
Remember me






This project seeks to determine whether a QI intervention to improve appropriateness of antimicrobial prescribing can be implemented in LMIC ICUs as part of an existing multinational Care Quality Registry (CQR) network. We hypothesise that a stakeholder co-designed intervention to improve appropriateness of antimicrobial prescribing can be implemented according to a priori thresholds of fidelity, reach and adoption in participating ICUs. The objectives of this project are therefore:
1.To determine whether a structured antimicrobial review can be implemented in LMIC ICUs
2.To evaluate the impact of a structured antimicrobial review on rates of antimicrobial density, redundancy and associated indicators of antimicrobial utilisation.
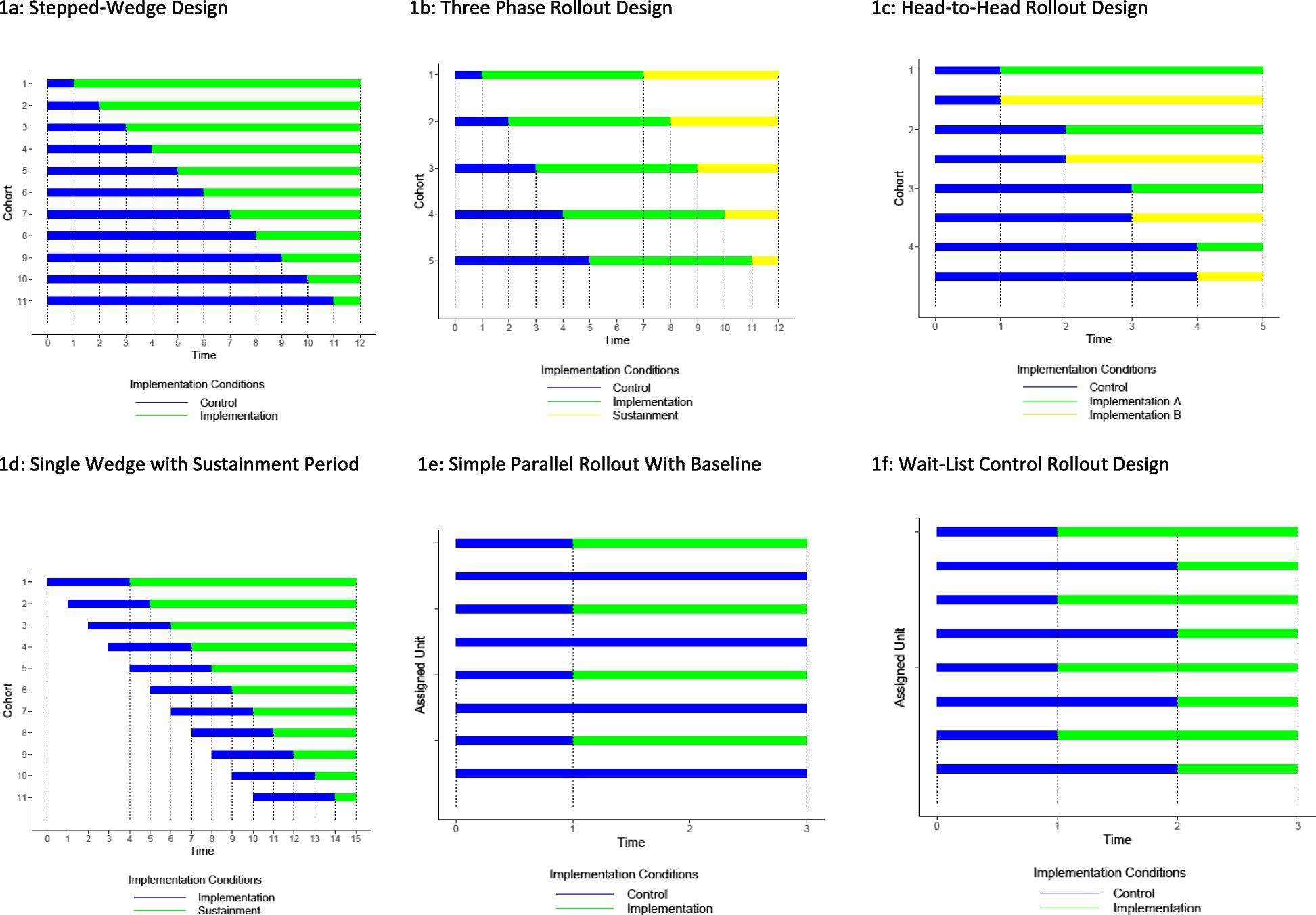
Project DesignWe report this protocol using the SPIRIT guidelines for reporting intervention trials (Supplementary file 1) [27]. This project is a hybrid implementation—effectiveness design, with the primary outcome being implementation (assessed by fidelity, reach and adoption), and the secondary outcomes being the success of the intervention on improving antimicrobial prescribing (care processes and outcomes). Such hybrid study designs are increasingly advocated in healthcare improvement [28]–[30]. This project uses a person-centred approach [31] whereby national CQR and ICU clinical stakeholders will have ownership of the project within their clinical settings. The implementers are appointed ICU Champions, and they, together with the stakeholders, will be responsible for engagement of sites, navigating institutional administration, providing input into the design and implementation of the intervention, and its subsequent adaptations to achieve adoption into daily practice [31]. The RE-AIM (Reach Effectiveness Adoption Implementation Maintenance) framework will be used to structure the evaluation of the project [32]. This framework provides a widely accepted and reproducible guideline for evaluating implementation studies. Designed to assess both implementation effectiveness and its determinants, RE-AIM also informs future scalability and sustainability. Primary and secondary outcomes will be collected using both quantitative data (via the existing CQR dataset and a project E-CRF) and qualitative data captured through interviews with the ICU Champions.
