figure 3.: Esophagogastroduodenoscopy showed the typical appearance of mucin-extruding patulous ampulla in patients with intraductal papillary mucinous neoplasm.
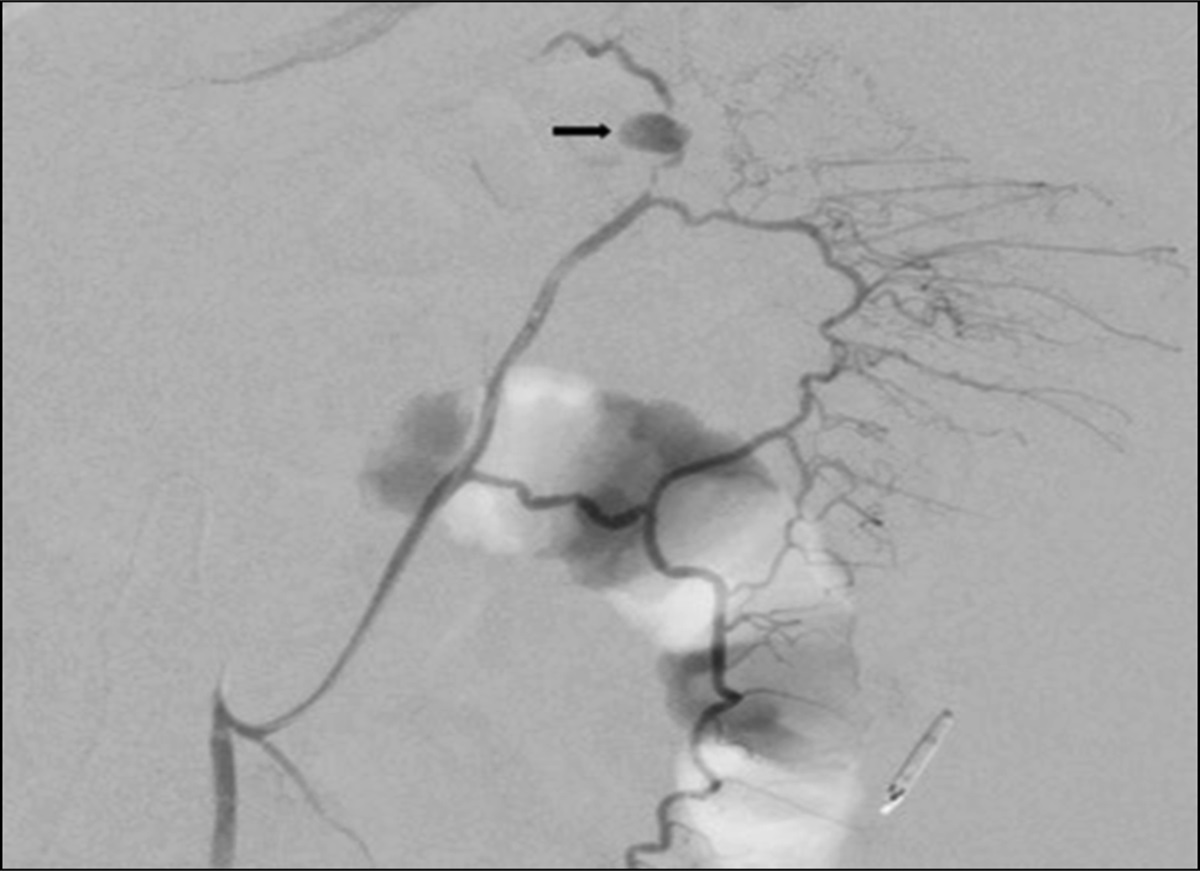
 Figure 4.:
Figure 4.: Endoscopic ultrasound showed a diffusely dilated main pancreatic duct measuring 5 mm. No mass or cystic lesions.
 Figure 5.:
Figure 5.: Endoscopic retrograde cholangiopancreatography and SpyGlass. (A) Main pancreatic duct dilatation shown in fluoroscopy. (B) Pancreatoscopy showed papillary changes in the pancreatic head area.
