The global scale-up of HPV vaccination, HPV-based screening, and treatment of precancerous lesions are the recommended interventions to curb the burden of cervical cancer worldwide. This particular review summarized the findings of articles containing information about the level of adolesent girls HPV vaccination uptake and mothers willingness to vaccinate thier children in Ethiopia.
In our review, the included studies reported the proportion of vaccination uptake between 44.1% [12] and 66.5% [13]. The pooled estimate of vaccination uptake of at least one dose of HPV vaccine among adolescents in Ethiopia was 55% (95%CI: 53–57), which is quite low and represents the wide gap that needs to be bridged before achieving the WHO strategy of having 90% of girls fully vaccinated by the age of 15 years in 2030 [6]. Our finding suggests that a significant proportion of adolescent girls remain largely unprotected [20, 21]. According to the WHO recommendation, the strategy to eliminate cervical cancer requires fully vaccinating 90% of girls by 15 years of age, screening 70% of women with a high-performance test by 35 years of age and again at 45 years of age, and 90% of women identified with cervical disease receiving treatment [6].
If HPV vaccination and cervical screening are scaled up, the annual cervical cancer incidence can be brought down by significant levels. HPV-based vaccination in Ethiopia was started in October 2018 for school girls. The available vaccine in the country is Gardasil-4, which targets HPV6, 11, 16, and 18 [22]. According to the information from WHO African region report, so far about 2 million girls aged 9–14 were vaccinated in the country [23]. The HPV vaccination is not part of the national immunization program in Ethiopia partly because of the cost of the vaccine. However, our review result showed that the uptake was low even if the vaccine was made available for the public for free. Using Gardasil-4, that doest target the most high-risk HPVs in Ethiopia [22], coupled with low vaccine acceptance will complicate the fight against CC in Ethiopia.
The level of HPV vaccination uptake in different African countries was also reported to be low. For example, a study in Nigeria showed that the level of knowledge of adolescent girls on HPV vaccines was low and the vaccination uptake was 2.1-4%. The most common reason given for not having taken the vaccine was unawareness of the vaccine [24, 25]. Similarly, a study in Uganda and Kenya showed that the vaccination uptake of adolescent girls was 17.61% [26] and 33% [27], respectively. Further, in a similar meta-analysis study on HPV vaccination uptake in low and middle-income countries, the pooled estimate of vaccination uptake of any dose was about 61% with a wide range of percentages of uptake reported from various countries in the period of 2006 to 2020 [28].
Another systematic review on the uptake of HPV vaccination among adolescent girls showed that the vaccination uptake rate for at least one dose varied significantly among countries, ranging from 2.4% in Hong Kong to 94.4% in Scotland [29]. Similarly, the HPV vaccination uptake of female students (age 9–12 years) from 31 primary schools in South Africa was reported to be 98% [30]. More than 90% HPV vaccination uptake was also reported among girls (9–15 years) in the Europian union [31].
The difference in the reports of the HPV vaccination uptake across these studies might be due to disparities in socioeconomic status, health information access, and tools used to measure the acceptance of HPV vaccination. Specifically, the higher vaccination uptake in the developed world might be because girls might have good accessibility to the HPV vaccine with all the necessary information.
The acceptance of the HPV vaccination in our review is low which might be due to poor health information access, less involvement of girls participating in health-related school clubs, and sociocultural influence on the female gender. In our review, the pooled estimate of the proportion of good knowledge about HPV vaccination and the agreement of adolescent girls to get the vaccine were 60% and 65%, respectively. These figures might be directly related to the low uptake of the vaccine. A review article in Sub-Saharan Africa also showed that there was a relatively higher level of willingness to get the HPV vaccine, but low levels of knowledge and awareness about the HPV vaccine was reported [32].
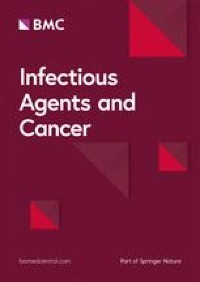
The influence of knowledge and perceptions of HPV vaccination suggests the importance of tailored health education on HPV immunization. Therefore, actions aimed at creating a positive attitude toward the HPV vaccine, sensitization of adolescents about the vaccine, and conducting community outreaches are timely areas of interventions that the stakeholders should consider. As social media outlets are becoming an increasing source of information in Ethiopia, using these platforms HPV related information, attitudes, and behavioral-related information can be easily made available to the people at large.
The United States, Australia, and Canada were the first countries to implement HPV vaccination as part of their national immunization programs since 2006 [24]. In contrast, most low- and middle-income countries started the HPV vaccination in 2018/19. Only about 31% of countries in the WHO AFRO region had begun vaccination as part of their national immunization program [24]. By the middle of 2020, 15 to 20% of adolescent girls took at least one dosage globally in terms of coverage. As a result, many girls who reside in nations that have not yet incorporated the HPV vaccine into their national immunization schedules are unprotected [20,21,22,23,24].
