The reported prevalence of IC/BPS in the general population ranges from 0.45 to 12.6%, with a higher predominance in middle-aged and elderly women. The global incidence in females is estimated at approximately 52–500 per 100,000 person-years, while the incidence in males has shown an increasing trend, with a reported female-to-male ratio ranging from 5:1 to 10:1. Available evidence suggests that male patients with IC/BPS may have a higher likelihood of tumor-related diagnoses compared with female patients [4]. In our cohort of 863 patients (248 males and 615 females), the proportion of tumor-related diagnoses identified during the diagnostic course of IC/BPS was approximately 6.04% among males and 1.62% among females. However, due to the lack of large-scale epidemiological data on IC/BPS in China, further external validation is still needed.
Currently, there is no definitive evidence demonstrating a direct association between specific IC/BPS clinical phenotypes and the risk of bladder malignancy. Notably, 8/25 patients (32.0%) in our tumor-related cohort developed hematuria during the disease course, suggesting that hematuria—particularly new-onset or persistent hematuria—may serve as a warning sign warranting heightened vigilance. Importantly, the median interval from IC/BPS diagnosis to definitive tumor diagnosis was 12 months in patients diagnosed on repeat biopsy (Table 2), emphasizing the need for clinically driven follow-up and re-evaluation rather than reliance on a single assessment in selected high-risk scenarios. A recent Korean study involving 646 patients with suspected IC/BPS demonstrated that no single diagnostic modality is sufficient to completely exclude urinary tract malignancy or tuberculosis, and that combined evaluation using imaging, urine tests, and cystoscopy is required [5].
With respect to imaging, previous studies have shown that ultrasonography and computed tomography (CT) have limited diagnostic value in differentiating IC/BPS from bladder tumors [5]. Diffusion-weighted magnetic resonance imaging (DWI-MRI) has been reported to have potential diagnostic value; however, both sensitivity and specificity remain suboptimal [6]. Our results further support the notion that imaging alone is insufficient to reliably exclude bladder tumors, while the actual clinical utilization rate of advanced imaging remains relatively low.
Cystoscopic findings in our cohort demonstrated marked heterogeneity. Some patients showed tumor-like mucosal abnormalities, such as papillary changes, focal mucosal elevations, or friable bleeding lesions, whereas others predominantly exhibited inflammatory features including diffuse mucosal hyperemia, edema, punctate hemorrhages, and pale mucosa without exophytic tumor-like morphology. These findings suggest that chronic inflammatory changes of the bladder mucosa in the context of IC/BPS may obscure early neoplastic lesions, thus increasing the risk of false-negative endoscopic assessment.
Random multi-site biopsies are not routinely performed in many centers for all IC/BPS evaluations. In the 2025 CUA guideline, cystoscopy is emphasized to help exclude malignancy in patients with risk factors (e.g., hematuria) and to identify Hunner lesions, and bladder biopsy is recommended when malignancy is suspected [19]. In our referral setting, the diagnostic overlap between IC/BPS-related inflammatory changes and early flat neoplasia (e.g., CIS/Tis) may reduce the sensitivity of purely visual, targeted sampling. This concern is supported by our observation that a subset of patients had non-specific inflammatory pathology on index biopsy but were diagnosed with malignancy on repeat biopsy. Therefore, we implemented a standardized protocol of multi-site sampling (with additional targeted biopsy of any suspicious areas) as a quality-control strategy to mitigate sampling error in selected patients. Importantly, we do not advocate indiscriminate repeat biopsies for all IC/BPS patients; surveillance and re-biopsy should be risk-stratified based on clinical and endoscopic risk signals.