Ethical considerationsThe project will be conducted in accordance with relevant national and international guidance and regulations, including the Global Code of Conduct for Research in Resource-Poor Settings [56]. To ensure that the project is conducted in an ethical manner, this protocol has been approved by the Oxford Tropical Research Ethics Committee (OxTREC – ref 559–24, Supplementary File 7 [57]). CQR national leads will be responsible for coordinating with their participating sites for any institutional or institute review boards for relevant approvals. Individual patient consent will not be sought as the intervention intends ICU level service improvement in line with international recommendations. All patient level data will be anonymised. Champions will give verbal consent prior to being interviewed and can withdraw their consent at any stage (see Supplementary File 4 – Participant Information Sheet).
SettingCollaboration for Research Implementation, Training in Critical Care, Asia Africa (CCAA) is an international network of Care Quality Registries (CQR), spanning 15 countries and 300 + acute and critical care units. Following stakeholder selection of QI indicators in 2022, eleven collaborating registries elected to implement AMS surveillance in their respective CQRs; Afghanistan, Ethiopia, Ghana, India, Kenya, Malaysia, Nepal, Pakistan, South Africa, Uganda and Vietnam.
Site selection criteriaAll adult ICUs within CCAA-affiliated CQRs, where surveillance of antimicrobial utilisation has already been established will be considered for participation. ICUs must appoint a named Champion in order to participate. A survey (Supplementary File 2) will be conducted to determine pre-existing AMS processes and current adoption of structured review activities. Pre-existing antimicrobial review processes are neither a requirement for an ICU to participate nor an exclusion criterion. Instead, parallel to the survey, pre-implementation patient-level data pertaining to current antimicrobial prescribing review practices will be measured during months 1–2. ICU’s which are found to already have a structured antimicrobial review in place, and which demonstrate adoption and reach of 80% or greater (median over the 2 months) will not be eligible to participate in the implementation. This is because the baseline activity will confound the selected measures for implementation success. However, findings of the project will be shared with those ICUs, along with opportunities to participate in subsequent improvement activities.