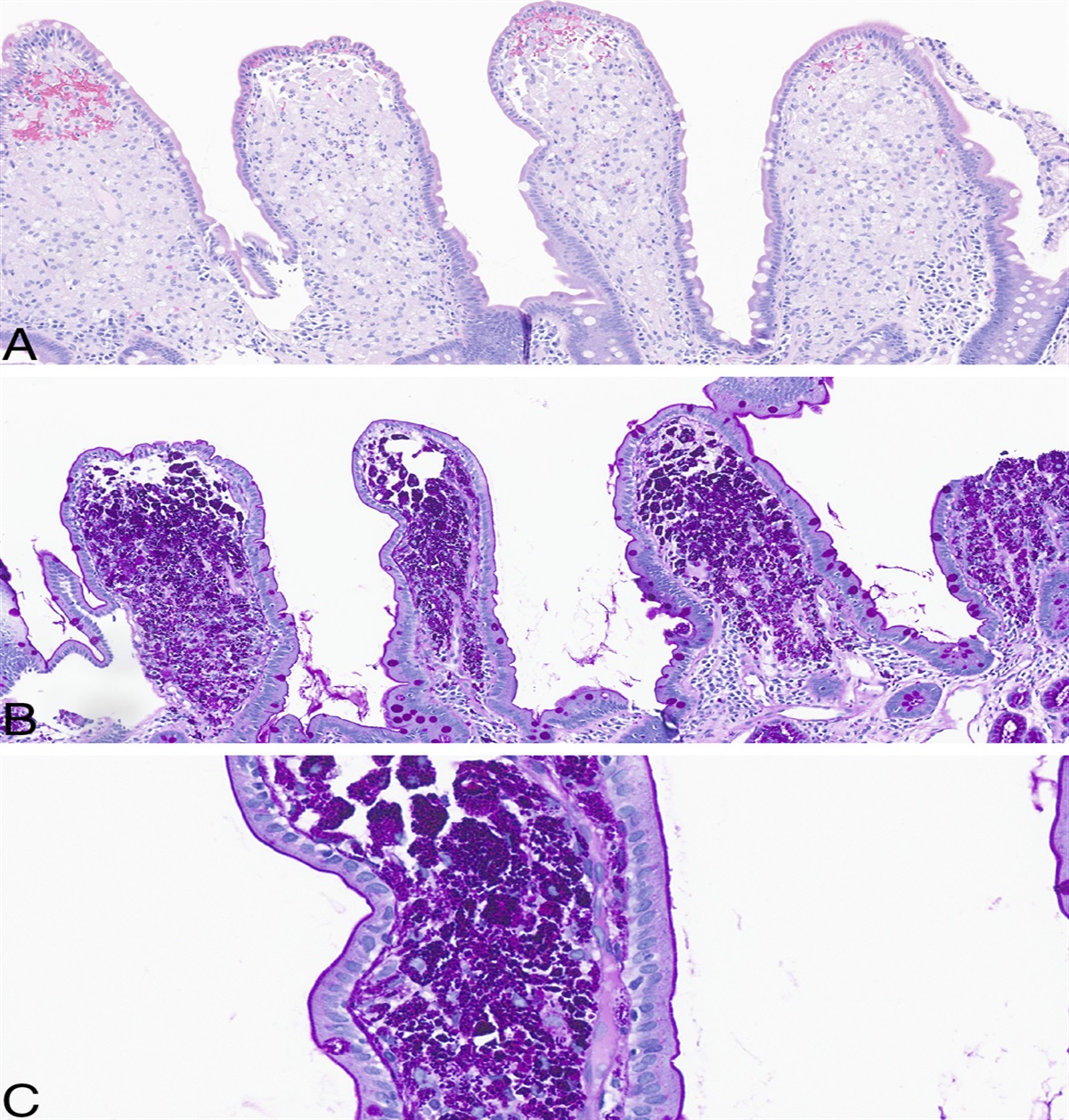
Owing to the positive biopsy results, the patient underwent pylorus-preserving pancreaticoduodenectomy (PPPD). A gross uncut specimen did not show any mass or cystic lesions (Figure 6). When the specimen was examined, the main pancreatic duct was dilated and an intraductal papillary mass was found at the pancreatic head (Figure 6). Main and peripheral pancreatic ducts were filled up with mucus. Histologically, atypical cells proliferate mainly in the main pancreatic duct, forming papillary structures. Most of the atypical cells were adenomas, but some were highly atypical. Immunochemical staining was positive for CK19, CK20, MUC2, MUC5AC, and CDX2 and negative for MUC6 (Figure 6). The final diagnosis was intestinal-type IPMN with high-grade dysplasia. The postoperative course was uneventful. Six months have passed since the surgery, and there have been no recurrences or late complications to date.
 Figure 6.:
Figure 6.: Surgical specimen and histopathology. (A) The uncut specimen did not show any mass or cystic lesions. The main pancreatic duct is dilated. (B–D) In cut sections, the side branches are also slightly dilated and mucus-filled. An intraductal papillary mass was found at the pancreatic head. (E) On immunostaining, CK 19, CK 20, MUC2, MUC5AC, and CDX2 are positive, leading to an intestinal type of intraductal papillary mucinous neoplasm.
