
Remember me




AVPEPs arising in the setting of keratinizing DOCs are rare lesions with only N = 11 previous examples reported in the English literature (Table 1) [14, 16,17,18,19,20,21,22,23,24,25]. When the current case is also considered, 10 (83.3%) affected men and 2 (16.7%) women (M:F ratio = 5:1) with a mean age of 50.5 years (age range = 13–76 years). A predilection for the maxilla was noted (8 of 12, 66.7%) with only 4 cases involving the mandible. The anterior and posterior portions of the jaws were equally affected. Accompanying clinical findings included symptomatic or painless, expansile, intraosseous lesions with occasional overlying mucosal involvement, cutaneous or intraoral sinus tracts (fistulas) [16, 17, 21] and an average duration of 39.4 months (range 6–96 months). Radiographically, most lesions presented as well-defined, unilocular or multilocular radiolucencies, with or without cortical thinning and perforation, and an average size of 3.4 cm (range 2.0–8.3 cm). A single lesion was described as radiopaque and extended into the maxillary sinus [24]. Infrequent complications include tooth mobility [17], trismus [21] and lower lip/chin paresthesia [23].
Table 1 Clinicoepidemiologic characteristics of previously reported intraosseous atypical verrucopapillary epithelial proliferations arising from odontogenic cystic lesionsThe histopathologic spectrum of AVPEPs evolving from the epithelial lining of DOCs is broad and may include a markedly acanthotic, hyperplastic epithelium with hypergranulosis, hyperortho- or parakeratosis, together with a verrucous or papillary architecture and inconspicuous to pronounced cytologic atypia [14, 23, 25]. More frequently, however, AVPEPs ex-DOC demonstrate features akin to VC of surface epithelial origin [16,17,18,19,20,21,22, 24], as also seen in the present case. Such VC-like cystic lesions of the jawbones show exuberant luminal keratin production with keratin plug formation, as well as elongated, bulbous and broad rete ridges “pushing” into the fibrous cyst wall. Cytologic atypia, when present, is usually limited to the basal/suprabasilar layers. Koilocyte-like features, i.e., keratinocytes with pyknotic nuclei and clear perinuclear halo, although present, does not correlate with HPV infection, as confirmed by negative HPV PCR testing and patchy p16 immunoreactivity [14, 15]. Notably, tautochronous occurrence of AVPEP and intraosseous SCC evolving from a DOC has also been documented [22].
