Trial design
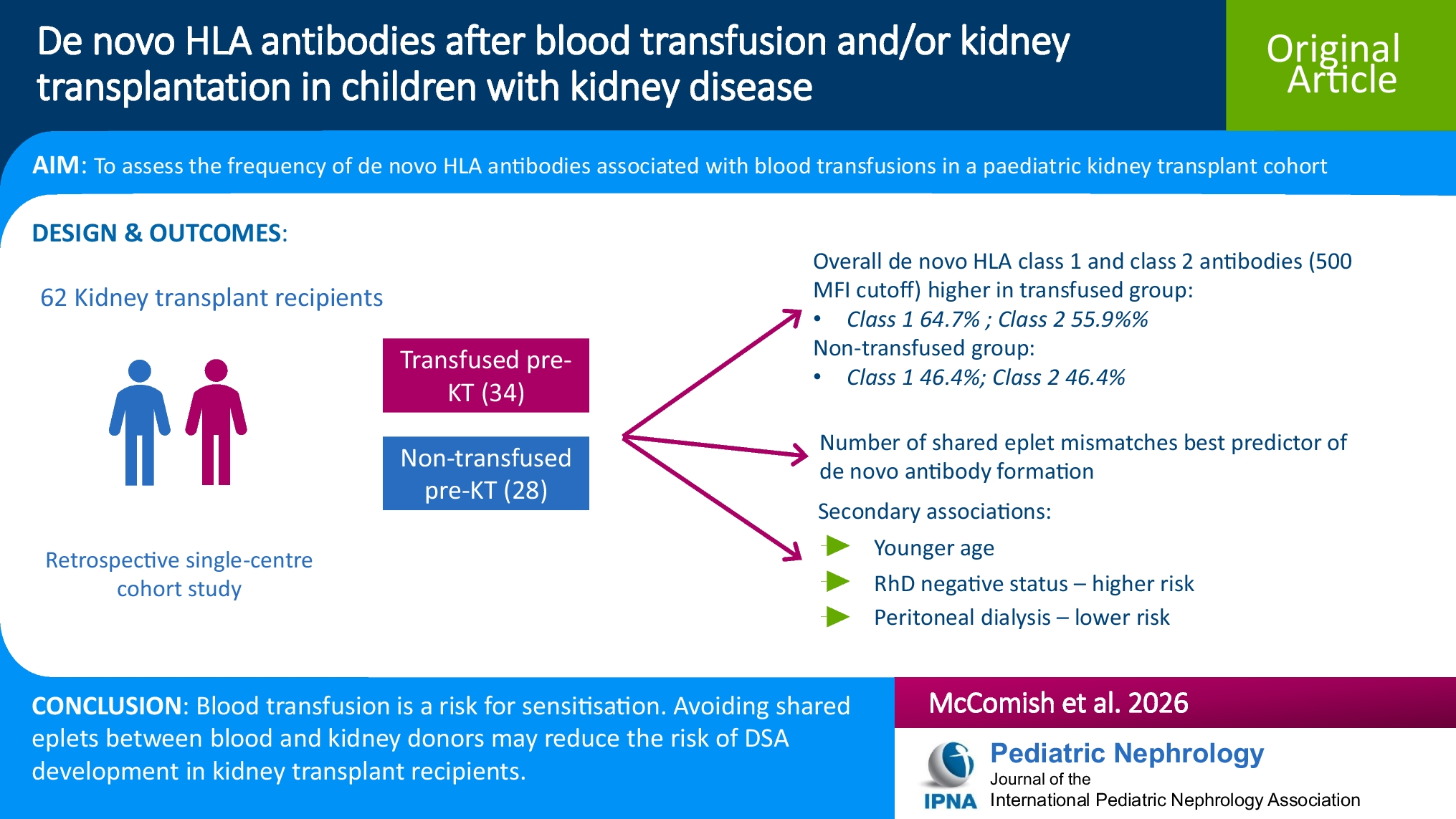
This retrospective, single-centre cohort study was conducted at the Royal Children’s Hospital (RCH), a tertiary care hospital in Melbourne, Australia. The study was approved by the RCH Human Research Ethics Committee (HREC) (reference number QA/54205/RCHM-2019), and by the Australian Red Cross Lifeblood HREC (reference number 2017#23).