DISCUSSIONIPMN is often diagnosed by using different imaging techniques, such as CT scan, magnetic resonance cholangiopancreatography, and EUS.5 This patient did not have any high-risk stigmata on imaging tests that would indicate the need for surgical resection following the Fukuoka guidelines.6 However, it was only during POPS with biopsy wherein a possible malignancy was identified. The role of POPS in the diagnostic workup of IPMN still remains to be determined. For patients with uncertain diagnosis, POPS may be of value. Reported POPS sensitivity rates for IPMN ranged between 64 % and 100%, specificity rates between 75 % and 100%, and overall diagnostic accuracy between 87.5 % and 100%.7 Pancreatoscopic characteristic features of IPMN were intraductal papillary or villous projections and the presence of mucus.7 Aside from definitive diagnosis of IPMN, POPS is also helpful in determining the presence of high-grade dysplasia and invasive carcinoma. The visual classification system proposed by Hara et al allowed for discrimination of malignant from noninvasive IPMN with an accuracy of 88% for MD-IPMN and 67% for BD-IPMN.7 Pancreatoscopic findings that were more frequently observed in patients diagnosed with malignancy were coarse mucosa, friability, and tumor vessels.7 In addition, because there is direct visualization of the pancreatic duct mucosa, targeted biopsy of lesions can be performed for histopathological analysis. The single-operator cholangiopancreatography-guided targeted biopsy was attempted in 11 patients, and adequate tissue sampling for histologic examination was secured in 90.9%.8 The impact of POPS on clinical decision making showed that POPS findings altered the surgical approach in 13%–62% of patients.7 In this case report, the patient underwent POPS with targeted biopsy, which showed malignant findings and changed the treatment plan.
It must be noted that POPS has a 12% adverse event rate, with mild post-ERCP pancreatitis being the most common.7 Judicious use of POPS in the workup of IPMN should always be practiced bearing in mind its risks and benefits. In current clinical practice, the exact role of POPS in patients with RAP and IPMN remains to be determined.6
In conclusion, IPMN with high-grade dysplasia may be a cause of recurrent acute pancreatitis. This case report showed how the use of POPS aided in early diagnosis in patients with equivocal findings in other imaging tests. The role of direct visualization with POPS in patients with RAP or IPMN should be determined in future studies because it may alter the patient's prognosis. The procedures followed were in accordance with the Declaration of Helsinki of the World Medical Association.
DISCLOSURESAuthor contributions: All authors had substantial contributions to drafting, revising, and final approval of this case report.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Basturk O, Hong SM, Wood LD, et al. A revised classification system and recommendations from the Baltimore consensus meeting for neoplastic precursor lesions in the pancreas. Am J Surg Pathol 2015;39(12):1730–41. 2. Jang JW, Kim MH, Jeong SU, et al. Clinical characteristics of intraductal papillary mucinous neoplasm manifesting as acute pancreatitis or acute recurrent pancreatitis. J Gastroenterol Hepatol 2013;28(4):731–8. 3. Tanaka T, Masuda A, Sofue K, et al. Acute pancreatitis in intraductal papillary mucinous neoplasms correlates with pancreatic volume and epithelial subtypes. Pancreatology 2021;21(1):138–43. 4. Fouladi DF, Raman SP, Hruban RH, Fishman EK, Kawamoto S. Invasive intraductal papillary mucinous neoplasms: CT features of colloid carcinoma versus tubular adenocarcinoma of the pancreas. Am J Roentgenol 2020;214(5):1092–100. 5. Ringold DA, Shah RJ. Peroral pancreatoscopy in the diagnosis and management of intraductal papillary mucinous neoplasia and indeterminate pancreatic duct pathology. Gastrointest Endosc Clin North Am 2009;19(4):601–13. 6. Tanaka M, Fernández-del Castillo C, Kamisawa T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 2017;17(5):738–53. 7. de Jong DM, Stassen PMC, Groot Koerkamp B, et al. The role of pancreatoscopy in the diagnostic work-up of intraductal papillary mucinous neoplasms: A systematic review and meta-analysis. Endoscopy 2022;55(01):25–35. 8. Kurihara T. Diagnostic and therapeutic single-operator cholangiopancreatoscopy in biliopancreatic diseases: Prospective multicenter study in Japan. World J Gastroenterol 2016;22(5):1891.
Comments (0)