
Remember me
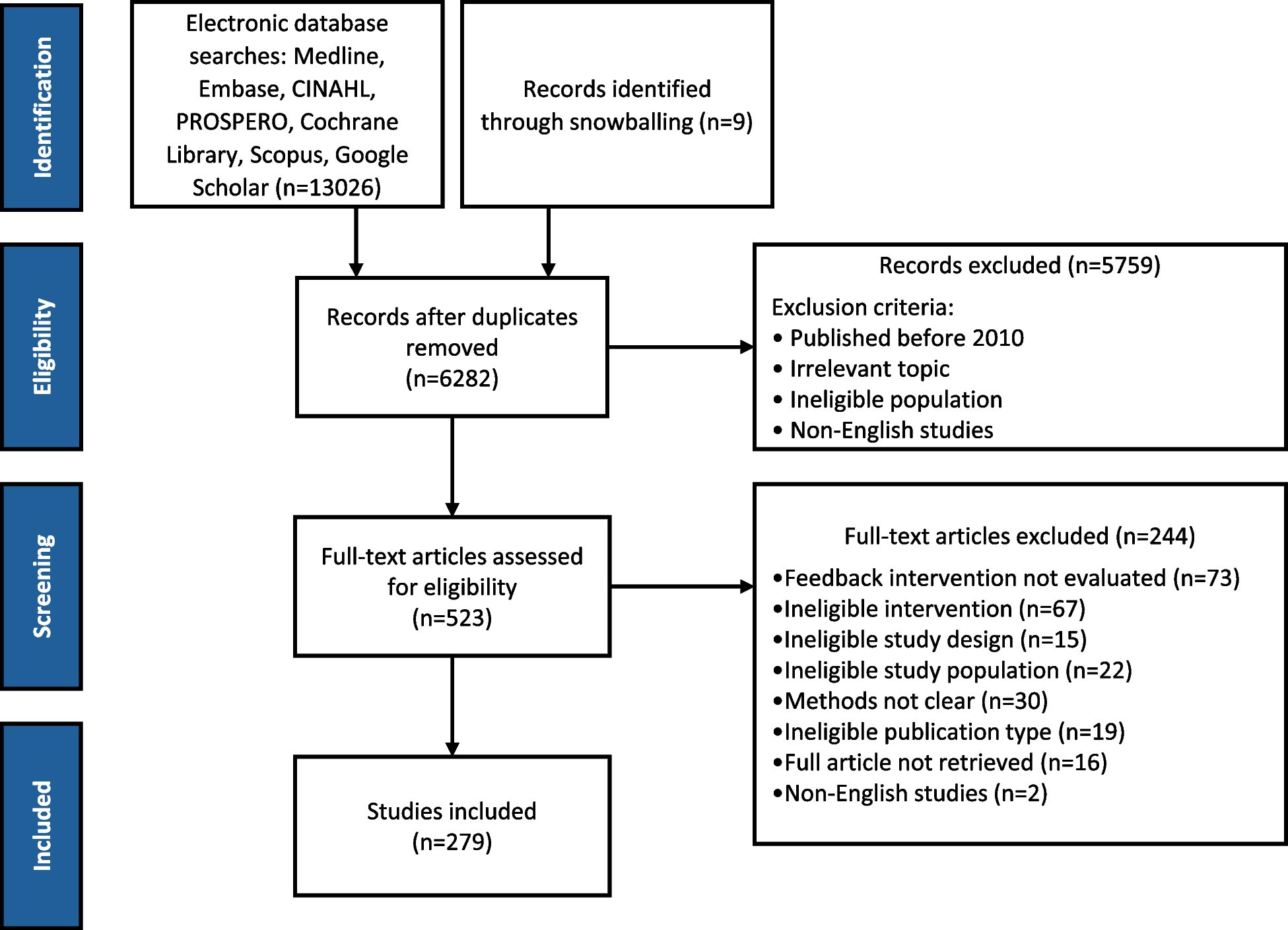






After screening titles and abstracts (550) and full-text documents [40], 23 documents summarizing 32 policy codesign studies met the eligibility requirements (Fig. 1, Table 1). Documents were excluded for describing research-practice partners rather than a time-limited codesign effort (n = 32), not providing enough information on approach (n = 12), not including multiple sectors (n = 4), not relating to policy (n = 4), and not describing codesign in sufficient detail (n = 4).
Fig. 1 Table 1 Study characteristics and policy focusCharacteristics of included documents (n = 22 documents)
Table 1 Study characteristics and policy focusCharacteristics of included documents (n = 22 documents)Documents included codesign studies across multiple continents, Australia/New Zealand (32%), UK/Europe (32%), South America (14%), Africa (9%), and USA/Canada (23%). The types of documents were classified as case studies (77%) which included qualitative description of phases and participant responses, descriptive studies (9%) which included quantitative process evaluation methods, syntheses (4%) which included comparisons of outcomes among different codesign efforts, and opinions (9%) which described codesign activities within a debate or opinion article.