Participant selection
The study included patients aged less than 19 years who received blood product transfusions under the nephrology unit at RCH between 2000 and 2018. Patients were excluded if they received platelets or if they did not have existing HLA antibody test results or stored serum for the relevant time points (pre-transfusion and at least 4 weeks post-transfusion). Only the first eligible transfusion event (defined as one or more red cell transfusions occurring between two serum sample dates, with the last unit transfused at least 4 weeks before the post-transfusion sample) was analysed for each patient. For all recorded transfusions, blood donor HLA typing information was collected if available. Where HLA typing of all blood donors was not available, participants were included where a de novo donor specific antibody (DSA) to a typed donor was identified or if results were negative, but excluded if the patient was transplanted prior to the post-transfusion sample, and a clear positive de novo result could not be attributed to a typed blood donor, as attribution of the HLA antibodies to bDSA or non-bDSA in these cases was not possible. Analyses comparing bDSA and kDSA were performed with and without the included patients with incomplete donor typing.
A control group from the same broad cohort (patients of the RCH nephrology unit between 2000 and 2018), comprising patients who received kidney transplants but no transfusions, was also included to compare the effect of transfusion and transplant versus transplant alone. For this group, two serum samples at least 4 weeks apart, with at least one post-transplant, were required.
Data collection
Clinical data were extracted from the electronic medical record (EMR) and included details of dialysis, transfusion indications, medications, infections, clinical observations and hospital laboratory test results (including full blood count, liver and kidney function, inflammatory markers and any microbiology results). Post-transplant outcomes, such as rejection and graft and patient survival, were also extracted.
Transfusion data, including blood donor data, were extracted from RCH Blood Bank records and correlated to Australian Red Cross Lifeblood records. HLA typing and antibody data were collected from Victorian Transplantation and Immunogenetics Service (VTIS) at Australian Red Cross Lifeblood. Where additional blood donor typing or antibody testing was required, it was performed at VTIS.
Data were managed using the REDCap electronic data capture tools hosted at Australian Red Cross Lifeblood [16, 17].
Outcomes
The primary outcome was the incidence proportion of de novo bDSA (HLA antibodies specific to one or more blood donors and present in the post-transfusion sample but not the pre-transfusion sample). Secondary outcomes assessed included the incidence proportion of non-bDSA (HLA antibodies specific to no blood donors and present in the post-transfusion sample but not the pre-transfusion sample) and the incidence proportion of overall HLA antibodies.
In addition, demographic, clinical and laboratory data were collected for a risk factor analysis as predictors of the primary outcome. Eplet analysis was also performed to identify exposure variables relating to blood and/or kidney donor mismatch that could predict the primary outcome.
For the purposes of analysis, HLA antibodies were distinguished as follows: bDSA, antibodies specific to one or more blood donors; kDSA, antibodies specific to one or more transplant donors; unspecified HLA antibodies, antibodies not specific to any known transfusion or transplant donor; and overall de novo HLA antibodies, the combination of the above categories.
Measures to reduce bias
To reduce bias, the study included all patients transfused during the study period, selecting based only on sample availability, antibody results and donor HLA typing, and avoiding duplicates. The control group comprised non-transfused transplanted patients from the same cohort. Factors influencing the need for transfusion in these groups (including age, underlying disease and intercurrent illness) comprise a possible source of residual bias.
Laboratory methods
For all patients, HLA class 1 and class 2 antibodies were detected and identified using the LabScreen single antigen bead (SAB) assay (One Lambda, Thermo Fisher Scientific, USA). Where the initial results were difficult to interpret or performed by an older method (enzyme-linked immunosorbent assay, ELISA), and stored serum was available, the stored serum was retested. The laboratory uses multiple factors to interpret HLA antibody results, including a range of threshold mean fluorescence intensity (MFI) cutoffs, of which the lowest is 500. Analyses were performed at MFIs of 500, 2000 and 8000, with the MFI 500 cutoff generally selected to maximise sensitivity. As per standard laboratory practice, the analysis was adjusted for beads known to be frequently positive in the absence of known HLA antibodies, and for common epitopes across multiple beads. HLA antibodies that were present in the second sample but not the first were considered de novo.
