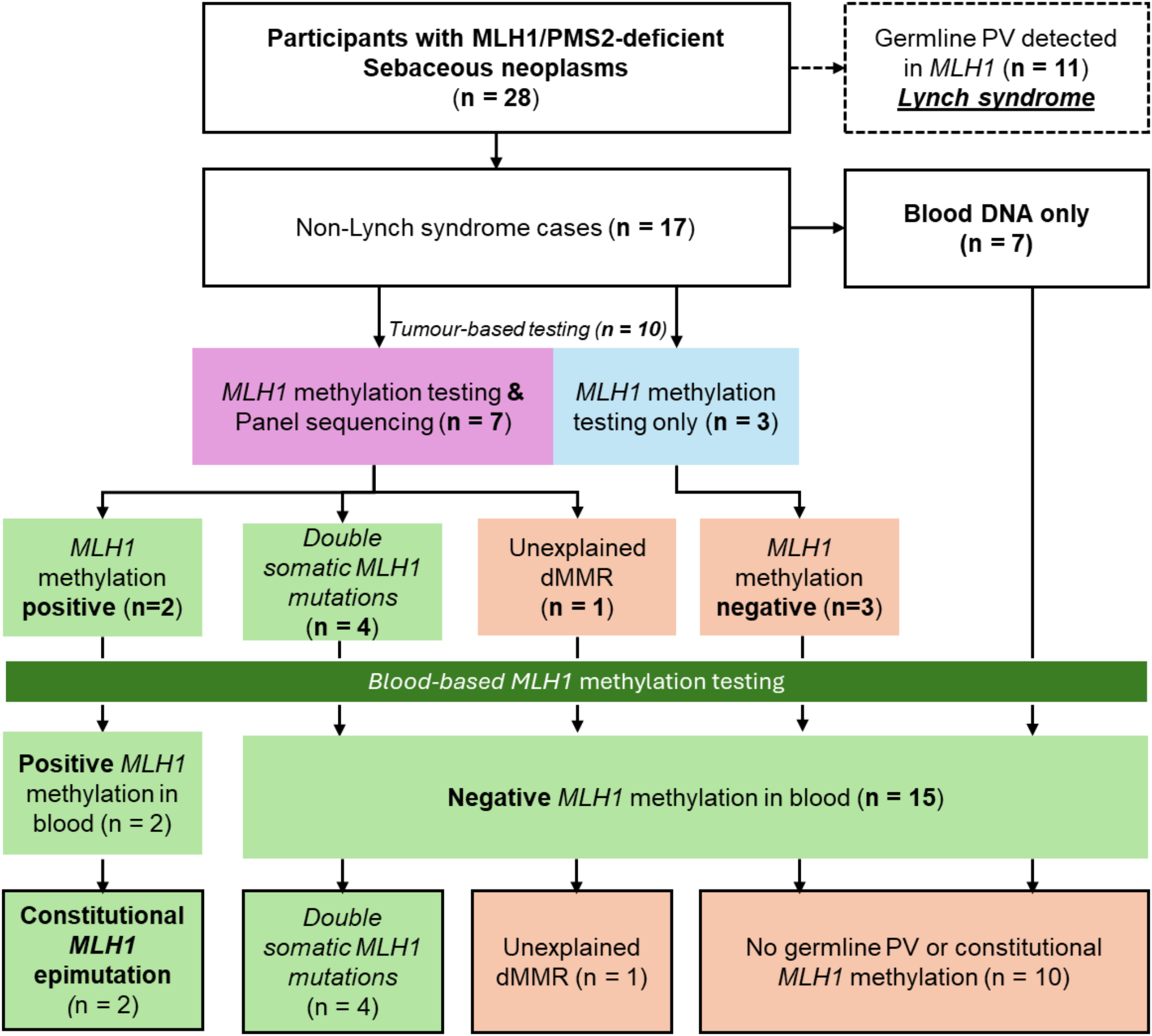
This study investigated germline and somatic mechanisms underlying MLH1/PMS2-deficiency in sebaceous neoplasms. After identifying Lynch syndrome cases due to germline MLH1 pathogenic variants, double somatic MLH1 mutations (n = 4) was the main cause, followed by Lynch syndrome due to constitutional MLH1 epimutations (n = 2). A single case with sufficient tissue DNA enabling both MLH1 methylation and MLH1 somatic mutation testing did not identify either as a mechanism, potentially suggesting a false-positive MLH1/PMS2-deficiency or other mechanisms not captured by the techniques used in this study (e.g. large structural variants, deep-intronic variants).
