
Remember me


Primary eosinophilic gastrointestinal diseases (EGIDs) are a spectrum of rare disorders characterized by excess eosinophil infiltration in the gut. Eosinophilic gastroenteritis (EGE) is now separated into eosinophilic gastritis and eosinophilic duodenitis, with eosinophilic colitis (EC) considered distinct. The prevalence of EGE and EC is reported to be 5.1 and 2.1 in 100.000 persons, respectively, in the United States and may be even rarer in Asia.1 EGE with concurrent eosinophilic esophagitis is common in children, but rare in adults.2-4 While EC may develop simultaneously with EGE, there is only 1 case report that reported ileocolitis preceding EGE.5,6 First-line therapies for EGE are 6-food elimination diet or corticosteroids.7 Initiating oral methylprednisolone may be complicated by tuberculosis and hepatitis B virus reactivation.8–10 We present a case of a Vietnamese man demonstrating the natural history of EGIDs that began with colonic disease and later manifest with esophageal then duodenal disease, in an adult with tuberculosis and latent hepatitis B infection.
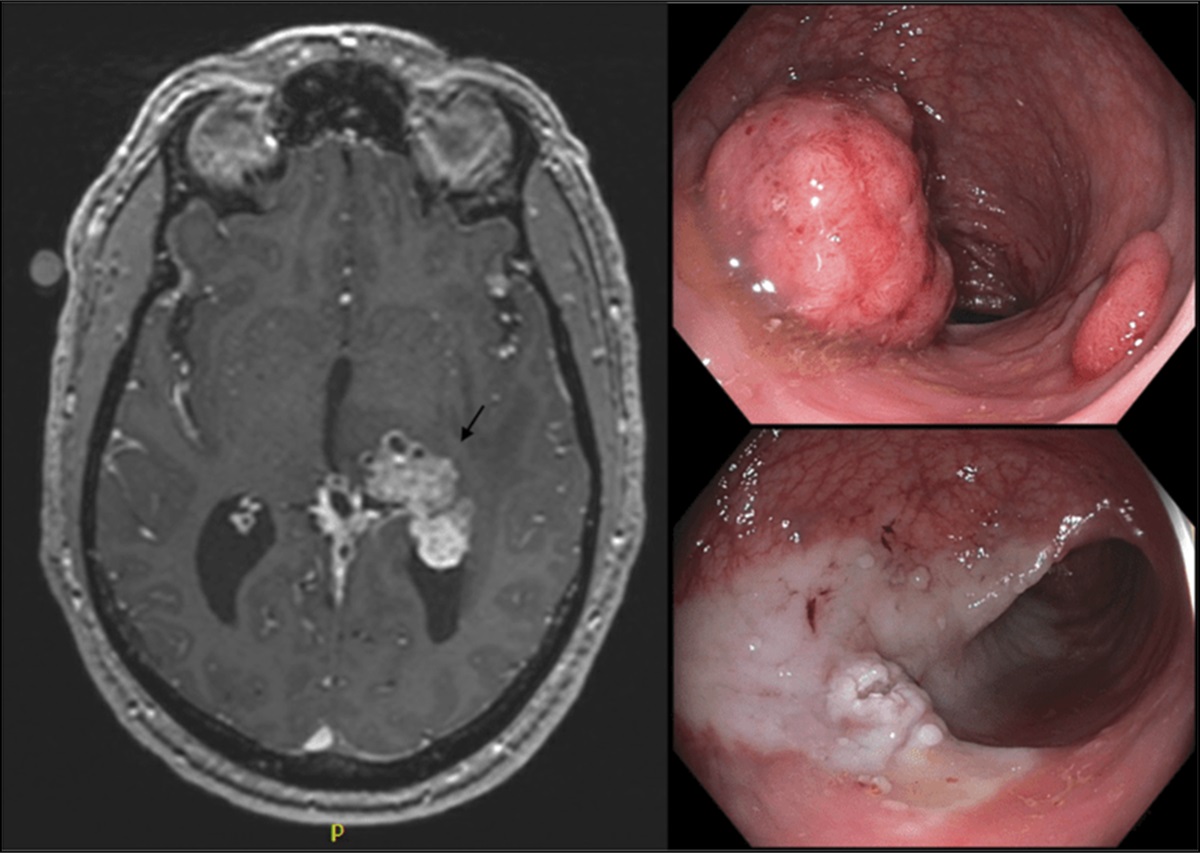
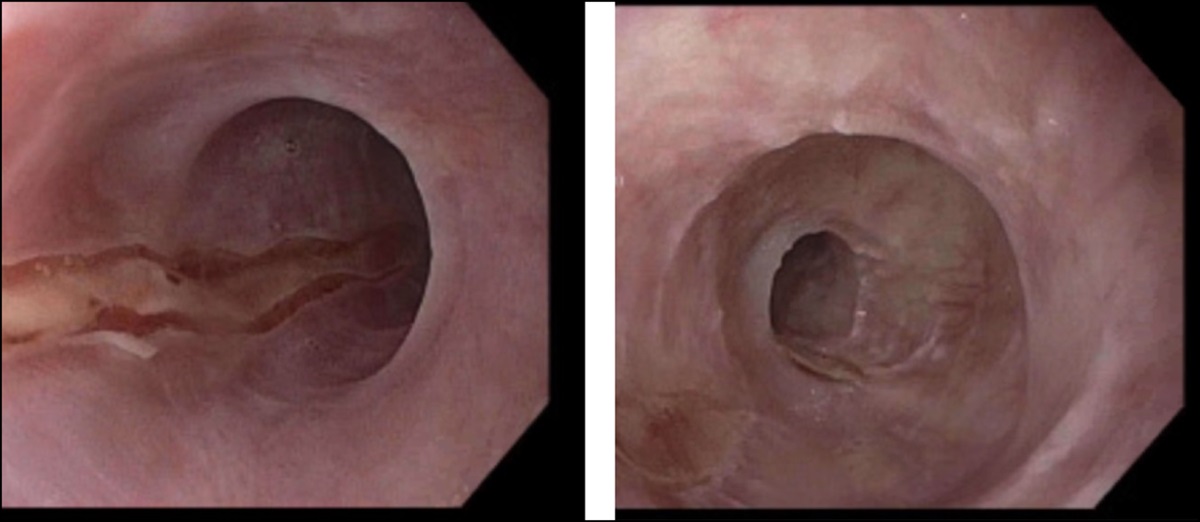
CASE REPORTA 59-year-old man presented with 3 days of abdominal cramps and watery diarrhea up to 10 times a day. Nine months earlier, he had presented with a 3-week history of similar symptoms of lesser severity. Colonoscopy showed a granular laterally spreading tumor in the ascending colon with a depressed area suspected of invasive adenocarcinoma (NBI International Colorectal Endoscopic Classification type 3). He underwent right colectomy, and his symptoms resolved. He had a history of sinusitis, and nasal polyps had been resected 7 months before the presentation. Two months before the presentation, dysphagia developed and an upper endoscopy