Cohort Selection
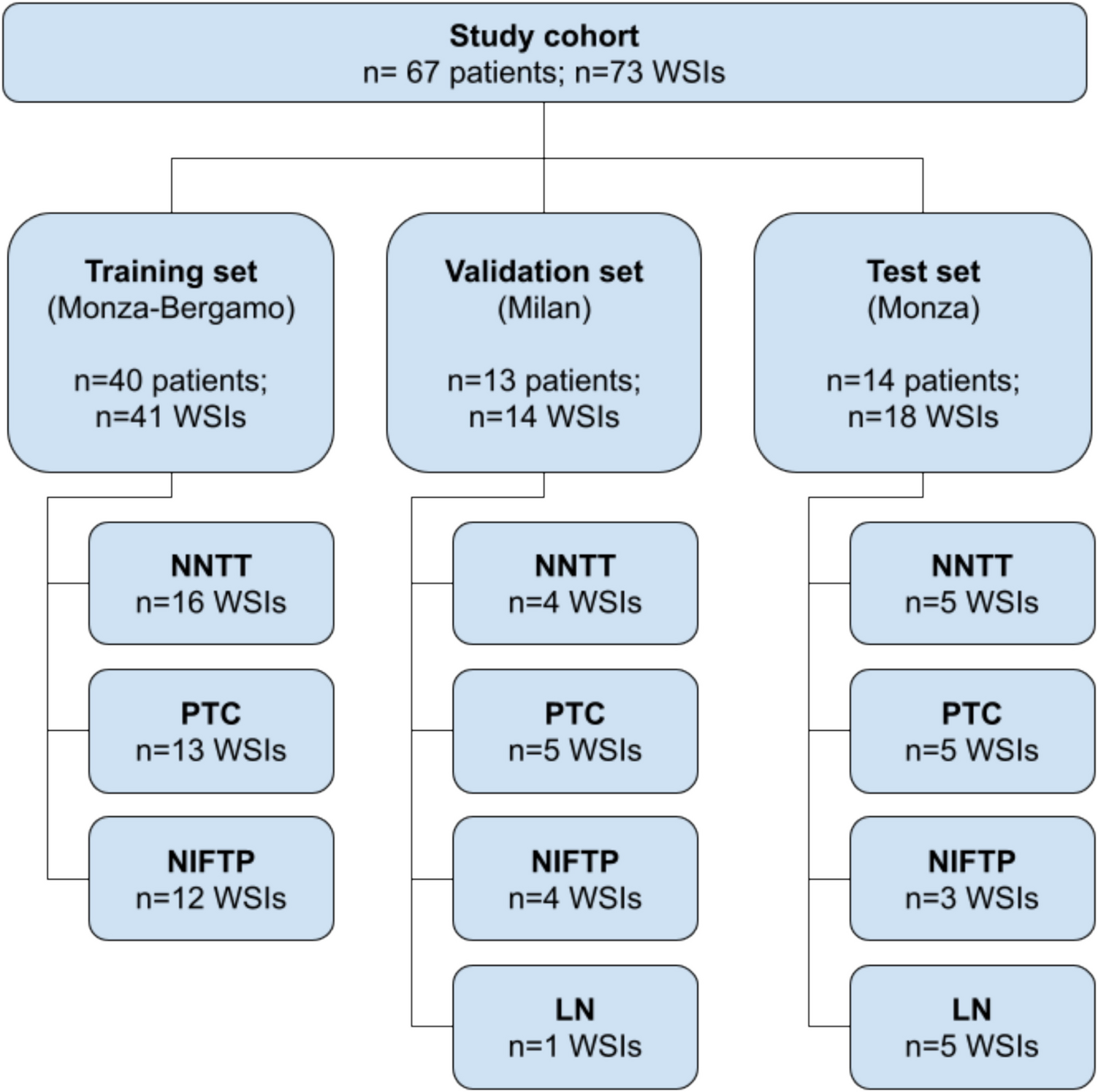
This multicenter retrospective study included patients with a histologically confirmed diagnosis of MTC. The inclusion criteria for patient selection were: (1) having undergone surgical treatment between years 2000 and 2024 and (2) availability of formalin-fixed paraffin-embedded (FFPE) blocks from the primary tumor. Patients were recruited from 5 centers across Europe: Hospital Universitario Ramón y Cajal (Madrid, Spain), Hospital Universitario La Princesa (Madrid, Spain), University Hospital Hradec Králové (Hradec Králové, Czech Republic), Ipatimup (Porto, Portugal), and ULS-Coimbra (Coimbra, Portugal). The study design is summarized in Supplementary Fig. 1.
