
Remember me

This is a prospective randomized controlled study performed in a single center, between 2022 and 2025, in Cairo, Egypt. Ethical approval #N-159-2025 was obtained from the Research Ethics Board, Kasr El Aini Faculty of Medicine, Cairo University, Egypt. All methods were performed in accordance with the relevant guidelines and regulations. Thorough patient counseling was performed, explaining the nature of surgery and its possible outcomes. Surgical steps were illustrated, particularly the different methods of corporotomy closure including SCCT, with the pros and cons of each. The advantages of SCCT were explained, as well as the possible disadvantage, namely the use of needle suturing with risk of device failure – though mitigated- and the longer operative time. Written informed consent was obtained from all participants.
iPP implantation was performed for 32 patients with erectile dysfunction refractory to medical treatment. Patients had full history taking including demographic data (age, relationship status, fertility status, ethnicity, contact information), general medical history and sexual history including types and outcome of previously-tried treatment modalities for ED, general and local examination, review of previously done investigations for ED, pre-operative investigations and anesthesia review. Exclusion criteria included patients who had previous penile surgery, Peyronie’s disease, history of priapism, corporal fibrosis or radical prostatectomy, patients with a requirement for ancillary procedures, or those receiving anticoagulant therapy.
Patients were randomized into two groups, using a computerized randomization generator, with allocation blinded to the surgical team. Control Group had the corporotomies closed by tying the pre-placed stay sutures. SCCT Group had the corporotomy edges everted with pre-placed horizontal mattress sutures, then sutured closed.
Operative detailsSurgery was performed through the peno-scrotal incision. Dartos and Buck’s layers were dissected down to the corpora cavernosa. For the Control Group, four stay sutures were pre-placed using 2/0 Polyglactin suture material, one on each side of the intended corporotomy sites. Each stay suture was placed in a W-shape, ending in four suture limbs on each side of the intended corporotomies. Corporotomies were cut open. The corpora were dilated, measured, and cylinders were implanted. Corporotomies were closed by tying-over the stay sutures, over the iPP cylinders.
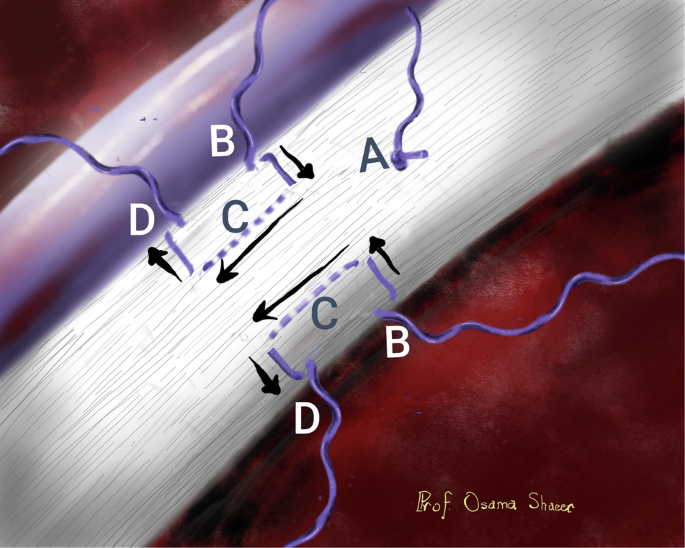
For SCCT Group the following steps were performed: A stay suture was placed at the upper angle of the intended corporotomy (Fig. 1-A). This was pulled upon to pull the tunica albuginea of the crura out, for a proximally-placed corporotomy. It would serve other purposes as will be demonstrated further on.
Fig. 1: Laying-in the stay sutures.
A Upper angle stay suture. B First arm of the everting suture, perpendicular to and towards the intended corporotomy (C) Secomd arm of the everting suture, parallel to and along the line of the intended corporotomy. D Third arm of the everting suture, perpendicular to and away from the intended corporotomy.
Four horizontal mattress sutures were placed on each side of the intended corporotomy, two on each corpus cavernosum. This was performed as follows: Starting with the medial mattress suture, a 2/0 Polyglactin suture line was passed into the tunica albuginea close to the spongiosum, from medial to lateral, in then out (Fig. 1-B). The suture was then passed parallel to and along the line of the intended corporotomy, half a centimeter laterally, in then out (Fig. 1-C). This was completed by passing the suture line back, from lateral to medial, in and out of the tunica, along the line of the first entry point (Fig. 1-D). This was repeated as a mirror image on the other side of the intended corporotomy on the same side. Then a similar pair was placed on the contralateral corpus cavernosum.
The corporotomies were cut. The horizontal mattress stay sutures were then tied on either sides of the corporotomies, everting the edges. For each knot, one of the two suture ends was cut, and the other kept to pull on the corporotomy edge (Fig. 2).
Fig. 2
Everting sutures tied, corporotomy cut and everted.
The corpora were dilated, measured, and cylinders were implanted. Upon implantation, the stay suture at the upper angle was pulled upwards to lift-up that angle, allowing easier insertion of the distal tip of the cylinder, however short the corporotomy was. The everted corporotomy edges were then sutured closed in a running fashion (Figs. 3, 4), starting from the proximal end adjacent to the tubes, proceeding distally towards the stay suture at the upper angle. We mostly ran the suture line loose, and pulled it taught once the upper angle was reached. The running suture line was tied to the upper angle suture. Once the corporotomies were closed, the stay sutures were cut, and the stump pulled out unless deemed difficult. Video of the technique can be viewed at the Video Journal of Sexual Medicine [8].
Fig. 3
Suturing the everted corporotomy edges.
Fig. 4
Corporotomy closed by a running suture line, before the everting stay sutures are removed.
For both groups, the reservoir was inserted in a high submuscular position, and the pump was inserted in an anterior position. Submuscular reservoir placement was the surgeon’s and patient’s choice rather than a part of the technique at hand. The implant tubes were connected and cycling was performed. Suction drain was inserted. Buck’s fascia, Dartos and skin were closed. Mummy wrap was applied. Cylinders were left semi-inflated for one week. The drain was removed once drain output was less than 20 cc’s, and the drain tube was empty, not before 24 h, and no later than three days in any case. Cycling started by the third week.
Operative time, drain output, complications and device malfunction were recorded and compared across the two groups. We applied out regular follow up protocol to this patient cohort: Patients were followed up at the hospital on days 1, 2 and 6, then by clinic visits at day 7, 21 and day 40, then at 3 and 6 months post-operative, and by phone interviews every 6 months for the first 2 years, and an annual phone call every year thereafter. Phone interviews included a general question on satisfaction with rigidity on a 5-point scale, any change in ability to inflate and deflate the implant, and de-novo pain or deformity.
Statistical analysis was performed using Microsoft Excel 365. Results were represented as range, mean and standard deviation. Statistical significance was calculated using Student T-Test. P-Value of 0.05 or lower was considered statistically significant.
Comments (0)