Health focus and policy type (n = 32)Health areasThe focus of health policy ranged widely. Eleven studies (34%) focused on health or social services delivery (e.g., early childhood education, mental health, substance use, tuberculosis care), followed by housing policy (9%), economic development/employment (9%), water supply (6%), built environment (6%), public health (6%), and general health policy (13%).
Policy typeLittle p policy change was predominant (47%), which included organizational agreements and clinical guidelines. Big p policy (25%) included laws, regulations, or financing changes. Service innovation (25%) included the development of new programs.
Frameworks and definitionsRange of definitionsThe most commonly used term to describe efforts was codesign (44%), followed by coproduction (16%), human-centered design (9%), participatory policymaking (6%), design-led policy (6%), participatory communication (3%), public participation (3%), community-engaged evidence synthesis (3%), cocreation (3%), coprioritization (3%), and knowledge-system action analysis (3%) (Table 2).
Table 2 Codesign descriptions and characteristicsTheoriesReferenced theories included formal design-thinking frameworks (44%), political science frameworks (38%), or health services research frameworks (16%). Coders drew from the journal discipline, the department, or the organization of the authors to assign studies to one of these three framework types. Studies referencing design-thinking emphasized the advantages of codesign for developing innovative solutions to intractable health policy problems. A foundational citation found in a reviewed paper included, for example, Verganti [61], Design-driven innovation, changing the rules of competition by radically changing what things mean. Political science theories emphasized citizen/resident engagement in public governance. A foundational article cited by reviewed studies included, for example, Mitlin [62], With and beyond the state—coproduction as a route to political influence, power and transformation for grassroots organizations. Health services research studies emphasized the use of evidence synthesis or research evidence as a part of social and policy innovation. For example, Richardson [32] describes a health services research study that pivoted to codesign after a researcher-led approach failed to capture sufficient interest and participation.
Engagement level of intended beneficiaries (policy users)The most common level of policy user participation was representative (50%), in which policy users sat on advisory teams but did not have full decision-making power. This was followed by full ownership (25%) in which policy users had voting or comparable influence on decision-making and informant (25%) in which policy users were consulted by were not involved in decision-making. Two studies were deemed to include no involvement (6%) in which policy users were not part of the policy codesign process.
Multi-sector involvementConsumer/community was the most commonly involved sector (84%), followed by government (78%), nonprofits (38%), research and universities (44%), service provider/industry (44%), and philanthropy (6%). The number of sectors within each study ranged from 2 to 7 with a mean of 4 sectors per study.
Codesign structureNumber of phasesThe number of phases across studies ranged from 2 to 10 with an average of 5 phases.
Description of phases. Activities within the first phase generally fell into either information gathering (e.g., mapping, literature review) or sector engagement (e.g., coalition-building, developing Memorandums of Understanding). Middle phases tended to include synthesis, presentation, and/or feedback activities (e.g., forums, workshops). Final phases tended to describe a product or final presentation and some studies reflected an intent to engage in continuous policy implementation. We identified a common pattern of linearity in phases: (1) scope the project and build a team, (2) convene stakeholders, (3) gather information from diverse sources, (4) integrate information and prototype solutions, and (5) test for acceptability. Within this general pattern, studies varied significantly in the strategies used to plan, convene, gather information, integrate information, prototype, and test (Fig. 2).
Fig. 2
Strategies within phases of policy codesign
Perceived benefitsOpen coding analysis of the reported benefits of policy codesign across studies yielded five themes: increased knowledge of community needs, community mobilization and equity, feasible policy options, multi-sector alignment, novel ideas, and critical thinking (Fig. 1). To provide context for the authors’ reports of perceived benefits, we provide a study example for each type (Table 3).
Table 3 Beneficial outcomes and challenges of policy codesignAn increased knowledge of community needs was noted in 20 studies (63%). A case study reported in Hagen [63] to increase engagement in early childhood education services noted that “the work emphasized how front-line staff and citizens were willing to share their experiences and actively participate in the development and implementation of new ideas” (pg. 42). The codesign process began with in-depth interviews of early childhood education staff and parents and synthesis of subject matter expert knowledge collected through an invited presentation. The synthesized information was brought into an “ideation workshop,” and prototyping solutions were conducted with early childhood education staff and parents.
Community mobilization and equity were a reported benefit in 16 studies (50%). Ostrom [50] noted “In Brazil, many urban neighborhoods that had never undertaken collective action were empowered by the action of government officials to make real decisions and coproduce an urban service that was highly valued” (pg. 1078). The process began with compiling key information on housing and holding meetings to discuss this information in individual neighborhood blocks. The meetings provided a dual function in facilitating discussion between neighbors on key issues related to design and providing information to government city planners about citizen concerns. Subsequent communications and negotiations were informal and ended in a signed agreement from residents about the housing development plan.
