This retrospective thematic analysis characterised how this MDM benefits clinicians and provides peer support in complex clinical scenarios, particularly where there remains uncertainty surrounding diagnosis and management in the context of rapidly evolving guidelines. The MDM has a role in training, peer support and feedback, as evidenced by volume of queries related to mainstreaming, interpretation of results, and determination of onward management for scenarios not currently represented in best practice guidelines.
We evaluated when MDM recommendations deviated from current guidelines and were able to characterise the MDM’s working patterns in order to ascertain its benefits. We also considered the ways in which specialist MDMs can provide support to colleagues performing mainstreaming.
The virtual format of this MDM facilitates significant collaboration between institutions, evident by the 12 different external institutions providing 77% of the caseload, covering a large geographical region. Established benefits of virtual MDMs were apparent in our analysis, including increased access for those not on site and a streamlined approach to case selection [15].
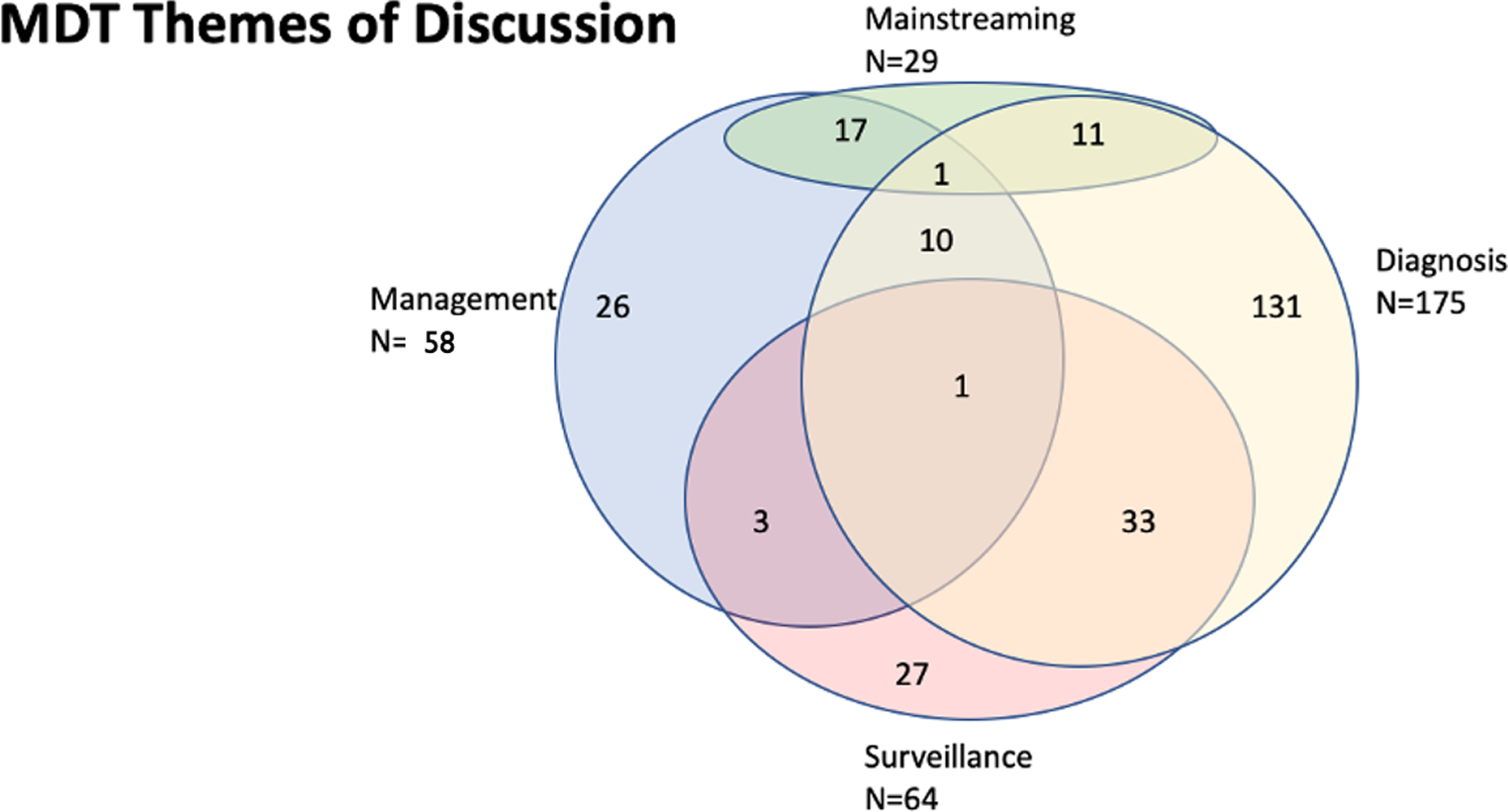
This MDM demonstrated several key areas of diagnostic uncertainty, particularly regarding genetic testing and LLS. The number of further testing queries reflects a previously reported lack of confidence by clinicians in interpreting genetic testing results [16]. Universal Lynch syndrome testing has led to a rise in unexplained dMMR tumours, which may exacerbate this issue [17]. MDM discussion enables situational judgement weighing the likelihood of obtaining a diagnosis against the potential cost to patients and the healthcare service- patients undergoing genetic testing may experience an anticipatory experience of loss [18]. In situations where there is lack of consensus in testing pathways, or when existing guidelines are limited in scope, the MDM provides peer support for clinicians.
A novel aspect of this MDM is the link between clinical geneticists with a specialist interest in cancer genetics, mainstreaming clinicians, and disease specialist clinicians within the SMCFIC, an expert centre for familial CRC management. The number of cases brought to discussion by regional genetics services suggests a mutually beneficial working relationship where specialist knowledge is shared.