revealed reflux esophagitis Los Angeles classification grade A. Dysphagia improved after a few days with esomeprazole 20 mg/d. There was no history of other allergies or atopy. There was a history of hypertension and dyslipidemia controlled by amlodipine, losartan, nebivolol, and atorvastatin. Physical examination was unremarkable.
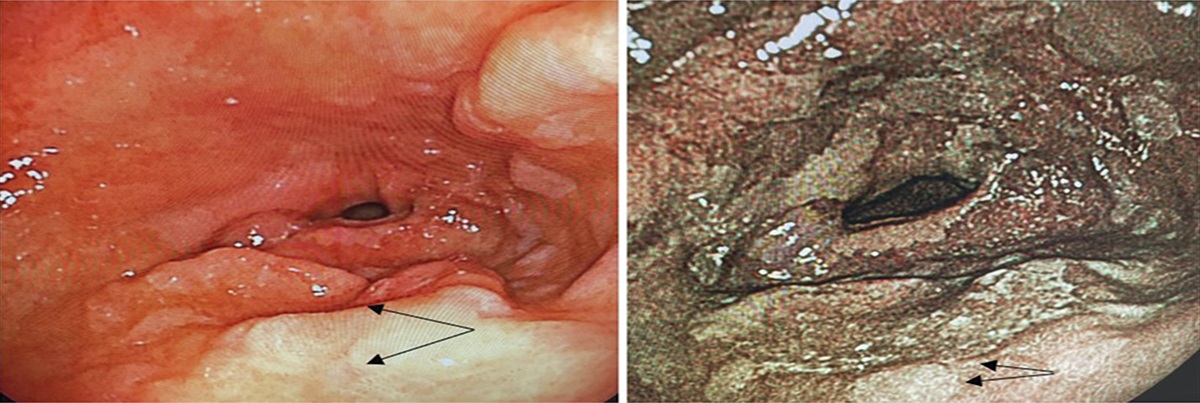
A 7-day course of ciprofloxacin and metronidazole for treatment of suspected acute gastroenteritis was given, with no improvement. Laboratory studies revealed variable peripheral eosinophilia over time and an elevated serum immunoglobulin E level of 315.6 IU/mL (normal: <130 IU/mL) (Figure 1). Infectious workup, including stool ova and parasite examination and serology tests for toxocara, Strongyloides stercoralis, and Schistosoma mansoni, was negative. Computed tomographic findings revealed ileal wall thickening (>4 mm) and mild ascites. Endoscopic findings included white papules, erosions, and erythema in the esophagus, duodenum, and ileum, respectively. Initial mucosal biopsies revealed excess eosinophil infiltration in the esophagus (maximum, 76 eosinophils per high power field [hpf]) and duodenum (64 eosinophils/hpf), but not in the ileum (Figure 2). Eight days later, additional biopsies from the ileum and colon showed eosinophilic ileitis (249 eosinophils/hpf) (Figure 3). Reviewing the previously resected colonic specimens showed a tubular adenoma with high-grade dysplasia (no carcinoma) but also a pathological excess of eosinophils in the mucosa, submucosa, muscularis propria, and serosa of the right colon (Figure 4). A review of the histology of the resected nasal polyps showed a typical edematous, eosinophilic type. He was referred to a tuberculosis specialist because the QuantiFERON-TB was positive. Sputum-negative pulmonary tuberculosis and mediastinal lymph node tuberculosis were diagnosed. He tested positive for anti-HBc, but was HBsAg-negative. Workup for vasculitis was negative.