Importantly, we observed heterogeneity in the timing of tumor detection. Some patients were diagnosed with bladder cancer at the time of the first cystoscopic biopsy, while others showed only chronic inflammation or nonspecific findings at the initial biopsy and were subsequently diagnosed with bladder cancer during repeat biopsies. Two potential mechanisms may explain this phenomenon. First, sampling limitations during the initial biopsy—especially in the setting of diffuse mucosal inflammation, hyperemia, and punctate bleeding—may lead to missed occult lesions. Second, the possibility of de novo tumor development during the interval between examinations (“interval bladder tumor”) cannot be excluded.
From a biological perspective, the chronic inflammatory microenvironment in IC/BPS may increase the risk of carcinogenesis through mechanisms involving oxidative stress, cumulative DNA damage, and abnormal cellular proliferation [7]. In addition, epithelial remodeling under chronic inflammatory conditions may further obscure early neoplastic morphological features, thereby reducing the diagnostic sensitivity of a single random biopsy. Therefore, a negative result from a single biopsy cannot be considered sufficient to exclude malignancy when clinical suspicion persists.
In this study, four patients were ultimately diagnosed with nephrogenic adenoma (NA). Although NA is regarded as a benign lesion, its clinical and radiological features may closely mimic those of malignant tumors, and its pathogenesis remains incompletely understood [8,9,10,11,12,13,14]. While definitive evidence of malignant transformation is lacking, sporadic case reports have suggested a potential association with malignancy [15, 16], indicating that its biological behavior warrants long-term surveillance. Based on the existing literature, NA should be considered a benign but potentially recurrent lesion that may clinically resemble malignancy, and a potential association with bladder neoplasia cannot be completely excluded [17].
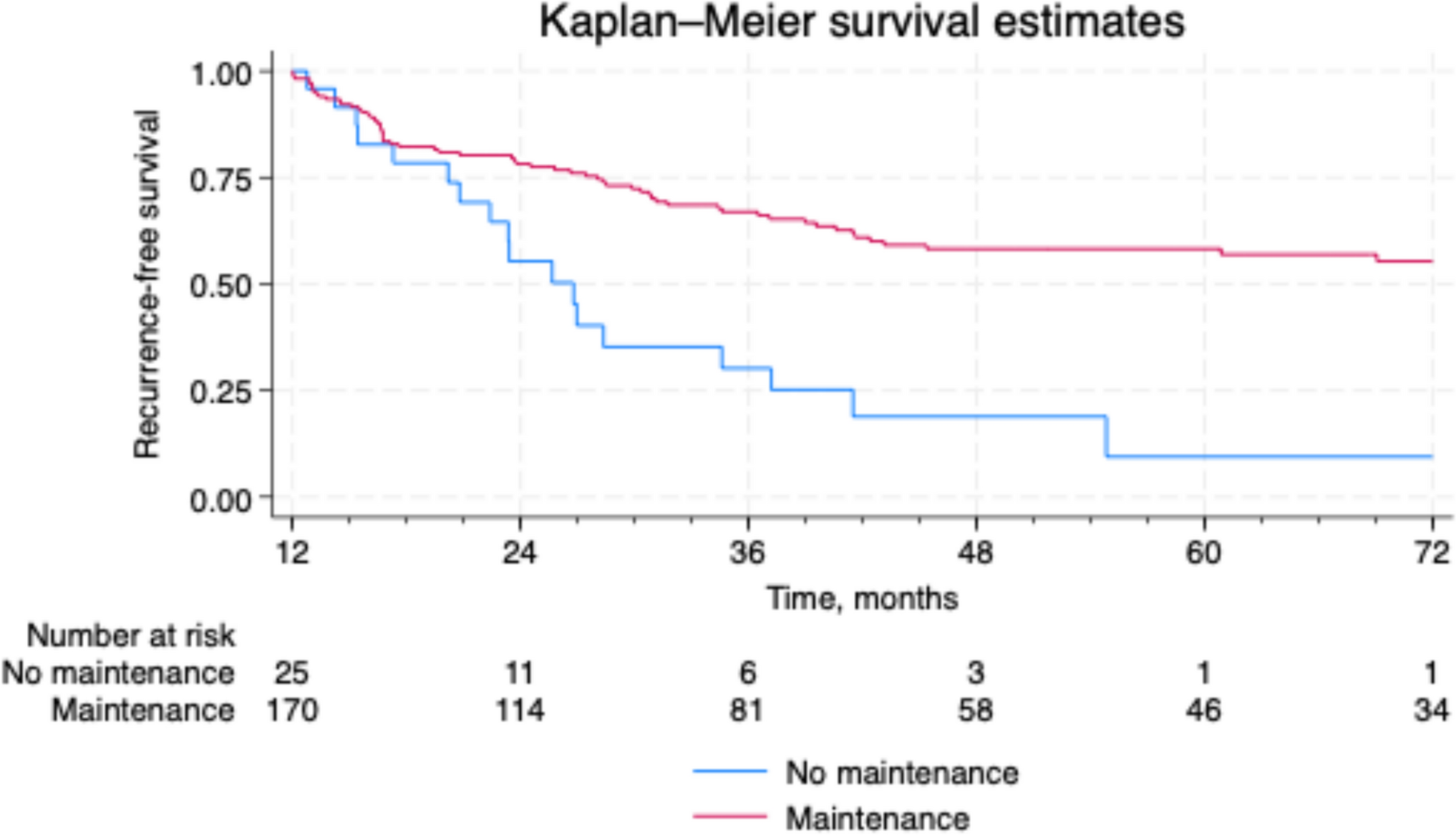
Interpretation of oncologic outcomes in our cohort should be cautious. Follow-up data were incomplete (20/25 patients), and the duration of follow-up was heterogeneous. Patients lost to follow-up may have experienced unrecorded recurrences, progression, or death outside our institution, which could bias our estimates toward a more favorable outcome. Therefore, our survival and recurrence findings should be regarded as descriptive rather