Surveillance was the second most commonly discussed theme; its importance in the prevention of cancers and reduction in patient mortality has been well-established [19, 20]. Issues raised included surveillance frequency or which FDRs would most benefit, particularly important when considering variation in intra-familial cancer risk even within known high-risk families [21]. Particularly surveillance guidance surrounding many ultra-rare multiple adenoma syndromes is lacking, therefore relying on input from expert centres such as SMCFIC. Another gap remains in the surveillance of the FDRs of patients with multiple adenomas who lack a genetic diagnosis- the individualization of advice for such families requires expertise [21].
Mainstreaming cases represented 11.1% of the caseload, which is likely to increase as mainstreaming is rolled out across England through the National Lynch Syndrome Transformation Project [14]. Most queries were with regards to management of patient and family, representing one of the most complex aspects of providing care in hereditary colorectal cancer- a diagnosis will not only impact patients but will have a direct impact on FDRs. Therefore, ongoing training and support clinicians who may feel less experienced [12] will remain a key activity of the MDM.
The retrospective nature of the project meant gender and ethnicity data was not available. Any future analyses would benefit from the inclusion of this data as frequency of certain risk alleles vary by ethnicity [22], or incompletely recorded proformas which were excluded from analysis. The heterogeneity within the eligible patient population, and of the outcomes of the MDM, necessitated a thematic analysis, which creates a challenge in demonstration of clinical benefit and justification for the replication of this service in other regions. However we have demonstrated how a regional collaborative MDM facilitated clinicians to navigate areas of uncertainty such as interpretation of genetic testing results, and decisions surrounding offering enhanced screening to high-risk FDRs, particularly in providing peer support in situations where existing guidelines are limited.
The implementation of the Genomic Medical Service in England aims to embed genomics in routine clinical practice, and includes 7 regional alliances (GMSAs). The NHS England LS transformation project includes the development of LS expert networks in each GMSA including access to multiprofessional expertise in the management of clinical and diagnostic complexity in this population [14]. These data indicate the utility of replicating regional MDTs on a national level, given appropriate funding, either in the inherited CRC population or in similar hereditary disease cohorts [14, 23].


Comments (0)