This study is a nationwide study including all 66 Danish patients who fulfilled the clinical criteria of JPS and/or had a PV in SMAD4 or BMPR1A. We found that almost 90% of patients with a clinical diagnosis of JPS had a PV in either BMPR1A or SMAD4. Endoscopy had been performed in 52 patients, and 21 (40%) of these did not fulfill the Jass criteria. Furthermore, the removed polyps frequently were other types than juvenile.
SMAD4 and BMPR1A: the only genes associated with JPS?
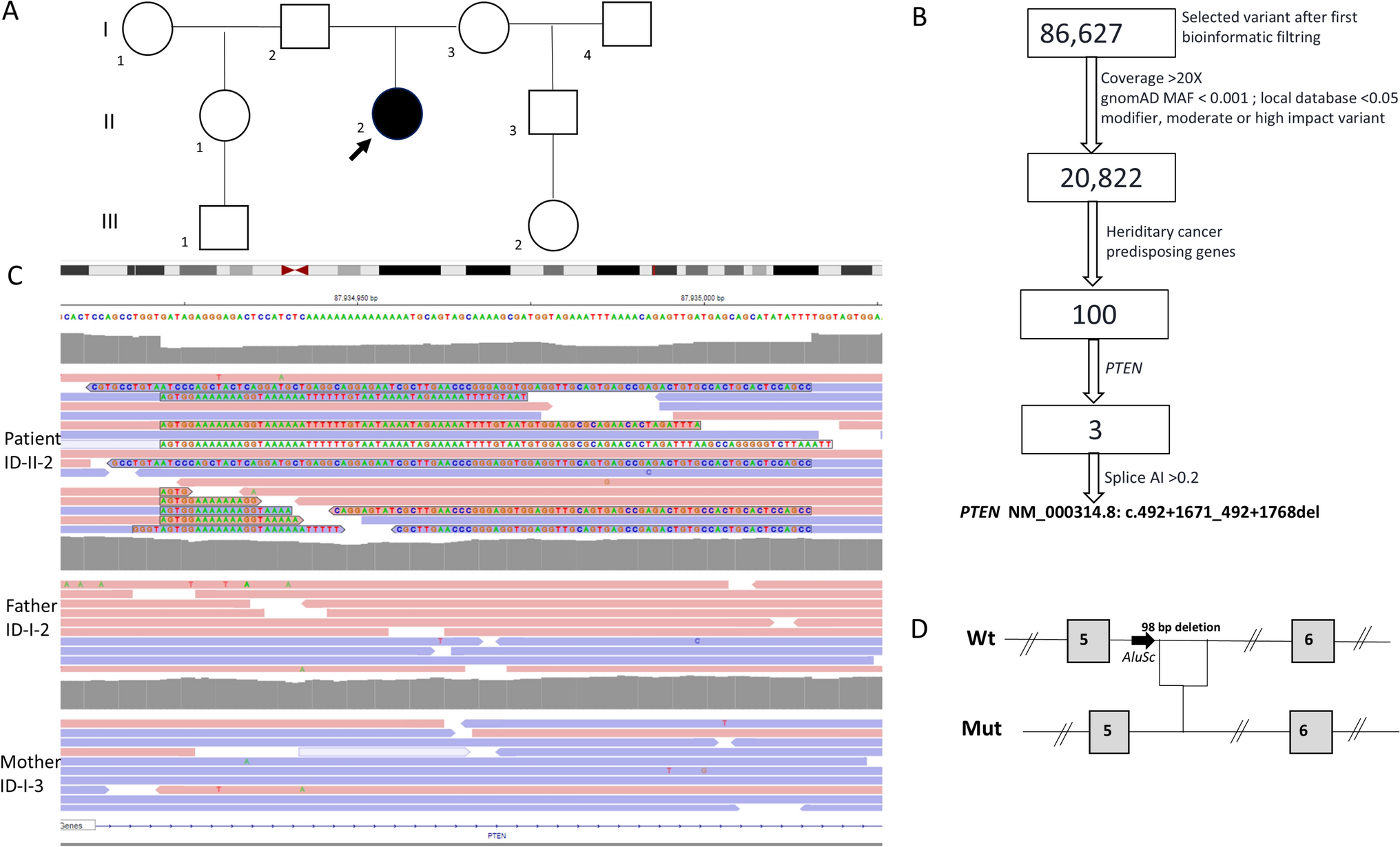
Previous studies have reported a relatively low variant detection rate when analyzing SMAD4 or BMPR1A indicating genetic heterogeneity [1, 5,6,7,8] (see Table 4). Our study as well as others suggest that PVs in PTEN are found in an additional (small) number of patients [7, 15]. The implementation of NGS, including WGS, did not add significantly to our detection rate.