 Figure 1.:
Figure 1.: Blood eosinophil count over a 9-month period. The dotted line represents an eosinophil count of 500/μL. EGE, eosinophilic gastroenteritis.
 Figure 2.:
Figure 2.: Mucosal biopsies show (A) 76 intraepithelial eosinophils per high-power field (hpf) in the esophagus and (B) 64 eosinophils/hpf in the lamina propria of the duodenum (hematoxylin-eosin [H&E] stain, magnification ×40).
 Figure 3.:
Figure 3.: Ileum biopsy, with sheets of 249 eosinophils/hpf in the lamina propria and numerous eosinophils in the crypt epithelium (11 eosinophils/hpf) (H&E stain, ×40). H&E, hematoxylin-eosin; hpf, high-power field.
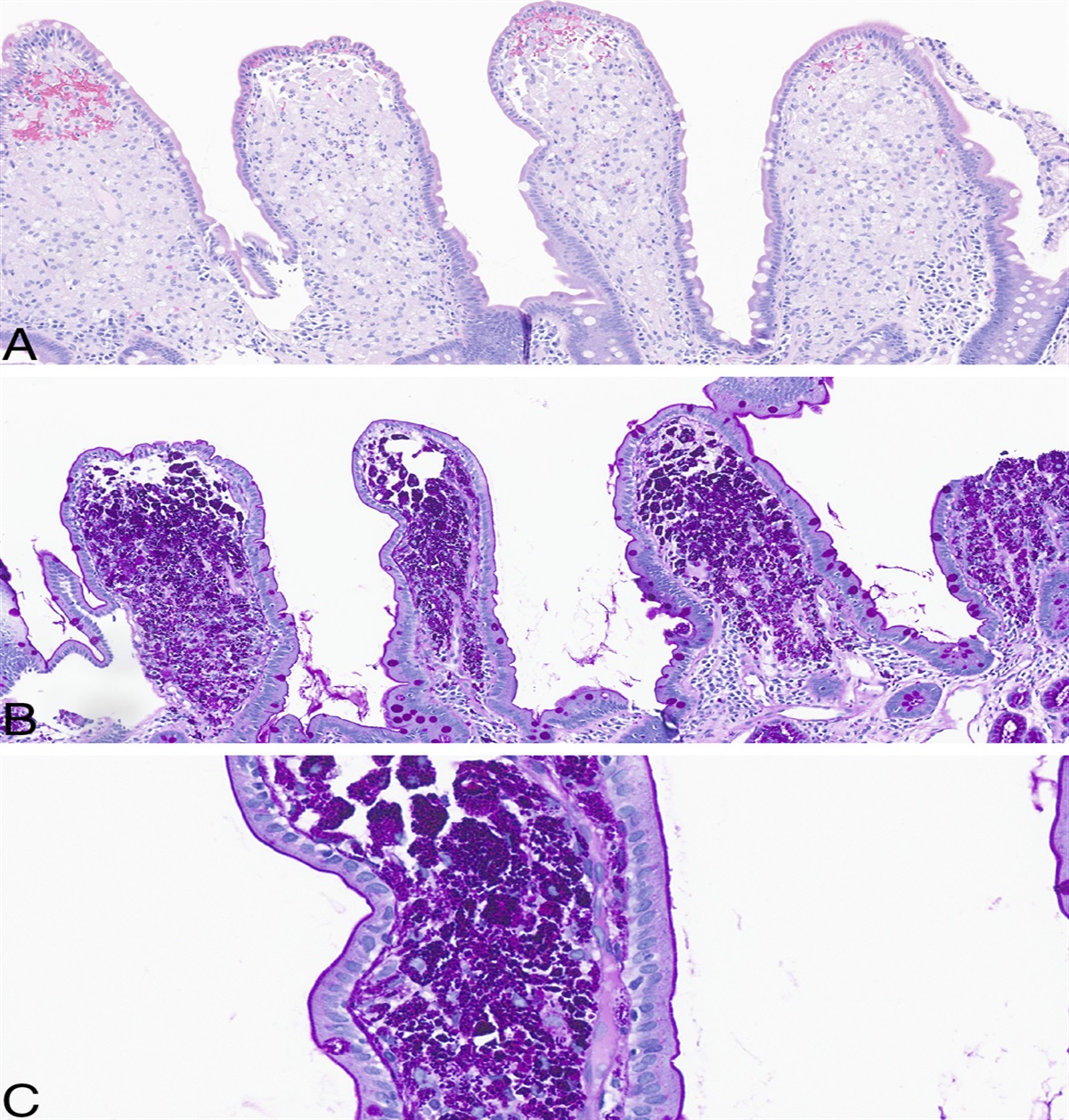
 Figure 4.:
Figure 4.: A review of resected tumor specimens in the right colon, with sheets of 85 eosinophils/hpf in the lamina propria (A) and altered eosinophil distribution including 25 eosinophils/hpf in the crypt epithelium (A) and 15 eosinophils/hpf in the surface epithelium (B) (H&E stain, ×40). There was eosinophilic inflammation in the mucosa, submucosa, muscularis propria, and serosa (C and D) (H&E stain, ×10). H&E, hematoxylin-eosin; hpf, high-power field.
He received twice-daily albendazole 400 mg for 7 days, followed by an intensive phase with a 4-drug regimen of antituberculosis therapy for 1 month before corticosteroid treatment. After that, oral methylprednisolone 32 mg/d, tenofovir disoproxil fumarate 300 mg/d, and a 6-food elimination diet were initiated. There was only a partial response to steroids after 2 weeks of treatment with the pain intensity declining from 10 to 6 on a 0-10 numerical rating scale (0, no pain; 10, worst pain imaginable). Azathioprine 50 mg/d, ketotifen 