Clinical and follow-up data were collected from medical records of all participating institutions. Disease-free survival (DFS) was defined as the time from the date of radical treatment to tumor relapse or death due to any cause, whichever occurred first. Overall survival (OS) was defined as the time from the date of treatment initiation to death due to any cause. Pathological parameters were collected at each center after reviewing the pathology reports and the available slides from each case. In cases where the proliferation index had not been assessed at the time of diagnosis, Ki-67 immunohistochemistry was subsequently performed to determine tumor grade. High-grade MTC was defined by ≥ 5 mitoses per 2 mm² and/or tumor necrosis and/or Ki-67 ≥ 5%, following the International Medullary Thyroid Carcinoma Grading Scheme [4].
The study was approved by the Hospital Universitario Ramón y Cajal Research Ethics Committee (approval code: 190/24) and was conducted in accordance with ethical standards of the Helsinki Declaration of the World Medical Association.
DLL3 Immunohistochemistry
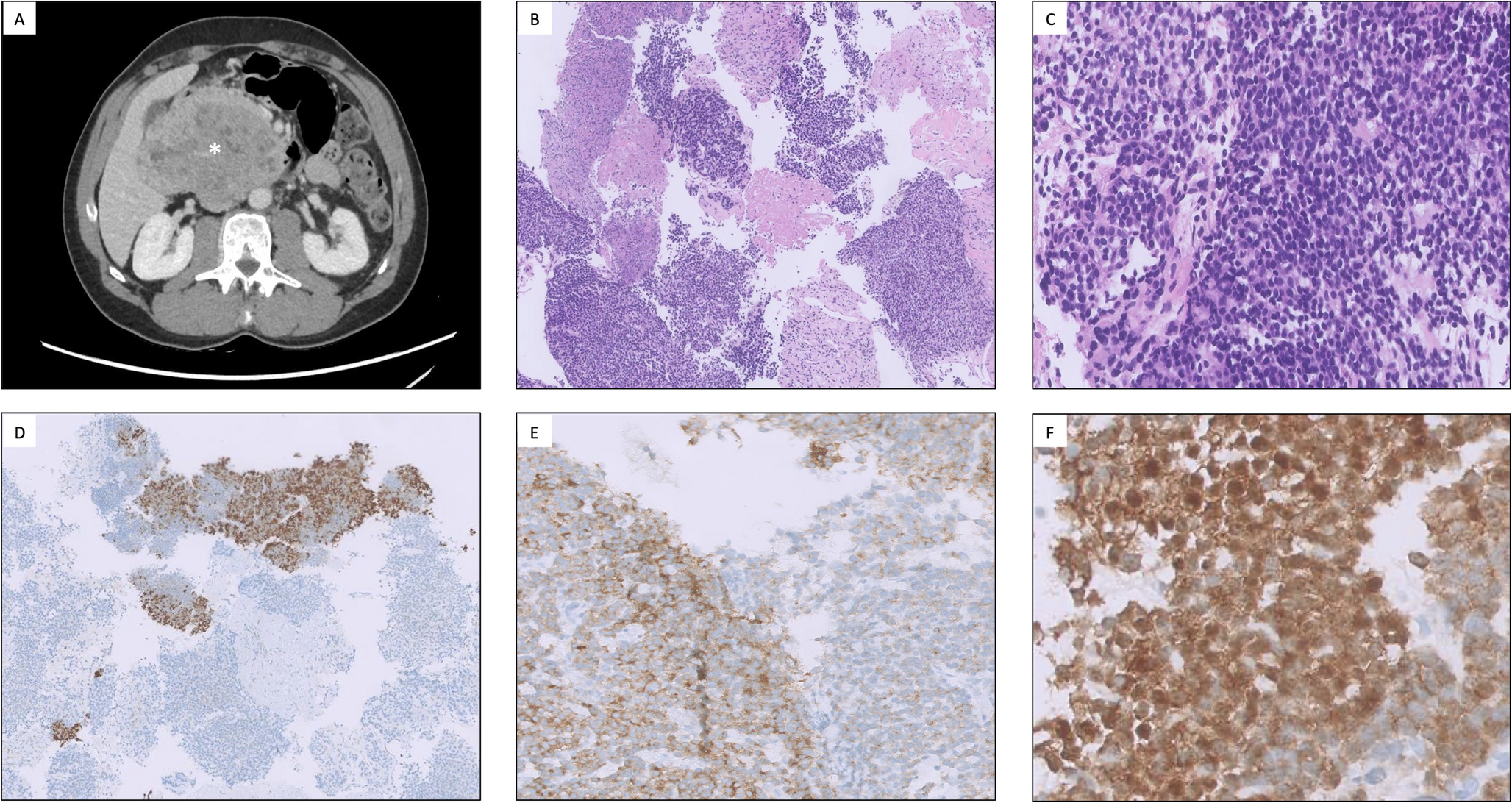
From each participating center, a representative FFPE tumor block was submitted to the central laboratory for centralized analysis. Immunohistochemistry was performed on 4 μm whole sections mounted on positively charged slides. Antibody against DLL3 (clone SP347, ready-to-use, Ventana, Roche) was incubated for 32 min on a Ventana Benchmark XT Immunostainer (Roche, Basel, Switzerland), after pretreatment with the Cell Conditioning 1 (CC1) solution for 80 min at 100 °C. Detection was conducted using the OptiView detection kit. A spot from an intensely and diffusely positive MTC was included as a positive control on each slide, normal thyroid parenchyma present in each tumor block was used as a negative control.
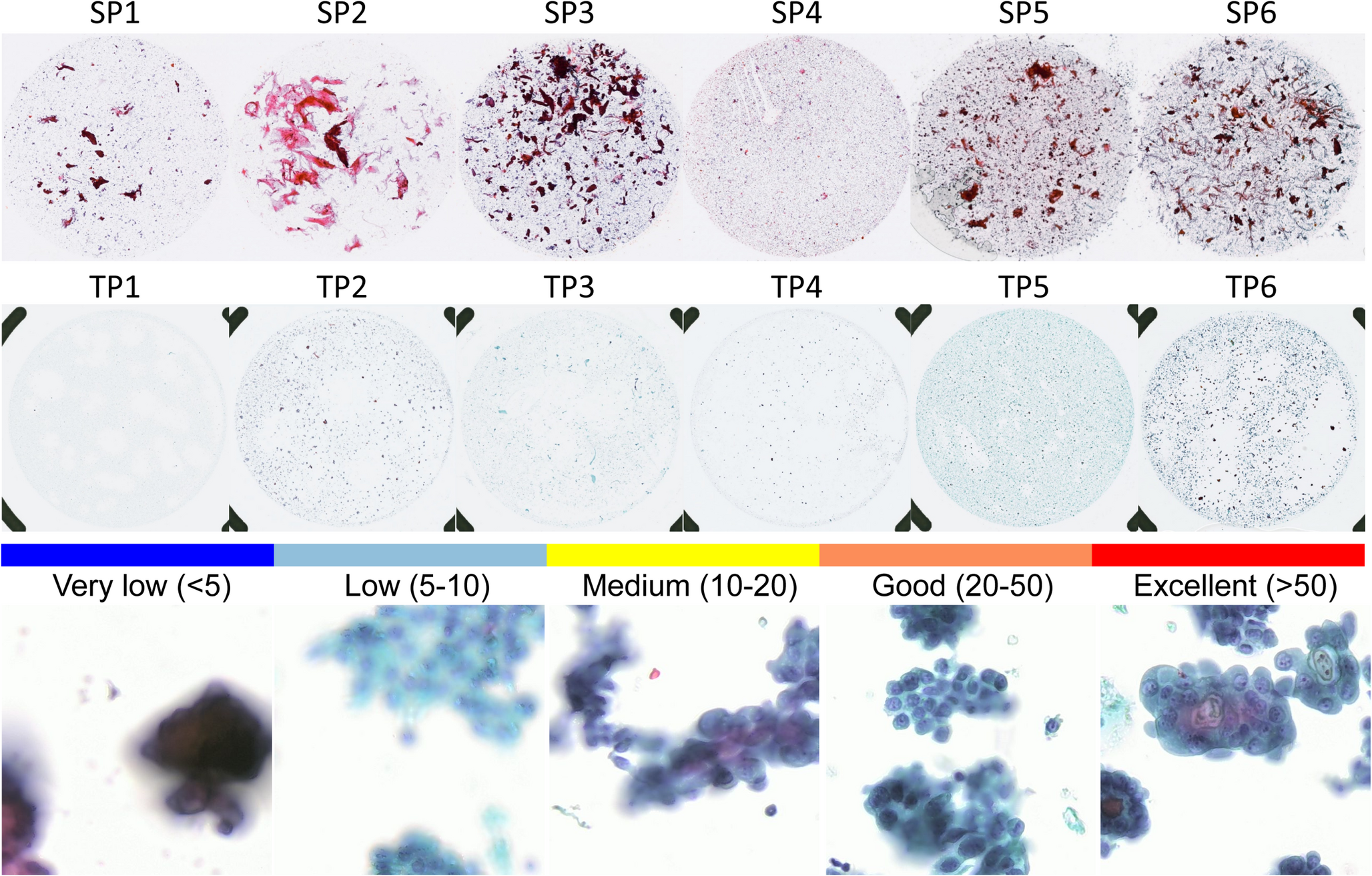
A hematoxylin-eosin-stained slide was evaluated together with DLL3 immunohistochemistry. Two endocrine pathologists (I.R.C. and A.R.) independently evaluated each slide. The percentage of tumor cells expressing DLL3 was evaluated following the previously published methodology [12]. Each pathologist quantified cytoplasmic and/or membranous expression as a percentage, using continuous values from 0 to 5, followed by increments of 10. The final DLL3 expression score was calculated as the means of the evaluations provided by both reviewers. Based on prior reports in MTC, three expression groups were defined: null (< 1%), low (1–49%), and high (≥ 50%) [13]. Additionally, staining intensity was classified as weak, moderate, or strong according to Ventana DLL3 (SP347) assay scoring criteria: Strong staining was defined as dark brown to nearly black cytoplasm and/or thickened, darkened membranes of similar intensity. Moderate staining corresponded to brown cytoplasm and/or membranes with less darkness than strong staining and thinner membranes, often less conspicuous at low magnification. Weak staining was characterized by light brown cytoplasmic and/or membranous signal lacking the richer brown tone seen in moderate intensity. Negative/equivocal included complete absence of detectable signal or pale grey/tan staining without true brown chromogenic deposition or membrane enhancement. Intensity scores were recorded independently of the percentage of positive tumor cells.
Statistical Analysis
Statistical analyses and associated figures were conducted using R software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria) and the following packages: psych, survival, coxphf, ggplot2, ggalluvial, and survminer. Agreement between DLL3 categorical assessments performed by both pathologists was evaluated using weighted kappa coefficient, calculated from the corresponding contingency table. The strength of agreement was interpreted according to Landis and Koch’s benchmarks.
For descriptive analyses, continuous variables were summarized as mean ± standard deviation (SD), and categorical variables as counts and percentages. Comparisons of continuous variables across the three DLL3 expression categories were performed using one-way analysis of variance (ANOVA). Comparisons of continuous variables between the heterogenous vs. homogeneous DLL3 tumors were performed using the Mann–Whitney U test. For categorical variables, comparisons across groups were performed using the Chi-squared test; when the expected frequency in any cell was < 5, Fisher’s exact test was applied instead.