Table 4 Detection of gene variants in JPSThe reason for the discrepancy in the variant detection rate between our study and most others is uncertain. Possibly, it could be caused by differences in methods used for identification and inclusion of patients. The mode of inclusion in our study is quite robust, as inclusion was based on data from The Danish Pathology Register: The register comprises data from all histopathological examinations carried out in Denmark since 1997, and for some departments even earlier. Although the significantly higher detection rate is unexplained, our findings, along with the findings by Latchford et al. suggest that in most cases, PJS is caused by a PV in either SMAD4 or BMPR1A.
We observed no indication of mosaicism, and to our knowledge this has neither been reported in other studies. Yet, mosaicism for variants in APC and STK11 has been reported [16,17,18], and it seems unlikely that mosaicism do not occur in patients with JPS. Possibly the phenotype in patients being mosaic for a variant in SMAD4 or BMPR1A is so “mild” that it typically is overlooked.
Varying histopathology leads to underdiagnosis
The high variant detection rate indicates that the Jass criteria [4] are a strong indicator of a pathogenic variant. However, our findings also suggest that there is a risk of missing patients with PVs in SMAD4 or BMPR1A if using these criteria alone: only 60% of the patients with a PV in one of these genes, who had endoscopic investigations, fulfilled the Jass criteria. Thus, one can only speculate that JPS in general is underdiagnosed, and that the calculated incidence is an underestimation. This also suggests that the threshold for performing genetic analysis should be rather low.
The histopathology of the colorectal polyps varied greatly—an observation that has also been recognized in other studies although at a smaller scale [15, 19, 20]. All patients with a PV in SMAD4 or BMPR1A had polyps removed and, furthermore, in approximately 15% of the patients no juvenile polyps (but other types) had been removed. This emphasizes that there should be an awareness, in the clinical setting, that JPS can present with a broad spectrum of polyps. This also indicates that SMAD4 and BMPR1A should be included in the panel of genes analyzed in all patients suspected to suffer from a genetic predisposition to intestinal polyposis. However, the varying histopathology can also be due to misclassification of polyps in the first place as have been reported before [7, 21]. In general, it can be difficult to distinguish different types of polyps from each other and especially juvenile polyps can resemble inflammatory polyps.
The consequences of the varying histopathology were evident in the two patients who had 10–20 colonic polyps removed over a period of 15–20 years. The polyps had shown various histopathology with only few polyps suspected to be juvenile. When participating in our study, both patients were found to have a PV in SMAD4 and were recommended additional upper GI surveillance. Both were then diagnosed with massive gastric polyposis and subsequently had a gastrectomy.
Wide clinical spectrum leading to suboptimal surveillance
In general, we observed that the clinical spectrum of patients with a PV in SMAD4 or BMPR1A was very wide: from massive polyposis (both gastric and colorectal) to very few colorectal polyps. Our findings also support the general conception of a difference in the phenotype of SMAD4-related JPS and BMPR1A-related JPS: We diagnosed more massive gastric involvement and HHT-manifestations in SMAD4-related JPS (Supplementary table 2) compared to BMPR1A-related JPS.
The highly variable phenotype suggests that the current surveillance guidelines impose a risk of overtreatment. According to most guidelines, surveillance of the GI tract should begin at age 12–15 years and examinations should be repeated every 2–3 years [22, 23]. Most agree that surveillance in JPS patients is indicated to reduce the risk of getting and dying from cancer as well as to reduce the morbidity caused by polyposis. However, there is a lack of long-term studies that can support the effect of surveillance. We calculated a probability of cancer at age 70 years to be approximately 50%, but various estimates have been reported and basically, a lack of knowledge concerning the pathophysiological mechanisms makes it difficult to tailor optimal surveillance [24,25,26,27]. As it is, a “one-size-fits-all” program does not seem to fit all. Possibly one could achieve a better balance between the “costs” (i.e. inconvenience of attending surveillance and the risk of overtreatment) and benefits for the individual patient by adjusting the surveillance program by the gene variant causing the predisposition and the personal history of the patient.
Strength and limitations of the study
A limitation of this study is the relatively low number of patients included and a risk of overlooking patients with a mild phenotype. Also, the facts that we ascertained from various sources, that we ascertained both on phenotype and on genotype, and that the patients had various ages at the end of follow-up, may have limited the generalizability of our observations.
However, it is a major strength that our study is nationwide and conducted in Denmark, where the health care system offers services, without out-of-the pocket expenses, to all citizens, where all citizens are identifiable by the unique social security number, and where registration in nation-wide registers, such as the Danish Pathology Register, is mandatory. This made it possible to identify the patient’s medical data and histopathological samples across registers and departments throughout the country, several years back.


Comments (0)