The aim of this study was to evaluate the potential effects of two targeted exercise interventions on symptoms of polyneuropathy in the upper extremities of cancer patients. Both the sensorimotor/vibration exercises (PNPEX) and the moderate resistance exercises (MREX) proved to be acceptable and safe to perform. However, PNPEX showed more significant improvements in selected neuropathy-related outcomes such as the FACT/GOG-Ntx or numbness/tingling (see supplements) [5]. PNPEX not only led to positive developments in terms of vibration sensitivity and symptom reduction, but also to improvements in depth sensitivity and paresthesia at four of eight measurement points (see supplements). This suggests that sensorimotor/vibration-based movement therapy is both feasible and clinically relevant for therapy-related neuropathic symptoms in the upper extremity.
Analysis of response probabilities based on the FACT/GOG-Ntx demonstrated substantial differences between the groups. The results suggest that PNPEX may offer more targeted benefits for PNP symptoms than resistance exercise alone. The FACT/GOG-Ntx, which was originally developed and validated by Cella et al. in 1993 [15], is particularly well-suited to detect subtle changes in neuropathy-related symptoms, and has been established as a sensitive endpoint in PNP research [4]. The findings are consistent with previous studies indicating that sensorimotor and vibration exercise can enhance proprioception and vibration sensitivity, thereby alleviating neuropathic symptoms [8, 9, 13, 14, 21]. Recent results from the VISCIPH A trial further support this interpretation, as PNPEX effectively prevented the deterioration of deep sensitivity in the upper extremities and demonstrated favorable effects on overall health compared to resistance exercise [5]. While resistance intervention remains important for improving strength and physical functioning in cancer survivors, its specific impact on neuropathic symptoms appears to be less pronounced.
Within the PNPEX group, no sociodemographic, clinical, functional, or behavioral variables predicted responder status, reflecting the variability in the response to PNP exercise reported previously [8, 14]. The findings of this randomized controlled trial further support the idea that sensorimotor intervention has high neuro-modulating potential, stimulating the regenerative and adaptive mechanisms of muscle spindles and sensory afferent nerves to promote neural plasticity [13]. In contrast, vibration exercise appears to primarily activate more superficial nerves [13]. These observations suggest that, when regularly trained under progressive load, the human neuromuscular system may preserve neural functions even during chemotherapy. This is consistent with preclinical models showing the potential for peripheral nerve regeneration through activity-dependent mechanisms. In this context, Kleckner et al. (2018) demonstrated that exercise may also modulate central neural processing in cancer survivors, suggesting a dual peripheral–central mechanism [11].
Analysis of the secondary outcomes revealed mainly small changes, with relevant group-specific differences. Both groups showed a reduction in symptoms on the NRS pain scale, although these changes did not reach statistical significance. Conversely, we observed an increasing trend in pain scores on the EORTC QLQ-C30 scale, particularly in the PNPEX group. The divergence between the two pain measures may be explained by their different conceptual focus: the NRS specifically assesses neuropathic pain in the hands, whereas the EORTC QLQ-C30 captures general pain, including tumor- and therapy-related joint or musculoskeletal pain that may accumulate during treatment [4]. Self-reported physical function remained largely unchanged, with a small improvement in the MREX group and minimal changes in the PNPEX group. Comparable intervention studies in patients with chemotherapy-induced neuropathy have also reported only modest changes in physical function [8, 14, 22], suggesting that these domains may require longer or multimodal exercise interventions to achieve measurable benefits. Furthermore, the post-intervention pain scores of both groups fell within the range reported for the general cancer survivor population [23, 24]. This suggests that exercise interventions may primarily stabilize, rather than substantially improve pain perception in the short term. However, global health status improved significantly in the PNPEX group, while the MREX group showed only a small, non-significant increase. This finding may suggest that reductions in neuropathic symptoms can translate into meaningful improvements in overall QoL, as reported in previous research linking symptom burden and health-related QoL in cancer survivors [24, 25].
In terms of depth sensitivity, both groups improved at the ulnar styloid, but only the PNPEX group showed a significant gain at the first carpometacarpal joint. At the third and fifth carpometacarpal joints, PNPEX again showed more favorable trajectories than MREX, though without statistical significance. These findings are consistent with previous studies indicating that sensorimotor and vibration exercise can improve proprioception and preserve sensory function in patients with chemotherapy-induced peripheral neuropathy [8, 13, 14, 21], whereas resistance exercise appears to be less effective in this area. Alongside the higher response rate in the PNPEX group, these results highlight the potential clinical relevance of neuromuscular exercise modalities. This supports earlier observations that neuromuscular exercise interventions can slow down PNP progression and maintain physical function [22, 25].
However, these findings should be interpreted with caution. Although depth sensitivity values below 5 mm for individuals under 60 years old and below 4 mm for individuals aged 60 years and over are classified as pathological, mean values in our cohort (5.94–7.18 mm) were consistently above these thresholds despite acute neuropathy [26]. This calls into question the clinical relevance of the observed changes and highlights the limitations of the tuning fork test, which is highly dependent on the examiner. More objective methods, such as multi-frequency vibrometry or biothesiometry, could prove to be more precise [27]. Early pilot data also suggest that standardized vibratory approaches could improve measurement accuracy and have therapeutic potential [28].