RecruitmentWe anticipate recruiting between 35–40 ICUs. Using existing CQR data from collaborating registries, we estimate that 75% of adult patients admitted to ICUs receive one or more antimicrobials. ICU occupancy varies between ICUs, but we estimate a median admission rate of 40 patients per month. Therefore, we expect a median inclusion of 180 ICU patient encounters for each ICU during the 6-month period, (totalling approximately 6300 ICU encounters).
Interviews with ICU Champions are described below. One interview with each Champion will be conducted during months 4–6, and one following month 6, resulting in 70 interviews (35 ICUs*2) and 3 months of field notes (recorded during months 4–6). Implementation challenges and effectiveness are likely to vary across sites, so we aim to include qualitative data from all sites. Qualitative data may, however, have a lower sample size as we will stop during each round when we reach saturation or predictability (data will be analysed contemporaneously).
Intervention: structured review of antimicrobial prescribing appropriatenessRationaleStructured multidisciplinary antimicrobial prescription reviews have been demonstrated to reduce overall antimicrobial utilisation and prescription redundancy (‘two or more agents intentionally, or unintentionally duplicating treatment’) [33, 34]. Redundancy directly impacts antimicrobial resistance rates and escalates healthcare costs for patients, providers and payers [22, 35]. Structured prescribing reviews promote: focused antimicrobial agent choice in response to microbiological evidence; avoidance and/or de-escalation of antimicrobial prescriptions where patients are found to have non-infectious syndromes or colonisation; utilisation of enteral routes of administration where appropriate, and avoidance of duplication of prescriptions [36]. Such interventions have appeal in the ICU setting where, in addition to patients with confirmed infection, many patients also present with acute inflammatory syndromes following surgery, injury, or in exacerbations of chronic disease, resulting in rapid commencement of antimicrobials. These prescriptions often occur prior to ICU admission, and once started, are difficult to de-escalate [5]. The WHO toolkit for AMS in LMICs prioritises reducing unnecessary and redundant antimicrobial prescribing and consists of four key steps for review: choosing therapies to best suit indications; optimising routes of administration; limiting therapy duration; and documenting a planned stop date [11].
Conduct of reviewParticipating ICU teams will be required to undertake a structured review of each antimicrobial prescription for all patients receiving antimicrobials. Reviewing prescriptions allows their appropriateness to be reconsidered in the context of emerging clinical and/or microbiological data [37]. The review should be completed within 48 h of a new prescription being commenced, or at ICU admission where pre-ICU antimicrobial prescriptions exist. The review will necessitate documentation of the four key steps as defined by the WHO: indication (in relation to pre-existing local guidelines), route (e.g. parenteral or enteral), expected duration of therapy and intended stop date (including escalation or de-escalation discussions). It will also necessitate documentation of any changes (or lack thereof) made to the prescription, including: the choice of drug, route of administration and duration of treatment. The reviewing ICU team will consider the choice of therapy in relation to the known or assumed indication, the dose in relation to local ICU antimicrobial guidelines, the route of administration, and whether escalation to parenteral, or de-escalation to enteral route (and related dosing and duration adjustments) are warranted. Given the rapidly changing clinical status of critically ill patients, and emerging clinical and/or microbiological data during the ICU stay, it is anticipated that patients may receive more than one review during their ICU encounter. ICUs’ existing antimicrobial guidelines for the management of infections in critically ill patients will be utilised.
Who leads the review, which multidisciplinary members participate, when it occurs during the ICU working day and how frequently it occurs during a patient’s admission will be for the ICU team to decide during the pre-implementation period. The ICU team, together with the Champion will be encouraged to align the intervention with their existing ICU structures (ward rounds, microbiology rounds, etc.), to maximise feasibility and minimise disruption to existing workflows. Given that patient management in the ICU is most commonly led by the consulting clinicians and decision-making often occurs during daily ward rounds, we anticipate that these existing structures will be used, so as to align with existing clinical roles and responsibilities, and to minimise additional workload. Champions will encourage ICU teams to include pharmacists and microbiologists in the review if these specialists are available as the attendance of these team members is associated with improved prescribing practices [38]. How and where the review decisions are documented, will be decided by the ICU team and where possible use existing documentation practices already operational in the ICU. The information must however be accessible to the ICU Champion and Research Assistant (RA) for daily review during the project.