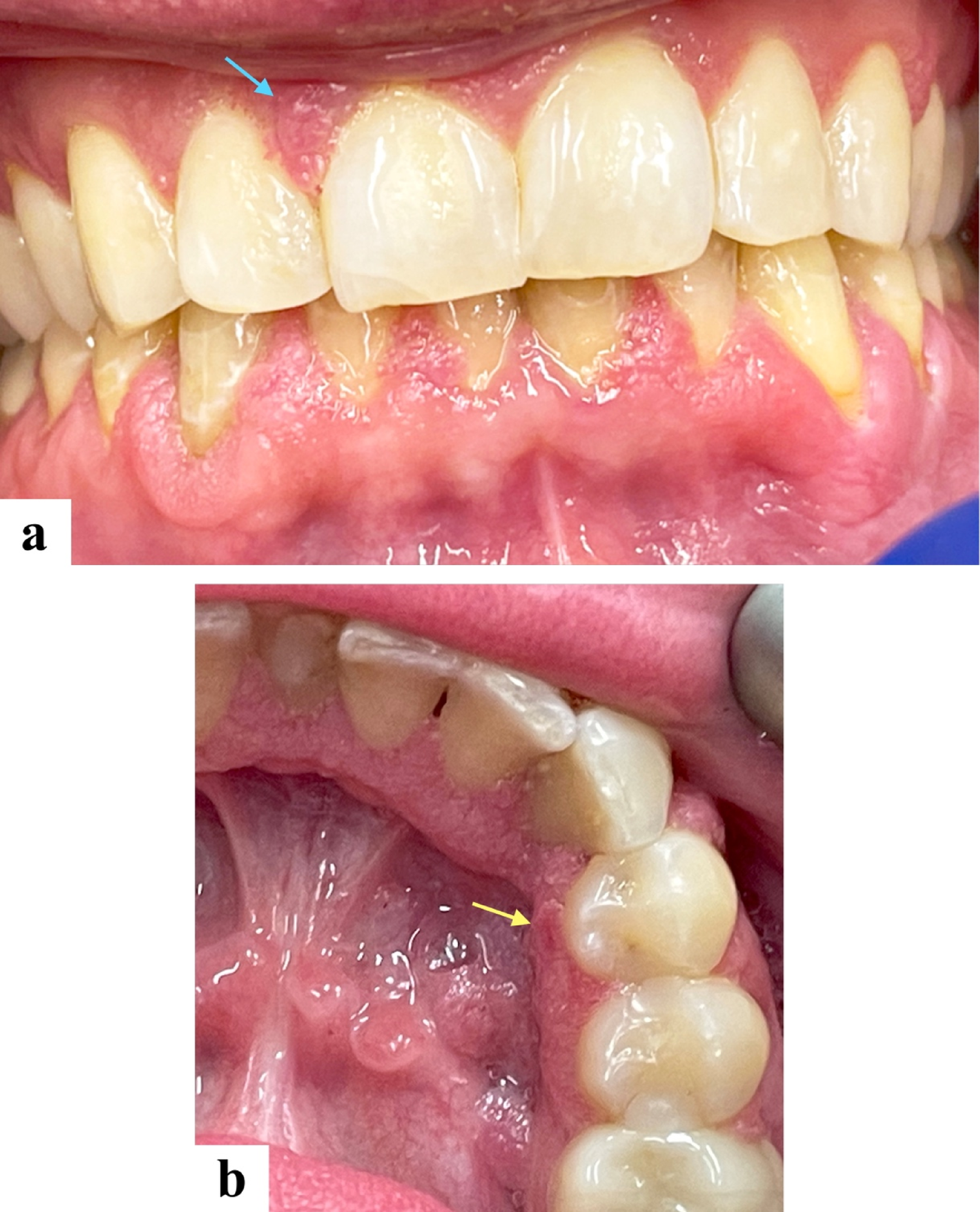
Two main differential diagnoses necessitate attention when an intraosseous cystic AVPEP ex-DOC is considered. Odontogenic cysts with a verrucoid pattern should be distinguished from proliferative verrucous leukoplakic lesions that have infiltrated the periodontal ligament space extending into the alveolar bone proper and causing cyst-like saucerization of the bone (Fig. 3A–C) [13]. Such lesions can be clinically and even microscopically misinterpreted as AVPEPs arising from an intraosseous odontogenic cyst (Fig. 3B, C). A useful diagnostic feature, however, is the presence of clinically detectable marginal linear gingival leukoplakia usually in the form of a “ring around the collar” of involved teeth [26, 27]. Additionally, well-differentiated cystic SCC, including carcinoma cuniculatum, can masquerade as a jawbone DOC with luminal keratinization, particularly in incisional or small biopsy specimens [28, 29]. Notably, thorough microscopic examination of the entirely submitted specimen of AVPEP, including VC, arising in the lining of a DOC is mandatory to exclude the tautochronous presence of conventional SCC.
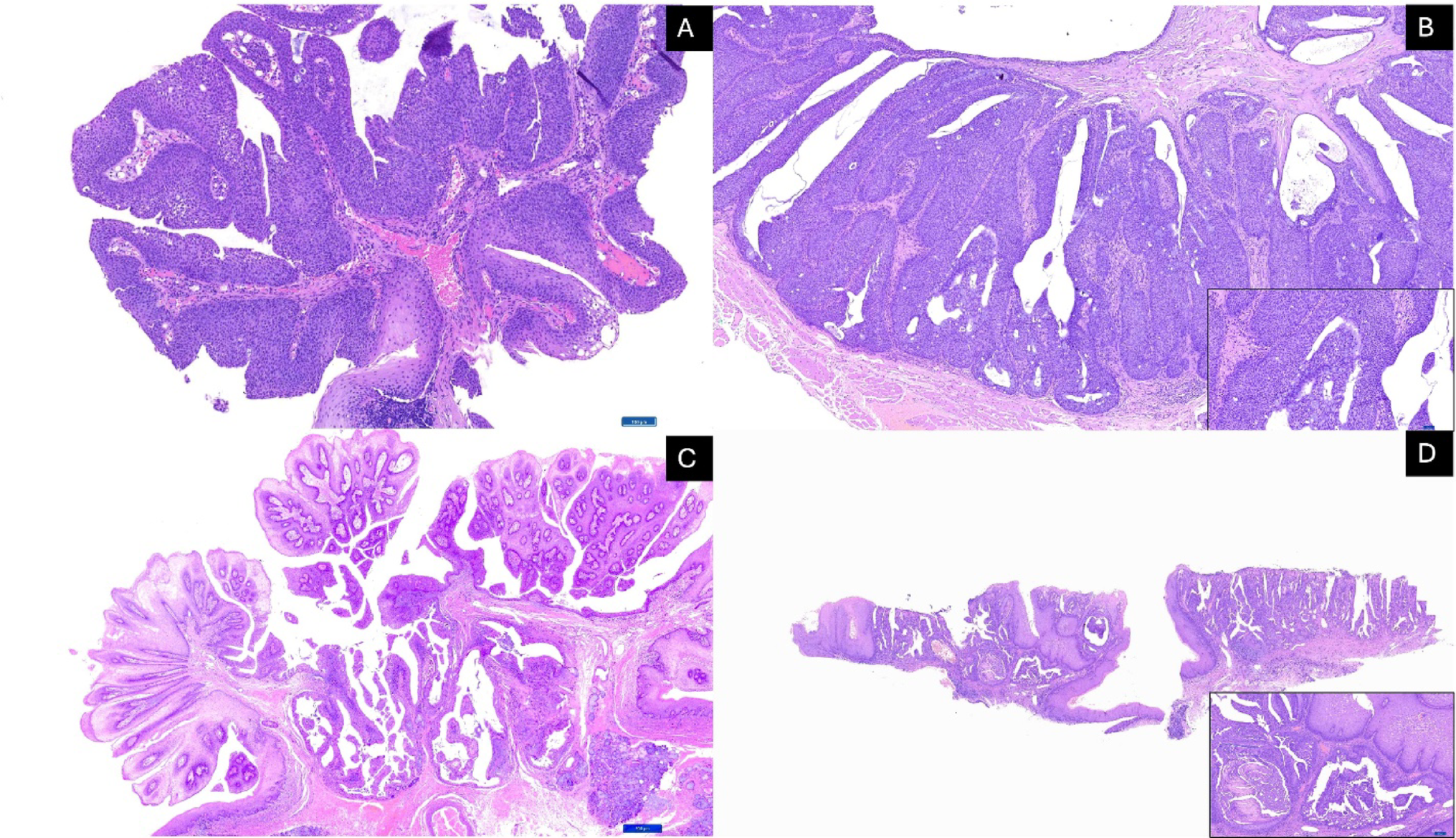
Fig. 3
A Gross images of proliferative verrucous leukoplakia lesion infiltrating the periodontal ligament space (PDL) and extending into the underlying alveolar bone at the root bifurcation of this mandibular molar tooth; B, C Histologic characteristics of proliferative verrucous leukoplakia involving the PDL space comprising an atypical epithelial proliferation with verrucoid architecture, prominent parakeratin production and clefting, together with cytologic aberrations (Images courtesy of Dr. Ioannis Koutlas, DDS, MS, University of Minnesota)
Carcinoma cuniculatum deserves special mention due to its, overall, bland cytomorphology and overlapping clinical and histologic characteristics with AVPEPs developing in the setting of DOCs. Carcinoma cuniculatum demonstrates a strong predilection for the jawbones (Fig. 4A) and a predominantly endophytic growth pattern comprising a burrowing labyrinthine network of well-differentiated squamous epithelium forming interconnecting keratin-filled crypts invading the underlying bone (Fig. 4B, C) [28, 