Three constitutional MLH1 epimutation cases with sebaceous neoplasms have been described to date [4, 8]. Zyla et al. reported a female patient diagnosed with CRC (33yrs), squamous cell carcinoma of the vulva (37yrs), a facial sebaceous adenoma (45yrs) and EC (52yrs) [8]. All tumours exhibited MLH1/PMS2-deficiency and MLH1 methylation testing of the EC was positive. Subsequent blood-based MLH1 methylation testing identified constitutional MLH1 epimutation, explaining development of multiple MLH1-deficient cancers. In our previous study, we investigated the mechanisms underlying MMR-deficiency in CRC, EC and sebaceous neoplasms from people with “suspected Lynch syndrome” or “Lynch-like syndrome” [4]. MLH1 methylation analysis identified two index MLH1 epimutation cases, both with sebaceous neoplasia [4] and are described in this study. This present study, the first to examine both somatic MLH1 methylation and constitutional MLH1 epimutation in sebaceous neoplasms, has provided an important extension of this work demonstrating that somatically acquired MLH1 hypermethylation was not present in the 10 sebaceous neoplasia cases tested, suggesting that this is not a common cause for MLH1/PMS2 MMR-deficiency unlike in CRC and EC.
The tumourigenic mechanism in constitutional MLH1 epimutation carriers is intrinsically different from somatic MLH1 methylation. In CRCs and ECs, somatic MLH1 methylation causes biallelic hypermethylation of the MLH1 gene promoter resulting in complete silencing of the gene [5]. Somatic MLH1 hypermethylation is specific to the malignant cells and associated with older age at diagnosis [9]. In constitutional MLH1 epimutation, monoallelic MLH1 hypermethylation inactivates one allele and a second somatic hit causes biallelic silencing of MLH1 resulting in loss of DNA MMR function [5]. As the tumourigenic process in MLH1 epimutation follows the same process as Lynch syndrome resulting from germline MMR pathogenic variants, cancer diagnosis age in MLH1 epimutation is thought to be similar to Lynch syndrome and younger than cases with somatic MLH1 hypermethylation. Therefore, triaging patients for constitutional MLH1 epimutation testing has often been guided by a younger age at diagnosis [9]. The diagnosis ages of sebaceous neoplasms in three MLH1 epimutation cases, including two from this study and one from Zyla et al. [8], were 55, 49 and 45 years. This is seemingly younger than the mean age of 68 years presented by our previous study of 882 people with sebaceous neoplasia [2], and may suggest that younger age at diagnosis could be useful for differentiating MLH1 epimutation carriers from sporadic cases.
This study demonstrates the importance of both germline and tumour testing in individuals diagnosed with MLH1/PMS2-deficient sebaceous neoplasms. Based on our findings, a potential testing strategy for people with MLH1/PMS2-deficient sebaceous neoplasms would be initial germline MMR gene testing to identify a MLH1 pathogenic variant coupled with MLH1 epimutation testing (Supplementary Fig. 1). For those without germline MMR pathogenic variant, tumour-based testing to identify biallelic somatic MLH1 mutations would provide a definitive diagnosis for an important proportion of MLH1/PMS2-deficient cases. Differentiating constitutional MLH1 epimutation from somatic MLH1 hypermethylation is clinically important, as having Lynch syndrome related toMLH1 epimutation is associated with an increased risk of developing multiple cancers including CRC and EC and may inform familial risk assessment [5]. Furthermore, differentiating primary MLH1 epimutations from secondary MLH1 epimutations resulting from a germline MLH1 promoter pathogenic variant is important for risk assessment in relatives. The two cases identified in our study were primary epimutation cases based on the testing undertaken.
A limitation of this study was the inability to complete sebaceous tissue testing in 10 cases due to the small lesion sizes resulting in insufficient DNA for testing. Although Lynch syndrome related to germline pathogenic variant and constitutional MLH1 epimutation were confidently excluded in these cases, somatic MLH1 methylation cannot be ruled out in these 10 cases. However, findings from the sebaceous tumours we could test suggest biallelic somatic MLH1 mutations are a more likely cause of MLH1/PMS2-deficiency than somatic MLH1 hypermethylation. Validation of our findings will help guide clinical diagnostic testing for people with MLH1/PMS2-deficient sebaceous neoplasia. With a sample size of 28 cases, this study is the largest to perform systematic investigation of germline and somatic mechanisms of MLH1/PMS2-deficient sebaceous neoplasms. We identified 11 participants with MLH1 pathogenic variants, which was the most prevalent mechanism for MLH1/PMS-deficiency, however, this could be an over-representation due to a potential ascertainment bias resulting from recruitment of our some of our participants from Family Cancer Clinics and the ACCFR.


Comments (0)