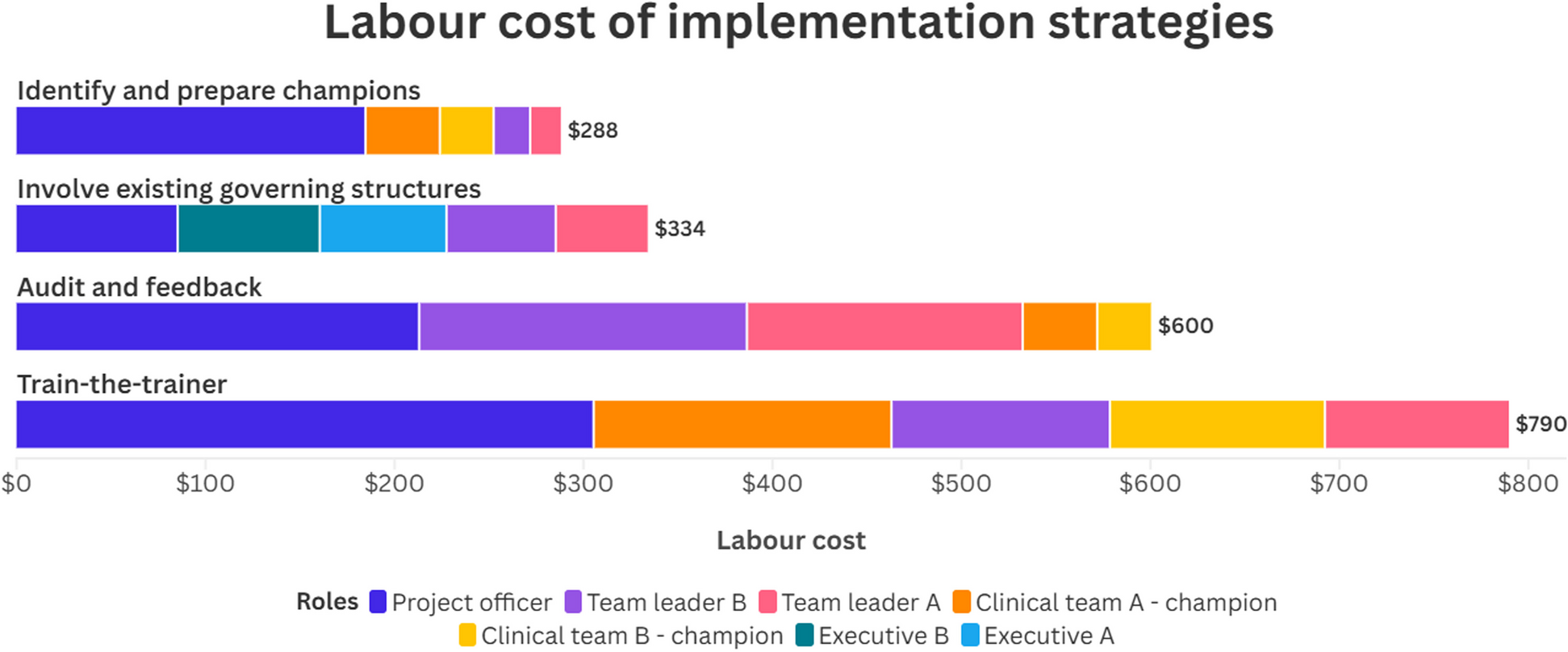
ImplementationDesignA multifaceted approach has been shown to be a critical condition for success of implementation in various settings [39]. Combining implementation strategies has been demonstrated to have a greater success of both implementation and intervention effectiveness when compared to the use of single strategies alone [40]. This project will combine three implementation strategies that have been reported to have been both effective in implementing practice change in critical care in LMICs in a recent systematic review [39], and leverage existing infrastructure already operational in the CQR networks [41, 42]. These strategies are described below and summarised in Table 1.