The development of more feasible policy options was reported by 13 studies (41%). Lloyd-Williams [57] reported a case study to develop prevention strategies for non-communicable diseases (NCDs) in the UK. They noted that “strategies to prevent premature NCDs therefore potentially represent ‘wicked’ problems…co-production could well be valuable, potentially providing context, relevance, and reality checks regarding feasible strategies” (pg. 19). The presented case study described a process engaging health policy and decision-makers across the UK. Policymakers were engaged in four workshops that iteratively prioritized and narrowed the range of feasible and effective policy options to prevent NCDs.
Improved multisector alignment was noted by 10 studies (31%). Freebairn et al. [14] presented three case examples of participatory dynamic simulation modeling as a strategy to engage “policymakers, researchers, scientists, clinicians, and consumers.” They noted that “an important element of coproduction in these case studies was equal partnering with key stakeholders to negotiate the priority issue” (pg. 10). The approach taken in the case studies involved assembling an initial codesign team to produce a starting model to conceptualize the issue followed by workshops with larger teams to refine conceptual models (i.e., services and casual pathways leading to service outcomes) for the health area.
The introduction of novel ideas and critical thinking was noted in 15 studies (47%). Van der Bijl-Brouwer [40] presented a case study of developing a new service approach to providing mental health crisis response. The author noted the “the method…provides a ‘backbone’ to the human-centered innovation process, by indicating how insights gained through a specific method, e.g., stakeholder interviews, feed into the framing process, and through that that the innovation process” (pg. 13). The approach used was conceptualized as human-centered design, using Dorst’s frame creation methodology [64].
Relationships between policy user participation and reported benefitsWe conducted a descriptive analysis to explore potential associations between the reported benefits of codesign and level of user involvement. Omitting the two cases with no user involvement, we ran a cross tabulation of user involvement level (informant, representative, full ownership) and the five reported outcome areas that emerged from content coding (Fig. 1). We calculated within group percentages of user involvement by outcomes via counting cases within user involvement level and outcome type and dividing by the total cases for that user involvement level. For example, to calculate the percentage of cases at the users as informant level reporting “increased knowledge of community needs,” we summed the cases coded at the informant level reporting this outcome (n = 3) and divided it by total number of cases at the informant level (n = 6), resulting in 50% of the informant level cases demonstrating “increased knowledge of community needs” (Fig. 3).
Fig. 3
User ownership and policy codesign outcomes
Community mobilization and knowledge of community needs were more frequently noted by studies aiming to engage user ownership in policy development. Community mobilization as a beneficial outcome was noted by 100% of the 8 case studies coded at full ownership, compared to 20% of cases coded as only representative involvement (n = 8) and 70% of cases coded as informant level involvement (n = 6). Novel ideas/critical thinking was most frequently mentioned by cases with users involved at the representative level (70%), compared to full ownership involvement (30%) and informant involvement (50%). No clear difference emerged for multisector alignment or feasible policy options among user involvement level, with both outcomes noted by 50% or less of the assessed case studies.
Perceived challengesStudies across disciplinary types and methods repeatedly noted that a codesign approach takes significantly more time and person resources than “typical” policy development approaches (e.g., expert-led consulting and forecasting) [43, 56, 60, 63, 65]. Authors reported the need to allow time for building relationships and trust, particularly when the initiative aims to engage citizens and consumers and where there is a power imbalance among engaged stakeholders. The studies also highlighted the need for codesign teams to have adequate skills in facilitation and project management in proportion to the degree to which efforts aimed to engage multiple sectors, diverse views, and sources of information [40, 43, 60, 63]. Lack of adequate experience or skills in these areas could lead to a loss of perceived credibility, shared sense of mission, and engagement.
Several studies also noted the emotional burden codesign can place upon consumer and citizen participants, particularly when consumers are asked to reflect on poor service delivery or difficult health experiences (e.g., navigating crisis services) [19, 46]. Similarly, authors noted that codesign can be taxing on facilitators who are tasked with maintaining the engagement of diverse participants [46, 50, 63].
Skepticism towards codesign from policymakers and decision-makers and anxiety from stakeholders about the ambiguity of project aims in the early phases of the process were repeatedly noted by authors [41, 45, 63]. Authors also noted the importance of continuous reorientation for engaged stakeholders to the phase and goals of the project and the through-line of synthesized information in final recommendations and policy products [43, 46, 50, 63]. Relatedly, authors noted that the skills needed to facilitate codesign are not routinely found in public administration, posing a challenge for the successful implementation of codesigned policies as well as the broader use of these approaches in routine policy development [49].
Comments (0)