1 mg/d, and montelukast 10 mg/d were added to methylprednisolone, and then, ketotifen was increased to 4 mg/d. He went into clinical remission in the third week of treatment. Methylprednisolone was slowly tapered and discontinued. After 6 weeks on the full 6-food elimination diet, each food was rechallenged biweekly. Egg and nuts triggered peripheral eosinophilia (>500/μL). Food reintroduction was discontinued, and add-on medications were successfully ceased. He was completely well at the 6-month follow-up.
DISCUSSIONA 3-day history of abdominal cramps and diarrhea led us to misdiagnose acute gastroenteritis. Peripheral eosinophilia was a clue to the definitive diagnosis.11 Nevertheless, it is not universal in EGE.12 Our case demonstrates that repeat biopsies should be undertaken if EGE is suspected because its pathology is often patchy.13 Twenty-five percent to 75% of EGE cases have a history of allergies and atopy, and this case had nasal polyps.14 Most notably, our review of resected tumor specimens revealed EC in addition to adenoma. Colon cancer may be associated with colonic eosinophilia.15 Importantly, he had resolution of not only symptoms but also peripheral eosinophilia after right colectomy, suggesting EC was the primary underlying cause of his symptoms at that time. The patient later presented with dysphagia. In the differential diagnosis is eosinophilic esophagitis that is often proton-pump inhibitor-responsive, as in this case, but esophageal biopsies were omitted as a diagnosis of esophagitis was made.16 The natural history of this case suggests EGIDs can develop into a clinicopathologic continuum that commences in the colon spreading clinically to the esophagus over time, likely related to food. In this case, there was clinical resolution and then resurgence of the EGID elsewhere.