Table 1 Implementation strategies Strategy 1is agreement and documentation of a local protocol for structured review of antimicrobial prescriptions, as described above (’Conduct of review’). The protocol must include the core aspects which the WHO recommends for review of prescribed antimicrobials [11, 43], but will also include adaptations to the local contexts. Expected adaptations include: which team members perform the review; when during the ICU day the review is performed; how frequently the review is undertaken (beyond the mandate of 48 h post prescription); how the review and its conclusions will be documented and disseminated; when the review should be repeated or revisited.
Strategy 2is a registry-enabled audit and feedback cycle. Audits of clinical practice with feedback to clinicians have been shown to improve health outcomes and clinical performance [44]. The WHO has recommended audits to improve antimicrobial prescribing where they are feasible and costs of collecting data are low [11]. By using the existing CQR data and infrastructure we can: 1) provide near-real time feedback on clinical practice and data quality; 2) empower health professionals to act on the feedback and improve clinical practice and data quality; 3) enable efficient health service planning and future research; and 4) automate a large proportion of the data collection for assessing outcomes [45].
Audit and feedback for the project will augment an existing CQR report whereby data on case mix, clinical outcomes, and proportion of patients receiving antimicrobials, along with the following measures of antimicrobial utilisation are reported monthly: Antimicrobial Density (AD), culture availability, Duration of Therapy (DoT) and Antimicrobial Resistance Index (ARI). More details on this dataset are published [42, 45, 46]. For the duration of the project (7 months), existing antimicrobial utilisation reporting will be augmented by the measurement and reporting of antimicrobial redundancy rate. Once structured prescribing review commences, the proportion of eligible patients receiving a prescribing review within 48 h will also be reported, along with each ICU’s performance on the 4 components of the review (indication appropriateness, route, duration and stop date) compared to other participating sites. Data on indications and microbiology data will also be captured and reported. Following commencement of the review, frequency of reports will be increased to weekly (for a maximum of 3 months). Champions will be encouraged to facilitate review of the report and discussion of the audit data with the wider ICU team, at their preferred frequency and structure, but as a minimum weekly. The presence, format and structure of the weekly discussions will be reported by the Champions. Feedback from the ICU teams on the report structure will be sought prior to and during implementation.
Strategy 3is an online education resource to support Champions and ICU teams during implementation. Education has been recommended as a ‘persuasive’ AMS intervention [11] and is synergistic when used in conjunction with Audit and Feedback [9, 17, 47]. The resource will be available through an already existing online CCAA platform co-designed with stakeholders in 2020. The platform has a series of QI modules, aimed at supporting clinical teams who are seeking to undertake quality improvement initiatives in their ICU. The material includes interactive teaching methods, self-assessments and case studies from QI interventions implemented already in acute and critical care in LMICs. This material has already been used successfully in published outputs from the CQR network [48]–[50]. For this project, an additional module specifically focused on AMS will be included. The module will explain the rationale underpinning the prescription review process and the WHO AMS LMIC toolkit, including the dimensions of and justification for the prescribing review. The resource will be available to all ICU teams, and the Champions throughout the project period. In month 1, Champions will define a list of eligible staff members who they feel should engage with the education tool in order to support implementation. Engagement will be tracked by measuring the proportion of these staff who access the tool.
Implementation team membersEach participating ICU will be asked to identify a Champion for the project. This person will have clinical knowledge and will be from allied specialties who are involved in antimicrobial prescribing in the ICU (e.g. pharmacist, doctor, ICU nurse). The Champion will undergo online training in QI strategies, the intervention and its implementation alongside regular mentorship from the project team throughout the project period. The Champion will be responsible for all aspects of coordination with the ICU team, be the ‘implementer’ within the ICU, and the direct communicator with the project team. At the beginning of the project, they will liaise with the ICU team to complete an online survey (Supplementary File 2) to identify the nature of any existing antimicrobial review processes and other core elements of antimicrobial stewardship. They will have responsibility for the organisation of the ICU team, onboarding to the project, and implementation of the reviews. They will facilitate the weekly audit and feedback cycles, and provide support and feedback to the project team identifying, recording, and solving barriers to implementation [17]. They will be supported by a research assistant (RA) at each ICU who will be recruited for a maximum of 8 months, to support the intervention-specific data collection. The RA will work in partnership with the Champion and the existing CQR data collector. The Champion will also be invited to join online sessions to review and reflect on accruing process and outcome data with the project team and Champions from other sites.