These findings are supported by previous publications demonstrating beneficial effects of sensorimotor and vibration-based exercise on upper-extremity sensory function and patient-reported outcomes [8, 13, 14, 21]. The above findings emphasize the need for future interventional studies for both extremities to improve understanding of the impact of therapy-related PNP on patients’ daily lives. From a clinical perspective, the timing of such interventions also appears to be important: exercise may be beneficial during active therapy when neuropathic damage occurs, as well as during the rehabilitation phase. Early, targeted exercise may help slow down the progression of symptoms or support partial recovery [5], which highlights the importance of integrating structured physical interventions into cancer treatment.
Limitations
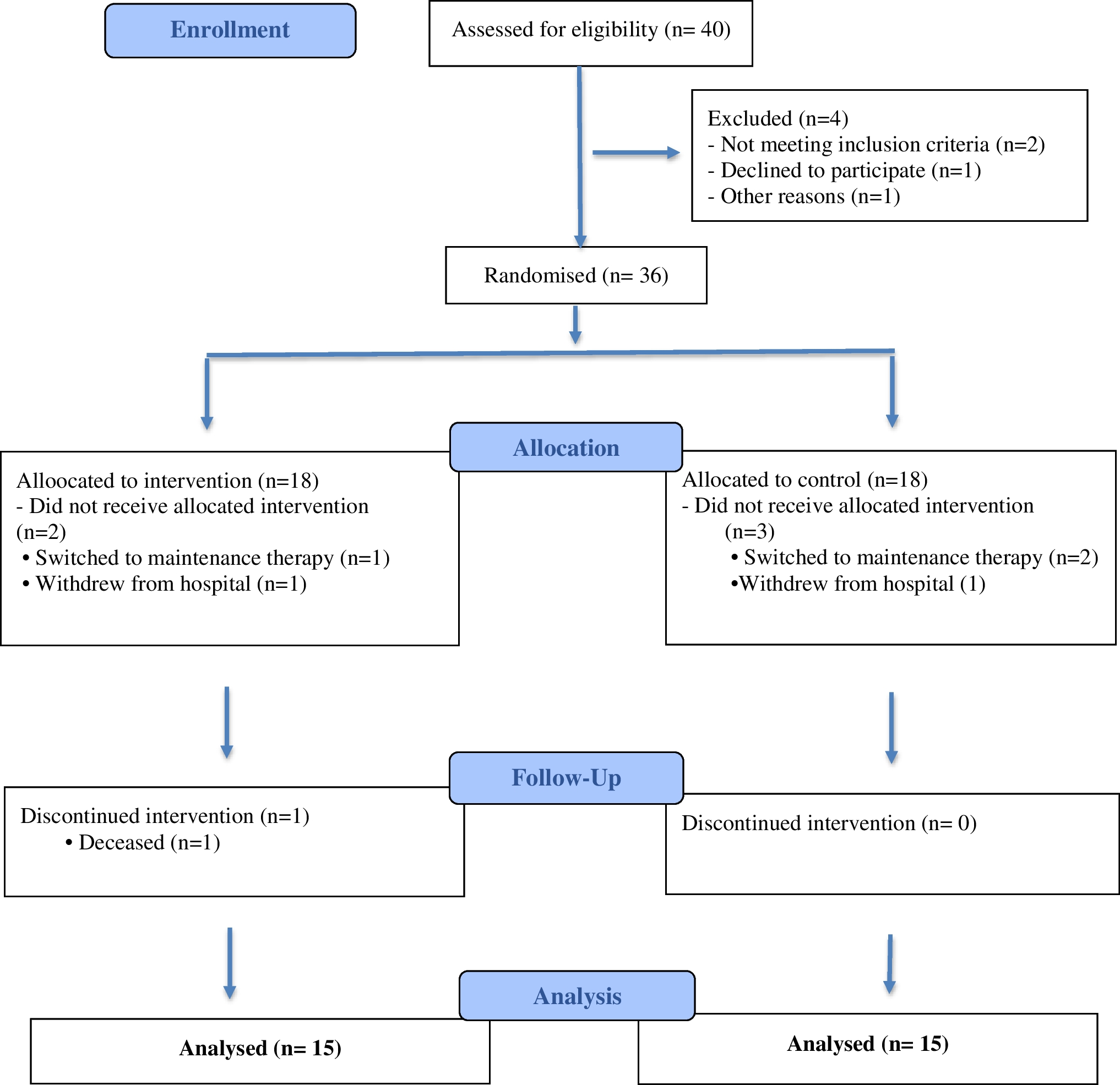
Several limitations should be taken into account when interpreting these results. Firstly, the relatively small sample size reduced statistical power and may limit the generalizability of the findings. Secondly, information on previous therapies was incomplete for some patients, meaning potential influencing factors could not be controlled in all cases. Thirdly, drug dosage was not fully standardized or consistently documented, so some degree of variability in treatment exposure and potential influence on the results cannot be ruled out. Additionally, the relatively short intervention and observation periods, which were partially non-overlapping, limited the ability to assess the potential long-term effects of the drug therapy [25]. Consequently, potentially relevant developments outside the study window were not considered. Most dropouts were related to disease progression or death rather than intervention-related factors; however, the absence of a formal comparison between completers and non-completers limits conclusions regarding potential attrition bias. The primary responder analysis used the FACT/GOG-Ntx, which assesses CIPN in both the upper and lower extremities. While this captures relevant functional impairment, it does not exclusively measure symptoms in the upper extremities. Finally, the patient recruitment, program implementation, and data collection were complicated by the COVID-19 pandemic restrictions, which did not lead to critical protocol deviations that would substantially bias the interpretation of the results.




Comments (0)