Our review also identified factors associated with HPV vaccination practice among adolescent girls. The included studies in our review reported different statistically significant predictors for the uptake of the HPV vaccine by girls. Positive attitudes to the vaccine, higher maternal education, and having knowledge about HPV and its vaccine were reported by two or more articles as important predictors to take the vaccine. On the contrary, not having adequate information about the vaccine and concerns about possible side effects were reported as reasons for not taking the vaccine. A similar study in Nigeria reported that The most common reason given for not having taken the vaccine was unawareness about the HPV vaccine (98%) [24, 25].
Proper strategies to overcome these barriers are needed to ensure successful vaccination uptake. There is no single solution to increase vaccination uptake and different approaches may be better suited to certain populations. Hence, it is suggested that barriers to the uptake of the vaccine should be addressed, and that school-based sexual health education of HPV infection and vaccine promotion should be practiced in Ethiopia [29]. A study in Nigeria reported that the perception of susceptibility to HPV infection by girls was significantly associated with acceptance of the vaccines [33].
A similar study in Latin America indicated that there were several reasons attributed to low vaccination uptake among adolescent girls: limited knowledge of HPV and HPV vaccine, misguided safety concerns, high cost, cultural barriers, and the COVID-19 pandemic [34]. There is an urgent need for more education to inform the public about HPV, cervical cancer, and the HPV vaccine, particularly to key parties, (adolescents and their parents), to leverage high levels of willingness and acceptability of the HPV vaccine toward successful implementation of HPV vaccination program in Ethiopia [35]. It is suggested that to increase the HPV vaccination uptake, strategies targeting adolescents/parents focussed on reminder-based regular announcements, education, information, and communication activities, and multicomponent approaches [35].
With regard to mothers‘ willingness to vaccinate their children, the pooled estimate of mothers who were willing to vaccinate their adolescent girls was 74%. Similar studies in Nigeria reported that 70-79.2% of mothers of adolescent girls demonstrated a willingness to vaccinate their daughters against HPV. Those mothers who were unwilling to vaccinate their adolescent girls reason out that it may encourage sexual promiscuity [33]. Likewise, parental HPV vaccine acceptance in Indonesia was 96.1%, which is higher than our report which may be because of the difference in socio-economic status of these people. But, the study demonstrated that knowledge about HPV and cervical cancer is low [36].
In our study, the pooled estimate of mothers who were knowledgeable about HPV vaccination and those who had a positive attitude to vaccinate their children were 38% and 58%, respectively. Similarly, in Nigeria, only 19.0% of mothers had good knowledge about cervical cancer prevention strategies [25]. Further, Jaspers et al., from Indonesia demonstrated that knowledge about HPV and cervical cancer is low among mothers of adolescent girls [36]. While the involvement of parents in the decision of their children to take the HPV vaccine [20, 21], the reported quite low knowledge and attitude towards vaccine need mitigating action.
For the HPV vaccination uptake barriers include parents‘ knowledge, perceptions, and attitudes toward the HPV infection [21]. In our review, parents having media exposure, having good knowledge about HPV infection, and positive attitude towards HPV vaccination were reported to be important predictors to vaccinate their adolescent girls. In contrast, a study reported about mothers‘ perceived reasons why they failed to vaccinate their girl and the important factors identified were the absence of information about HPV, their belief that the vaccine may affect their child‘s fertility, fear of side effects, and fear of needle injection [11]. A similar survey conducted to identify trends in the main reasons of parents of unvaccinated children in the United States showed that the top five most frequently cited reasons for not intending to vaccinate their children included “not necessary,” “safety concerns,” “lack of recommendation,” “lack of knowledge,” and “not sexually active.” Overall, parental HPV vaccine hesitancy decreased by 5.5% annually for some years [37]. Over time, more parents stated that they did not intend to vaccinate their adolescent children against HPV due to concerns about the vaccine safety [37].
It is reported that health education intervention was found to be effective at improving the parental willingness to vaccinate their adolescents with the HPV vaccine. A multipronged approach in educating the parents of adolescents about the benefit of the HPV vaccine in reducing and preventing the infection and its effects. Educated mothers might feel confident to vaccinate their daughters against HPV by retrieving medical information on the risks of contracting HPV infections [15].
Strength and limitations
To the best of our knowledge, this systematic review reported the latest summarized finding of HPV vaccination uptake and parental willingness to vaccinate adolescent girls in the Ethiopian context. However, our findings should be interpreted with caution due to some drawbacks; the studies were reported from only some regions of the country. The absence of data from the rest of the regions in the country might compromise our conclusion. The other snare of this review is the presence of high heterogeneity between the included articles.

Comments (0)