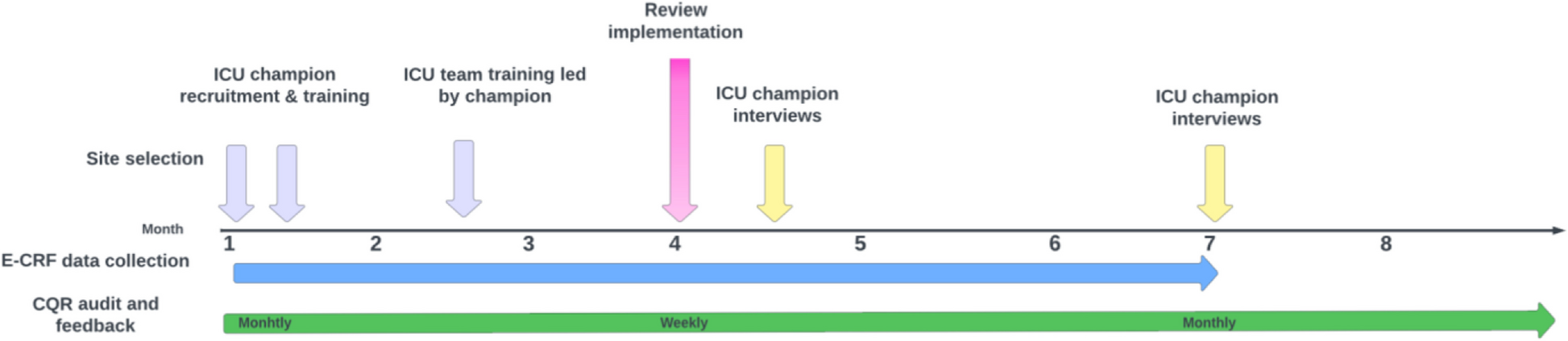
Implementation procedureThe project timelines are illustrated in Fig. 1. Baseline data collection will occur during months 1–3, during which data pertaining to current antimicrobial utilisation and prescribing appropriateness will be captured daily through the CQR, E-CRF and site survey. During this pre-implementation period, the Champions and RAs will undertake online education and receive training from the project team in review processes and orientation to the data in the A&F reports. In parallel, the Champions will engage the wider ICU team to complete the actions described above. Data on existing prescribing practices, which is already captured as part of the CQR report (see Table 1 below) will remain available to the ICUs.
Fig. 1
At month 4, ICU teams will commence the protocolised review in their ICU. The Champion will have access to the online enhanced CQR reports, and the online education material will remain available to all ICU team members. Online support for troubleshooting relating to the implementation strategies will be available to the Champions. In addition, voluntary monthly group sessions will be facilitated by the project team from months 4–6, whereby Champions, RAs and other team members will be welcome to join to reflect on their experience and share learning between sites. Daily data collection (CQR and E-CRF) will continue throughout this period. Champions will be interviewed during months 4–6 to explore barriers and facilitators to implementation, adaptations made to both the intervention and its implementation, along with perceptions regarding likely adoption and maintenance (Supplementary File 3).
At the end of month 6, the implementation strategies of online education, the role of Champions, and the RA collecting daily data on review processes will cease. The daily auditing of whether reviews take place will be transferred to the CQR data collectors and reported monthly as part of the CQR report. A second interview will be conducted with Champions following month 6 to explore barriers and facilitators to adoption, and adaptations to the intervention made post-implementation (Supplementary File 4).