An issue was the need to manage co-occurrent occult infections before prescribing systemic corticosteroids at moderate doses, especially because a major subgroup with EGE need longer term courses to control disease.7 First, albendazole was prescribed to treat any occult helminth infections, especially occult strongyloidiasis due to the risk of disseminated strongyloidiasis.17 Second, screening for latent tuberculosis infection led to a diagnosis of active tuberculosis. Previous studies have shown that patients with inflammatory bowel disease should be tested for tuberculosis before initiating immunosuppressant medications.8,9 Third, our case was classified into the high-risk group of hepatitis B reactivation, indicating that initiating antiviral prophylaxis was necessary.10
In summary, this case has some relatively unique features. We observed the spread of disease proximally from the right colon to the esophagus and duodenum clinically and pathologically. In highly endemic countries, recognition and treatment of occult helminthiasis and tuberculosis and prevention of hepatitis B reactivation are considerations before starting immunosuppressive therapy for EGIDs.
DISCLOSURESAuthor contributions: PV Nguyen wrote the manuscript. DT Quach and NJ Talley revised the manuscript. MHQ Bui and PV Nguyen analyzed biopsies. TP Dang performed endoscopies and biopsies. All authors critically reviewed the manuscript. PV Nguyen is the article guarantor.
Financial disclosure: none to report.
Informed consent was obtained for this case report.
REFERENCES 1. Mansoor E, Saleh MA, Cooper GS. Prevalence of eosinophilic gastroenteritis and colitis in a population-based study, from 2012 to 2017. Clin Gastroenterol Hepatol. 2017;15(11):1733–41. 2. Ko HM, Morotti RA, Yershov O, et al. Eosinophilic gastritis in children: Clinicopathological correlation, disease course, and response to therapy. Am J Gastroenterol. 2014;109(8):1277–85. 3. Dobbins JW, Sheahan DG, Behar J. Eosinophilic gastroenteritis with esophageal involvement. Gastroenterology. 1977;72(6):1312–6. 4. Netzer P, Gschossmann JM, Straumann A, et al. Corticosteroid-dependent eosinophilic oesophagitis: Azathioprine and 6-mercaptopurine can induce and maintain long-term remission. Eur J Gastroenterol Hepatol. 2007;19(10):865–9. 5. Turner KO, Sinkre RA, Neumann WL, et al. Primary colonic eosinophilia and eosinophilic colitis in adults. Am J Surg Pathol. 2017;41(2):225–33. 6. Haberkern CM, Christie DL, Haas JE. Eosinophilic gastroenteritis presenting as ileocolitis. Gastroenterology. 1978;74(5 Pt 1):896–9. 7. Walker MM, Potter M, Talley NJ. Eosinophilic gastroenteritis and other eosinophilic gut diseases distal to the oesophagus. Lancet Gastroenterol Hepatol. 2018;3(4):271–80. 8. Aberra FN, Stettler N, Brensinger C, et al. Risk for active tuberculosis in inflammatory bowel disease patients. Clin Gastroenterol Hepatol. 2007;5(9):1070–5. 9. Kumar N, Govil A, Puri AS, et al. Tuberculosis in ulcerative colitis: Bird in the bush. Trop Gastroenterol. 1994;15(4):219–21. 10. Perrillo RP, Gish R, Falck-Ytter YT. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology. 2015;148(1):221–44.e223. 11. Kovalszki A, Weller PF. Eosinophilia. Prim Care. 2016;43(4):607–17. 12. Talley NJ, Shorter RG, Phillips SF, et al. Eosinophilic gastroenteritis: A clinicopathological study of patients with disease of the mucosa, muscle layer, and subserosal tissues. Gut. 1990;31(1):54–8. 13. Collins MH. Histopathology associated with eosinophilic gastrointestinal diseases. Immunol Allergy Clin North Am. 2009;29(1):109–17. 14. Khan S. Eosinophilic gastroenteritis. Best Pract Res Clin Gastroenterol. 2005;19(2):177–98. 15. Khurana S, Abu-Sbeih H, Ma W, et al. Clinical characteristics and outcomes of eosinophilic colitis in patients with cancer. Am J Clin Oncol. 2021;44(8):395–401. 16. Collins MH. Histopathologic features of eosinophilic esophagitis and eosinophilic gastrointestinal diseases. Gastroenterol Clin North Am. 2014;43(2):257–68. 17. Jourdan PM, Lamberton PHL, Fenwick A, et al. Soil-transmitted helminth infections. Lancet. 2018;391(10117):252–65.
Comments (0)