30,31,32,33]. As a result, microsequestra are frequently present. The epithelial crypts display exuberant amounts of exfoliated keratin in association with neutrophilic microabscesses (Fig. 4C). Similar to this case of atypical VC-like proliferation evolving from a DOC, epithelial dysplasia is at most mild in carcinoma cuniculatum of the jawbones (Fig. 4D) and a verrucopapillary architecture may be, at least focally, identified (Fig. 4C). In contrast to keratinizing odontogenic cysts with verrucous features, carcinoma cuniculatum is characterized by multiple, infiltrative, cyst-like crypts, as well as architectural and/or cytologic aberrations of the overlying mucosal epithelium (Fig. 4B). However, these two diagnostically helpful findings may not be identified owing to non-representative tissue sampling.
Fig. 4
A Clinical presentation of carcinoma cuniculatum involving the maxilla, as well as maxillary alveolar and labial mucosa causing buccal and palatal cortical expansion and superficial telangiectasia; B, C Low-power photomicrographs showing an endophytic growth pattern comprising a burrowing network of well-differentiated squamous epithelium forming interconnecting keratin-filled crypts with exuberant amounts of exfoliated keratin and neutrophilic microabscesses; D Cytologic atypia in carcinoma cuniculatum is at most mild
Treatment of the AVPEPs in the setting of DOCs has varied greatly (Table 1). Eight (66.7%) patients, including the current case, were treated conservatively, i.e., surgical excision, enucleation, or curettage, while 4 (33.3%) received radical surgical resection and one of them additional neck dissection [19]. The single case of VC with tautochronous SCC arising from the epithelial lining of an OKC was treated with curettage followed by partial maxillectomy and nasal septectomy [22]. Loco-regional recurrence was reported in only 1 of 12 (8.3%) patients within 7 months after enucleation [23]. The remaining 11 patients (91.7%) with AVPEP evolving from a DOC showed no evidence of disease after a mean follow-up period of 24.2 months (range = 5–66 months), notwithstanding conservative therapeutic regimens in most cases. Given the favorable prognosis with conservative therapy, extensive resection should be reserved for recurrent or locally aggressive lesions, or when a synchronous SCC component is identified.
Comments (0)