Adaptations to implementation planIt is expected that ICU teams will make adaptations to their prescribing review processes. These adaptations will be captured throughout the project by Champions (in implementation logs) and synthesised by the project team as part of the evaluation. Adaptations may also be made to the implementation strategies, with the proviso that any adaptations are made at a ‘project level’, meaning uniformity of materials and resources across all sites. Site or regional level adaptations to implementation strategies will not be made. For example, the structure and/or content of weekly reports may be adapted, or elements may be added to or removed from the online education resource, following feedback. Such adaptations, and the reasons for them, will be logged, explored during interviews and synthesised.
OutcomesPrimary outcome: implementationImplementation is the primary outcome and will be assessed quantitatively using 3 of the 5 key domains identified through the RE-AIM framework: Reach, Implementation (defined as fidelity) and Adoption (see Table 1). These will be combined into a composite measure of implementation with a threshold of 80% for success in each domain. Furthermore, Champions’ perceptions of the determinants of successful implementation, including acceptability, maintenance of, and adaptations to, implementation will be captured through field notes and interviews [51].
Secondary outcomes: Intervention effectivenessIntervention effectiveness, defined as the intervention's effect on the relevant care processes and clinical outcomes, will be assessed by reporting ICU trends in prescription appropriateness (Antimicrobial density (AD), treatment duration (DOT) and antimicrobial redundancy rate (ARR, % of total prescriptions)), and processes of care (proportion of patients for whom cultures are sent, antimicrobial resistance rate, antimicrobial prescribing rate and compliance of prescriptions with local guidelines). Clinical care processes and outcomes (mortality, Length of Stay and duration of organ support) will be also collected as safety endpoints. Unintended and/or adverse consequences of the intervention will also be explored through field notes and interviews with Champions.
Feasibility of collecting outcomesEligible ICUs will have had a CQR established for at least 6 months and have an established CQR data collector. Clinical teams will already be trained in use of the CQR, and in the review and interpretation of CQR reports which will be used for audit and feedback. ICU team members, including the Champion will work together with the existing CQR and clinical teams to ensure that data on implementation and care processes can be integrated into analysis of outcomes. This will include records that include (1) diagnoses, (2) prescriptions of medications, (3) investigations and observations, and (4) care processes associated with AMS and the preselected outcomes. Information on the 4 steps of review (indication, route, expected duration, and expected stop date) will be recorded, either on paper, or electronically and reported as part of the audit and feedback as described above. CQR reports will be generated centrally by the CCAA data coordinating centre and made available to sites through existing mechanisms. Data pertaining to the availability of the above review and CQR information will be used as part of the implementation evaluation.
Data collectionData regarding case mix (including source and reason for admission, severity of illness at admission, comorbidities) along with physiology, organ support, antimicrobial prescriptions and microbiology data, care processes (duration of antimicrobials) and clinical outcomes will continue to be collected daily through the existing CQR during months 1–8. The CQR data collectors will also collect adoption and reach of any pre-existing structured review during months 1–2.
A project specific E-CRF on REDcap [52, 53], will capture data on antimicrobial reviews during months 4–6 (see Table 1 above). This additional E-CRF collection will be done by the RAs. Copies of existing antimicrobial guidelines will be requested prior to commencement of the study, and ICU stakeholders’ perspectives regarding the current guidelines, along with information on existing antimicrobial stewardship activities already present in the ICU captured during the site onboarding by Champions. Changes in guidelines made during the project will also be captured, and the current working version of the guidelines queried at each phase of the project. Post implementation (months 7 onwards), the CQR data collection will continue, along with a measure of adoption.
Qualitative data exploring the Champions’ perspectives regarding implementation, acceptability, adoption and maintenance, along with contextual factors influencing implementation will be collected through semi-structured interviews at two time points during the study: implementation (months 4–6) and post-implementation (month > 6). We intend to interview all Champions during both phases but recruitment may cease if concurrent analysis indicates that theoretical saturation has been achieved. Interviews will be conducted remotely using the Zoom (Zoom Video Communications Inc, San Jose, CA, USA) conferencing application. A participant information sheet (Supplementary File 5) will be provided and verbal consent for participation sought (Supplementary File 6). In addition, Champions together with RAs will be requested to maintain an implementation log [54], whereby adaptations, and observed barriers and facilitators to implementation will also be reported. These will be reviewed and thematically coded alongside the interview data.