HLA typing was performed at HLA-A, B, C, DR and DQ loci using LabType (One Lambda, Inc., Thermo Fisher Scientific Inc., Canoga Park, California) or next-generation sequencing by MIA FORA (Immucor, Werfen Inc., Barcelona, Spain) or AllType/AllType FASTplex (One Lambda Inc.), on Illumina MiSeq and Illumina MiniSeq (Illumina Inc., San Diego, California).
Eplet analysis
Eplet analysis was performed using patient, blood donor and organ donor HLA typing data with the HLAMatchmaker 1000 pair program (ABC + DRDQDP Eplet, version 3.1, 2020, www.epitopes.net) and HLA Fusion software (One Lambda, Thermo Fisher Scientific, USA). Where two-field typing was unavailable for an HLA locus, typing was imputed based on linkages in the local population in-house database.
The eplet mismatch load is the number of unique eplets that are present on the donor HLA but absent on the patient HLA. The analysis compared eplet mismatch loads for patients with both blood and kidney donors, including shared and separate eplet mismatches.
Statistical analysis
Categorical data were described using absolute and relative frequencies. Numerical data were found to be skewed and are described using median, inter-quartile range (IQR), and range. Cumulative incidences of bDSA and non-bDSA were calculated for MFI positivity cutoffs 500, 2000 and 8000 and are presented together with unadjusted two-sided exact binomial Clopper-Pearson 95% confidence intervals (95% CI).
Differences in the distribution of potential risk factors between patients with and patients without incident HLA class 1 or class 2 bDSA, non-bDSA and bDSA or non-bDSA were assessed using Fisher’s exact tests and Wilcoxon rank sum tests. Multivariable logistic regression analyses were used to adjust for the confounding effects of age, which was identified as statistically significant in bivariate analysis.
Further, associations between clinical factors associated with the transplant (graft function, causes of graft failure including rejection episodes and chronic rejection, immunosuppressive treatment, transplant nephrectomy, peritonitis and patient survival) and prevalent (i.e. present in the initial sample) HLA class 1 or class 2 bDSA, non-bDSA and overall HLA antibodies, as well as HLA class 1 and class 2 eplet mismatch, were assessed using Fisher’s exact tests. Positive HLA antibody results that were not associated with a known blood donor, but with incomplete donor typing information, were classified as indeterminate. Indeterminate results for de novo and prevalent bDSA and non-bDSA were excluded from the analysis where the categories were analysed separately but were retained for analysis of overall HLA antibodies (which does not require knowledge of donor typing).
For the eplet analysis, statistical comparisons between patients with de novo HLA class 1 as well as HLA class 2 bDSA (positivity cutoffs 500, 2000 and 8000, respectively) and those without were conducted using non-parametric Mann–Whitney U test and binary logistic regression analysis. Factors investigated included HLA class 1 and class 2 eplet mismatch loads for transfusion donor only, transplant donor only and shared mismatches (mismatched eplets present in both transfusion and transplant donors), as well as total eplet mismatch loads for transfusion and for transplant donors. These analyses were performed assuming indeterminate results for incident bDSA antibodies to be negative. Logistic regression analysis was used to adjust for the time passed between kidney transplant and final sampling dates as well as for the number of red cell units transfused (to account for confounding effects of elapsed time and total antigen load as compared to degree of mismatch). Similar analyses were conducted comparing patients with de novo HLA class 1 as well as HLA class 2 kDSA (kDSA only, shared eplet kDSA/bDSA and separate eplet kDSA/bDSA) to patients without these antibodies, with respect to shared and total transfusion eplet mismatch loads. The associations between HLA class 1 and class 2 bDSA/kDSA (MFI cutoff 500 and 2000) and the respective HLA class 1 and class 2 eplet mismatch loads for transfusion only, transplant only and shared, as well as for total transfusion and total transplant loads, were investigated using non-parametric Kruskal–Wallis tests.
Estimations of the variance in total bDSA that can be explained by total transplant eplet mismatch loads were based on pseudo R-squared results from respective logistic regression models. Analyses were conducted for patients with all or partially typed red cell units, combined and separately. Cases with no kidney transplant and/or with no blood donor typing were excluded (n = 7).
Analysis was conducted using Stata, version 12 (College Station, TX, USA).


Comments (0)