than definitive. Compared with the natural history of urothelial carcinoma reported in the literature [18], our patients appeared to exhibit the characteristics of “high pathological grade but relatively early pathological stage at detection,” which may reflect intensive diagnostic evaluation in symptomatic patients rather than a distinct tumor biology. Accordingly, our findings suggest that bladder tumors detected in the context of IC/BPS represent a clinically challenging diagnostic scenario with substantial symptom overlap and inflammatory masking, rather than establishing a distinct biological entity. Molecular profiling and comparative cohorts are needed to determine whether these tumors differ biologically from conventional bladder cancer.
Current international guidelines recommend a stepwise, multimodal treatment strategy for IC/BPS, including behavioral therapy, physical therapy, pharmacological treatment, intravesical instillation, endoscopic interventions, botulinum toxin injection, and neuromodulation [1]. Based on our findings, we suggest that follow-up and re-evaluation for IC/BPS should be risk-stratified. In particular, intensified surveillance (repeat cystoscopy with targeted biopsy of suspicious areas, with or without repeat multi-site sampling) may be considered for patients with high-risk features, such as male sex, hematuria, cystoscopic abnormalities suggestive of neoplasia, suspicious imaging findings, or discordance between persistent/worsening symptoms and benign initial pathology, to facilitate timely detection while minimizing unnecessary procedures.
This study has several limitations. First, the retrospective single-center design introduces selection and referral bias, and the observed tumor-related diagnostic yield may not be generalizable. Second, diagnostic approaches, endoscopic technology, and pathological reporting practices may have evolved during the study period, introducing temporal heterogeneity despite efforts to maintain interpretive consistency. Third, because random biopsies sample only a fraction of the bladder mucosa, we cannot fully distinguish sampling error from true interval tumor development in patients diagnosed on repeat biopsy. Fourth, follow-up was incomplete and heterogeneous, limiting conclusions regarding recurrence and survival. Further multicenter, prospective studies are required to validate these findings, establish externally generalizable risk stratification, and optimize surveillance strategies.


Comments (0)