No site or follow-up visits by the project team are required, as the design of the project is such that ICU teams together with Champions have direct ownership at site level, and the project seeks to minimise additional burden of data collection for clinical staff. All patient level de-identified data will be submitted by collaborating CQRs using existing processes. All data will be inspected before analysis to rule out spurious values, and appropriate transformations implemented where necessary. Existing data quality measures already operational within the CQRs will be utilised to provide information on data availability and reduce erroneous or missed data. These measures are already described in detail and published [55]. Once cleaned, data will be aggregated and anonymised at ICU level for monthly and weekly reporting (audit and feedback) and for the subsequent project analysi.
AnalysisAll analysis will be conducted at the level of ICUs. ICUs will be identifiable only by their type (i.e. medical, surgical, mixed or speciality), and by their organisation governance type (private, public, other). ICUs who have a pre-existing structured review with an adoption rate of 80% will be included in the context description, but not in the intervention analysis described below. No country or regional level analysis is planned. However participating CQRs will have access to their sites’ data for subsequent evaluation once the primary outcome is published.
Primary outcomeSuccessful implementation will be assessed by a composite measure combining rates of fidelity, reach, and adoption. Recent literature describes that for a multifaceted intervention to affect clinical practice change, implementation threshold needs to be 80% [58]–[63]. We will therefore consider this as the threshold for successful implementation at ICU level.
Secondary outcomesFor the secondary outcomes of intervention effectiveness, we propose a 10% absolute reduction in Antimicrobial Redundancy Rates (ARR) (Supplementary File 8), Antimicrobial Density (AD), and Duration of Treatment (DoT) (independently), compared with the baseline period, for successful intervention at the ICU level.
StatisticsFor the primary outcome, we will describe the proportion of ICUs that achieved ≥ 80% of all three indicators (fidelity, reach and adoption). We will also report these indicators separately. We will compare the proportion achieved in the post-implementation period, as specified in the Table 2, with the baseline assessment, using a McNemar test (Chi-square for repeated measures).
For the secondary outcomes, we will perform an interrupted times series analysis. We will observe the weekly temporal resolution of each indicator and set the model to account for the natural/secular time trend, implementation of the intervention (level change) and the trend after implementation (slope change). We will account for auto-correlations. The model applied will depend on the data, but we will evaluate ARIMA models, segmented regressions and Holt-Winters additive model to evaluate the best model for the times series. Counts of actions recorded in response to the review will be described. The code lists for the primary and the secondary outcomes, and definitions for indicators of quality will be developed and published in advance of data collection.
Qualitative analysisQualitative data will be analysed thematically and contemporaneously to data collection. Analysis of barriers and facilitators to implementation will be informed by the Consolidated Framework for Implementation Research (CFIR) framework [64]. Transcripts of the interviews will be deductively analysed independently by two researchers (DW and AB) to identify the key concepts (themes) regarding acceptability and maintenance of implementation, along with barriers and facilitators to implementation. DW and AB have extensive experience of working in ICU clinically and as researchers internationally. Initially the text will be open-coded by reviewing all text line by line and then descriptive codes will be assigned to the words, sentences and paragraphs in the transcripts. At this stage of the analysis, lines in the transcripts will be linked and grouped as the first set of codes which relate to the current prescribing practices, the experiences of the ICU team, RA’s and champions, along with adaptations made. Axial coding in the next step of the data reduction process will link the descriptive codes via repackaging and combine the data to identify categories that have similar characteristics [65]. After developing categories, the relationships between the categories will be explored to reveal higher level themes, and then where relevant to implementation of the intervention mapped to the CFIR framework [64]. New themes, and contextual and team factors that emerge from the evaluation but do not fit the existing framework will also be reported.
Comments (0)