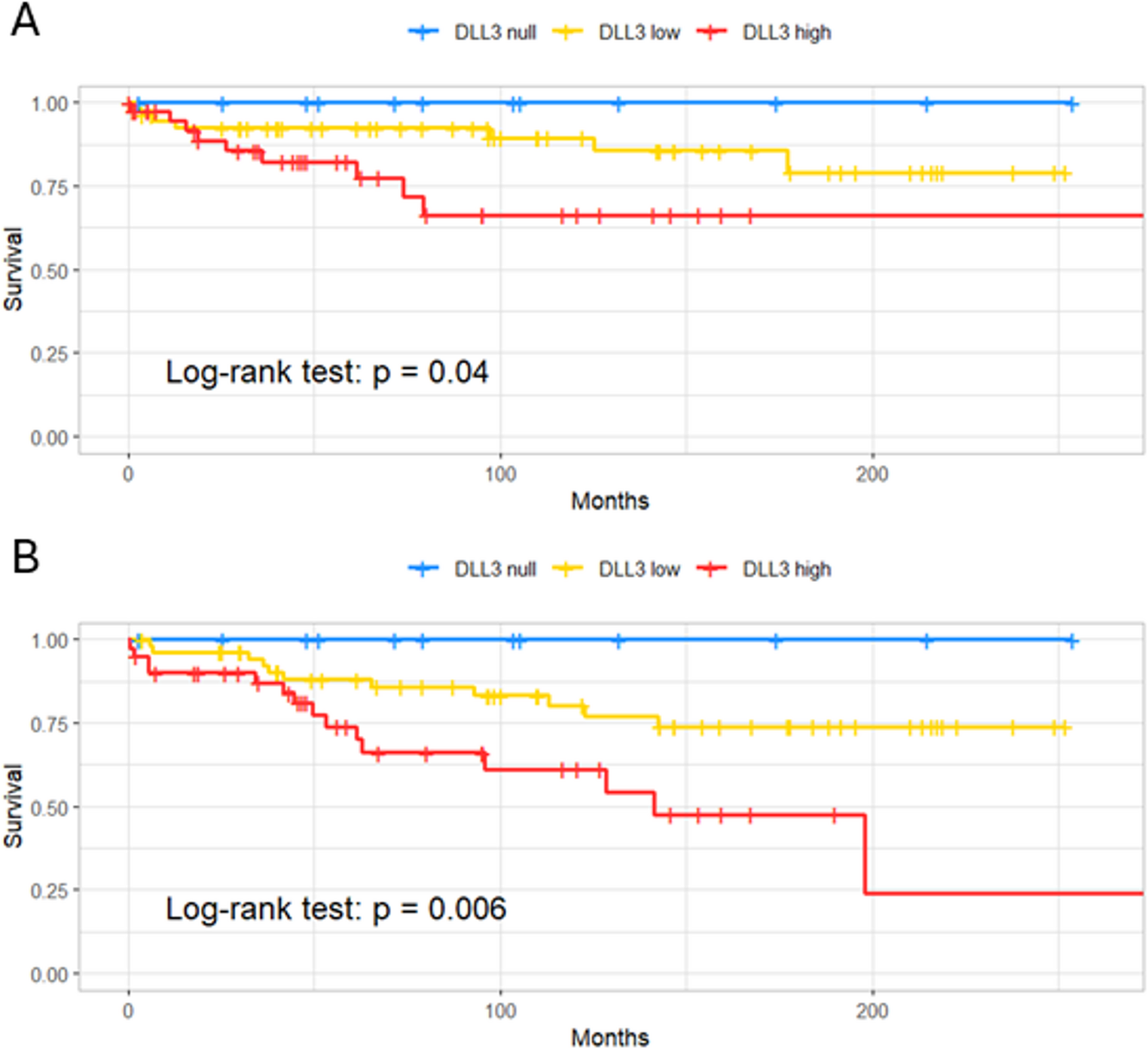
Disease-free survival (DFS) and overall survival (OS) were estimated using the Kaplan–Meier method and compared among DLL3 expression categories (null, low, high) with the log-rank test. Cox proportional hazards regression models were applied to evaluate the association between DLL3 expression and outcomes. Due to the small number of events and quasi-separation issues, hazard ratios (HR) and confidence intervals were estimated using Firth’s penalized maximum likelihood approach. Global model significance was assessed with the likelihood ratio test. All p-values were two-sided, and values < 0.05 were considered statistically significant.



Comments (0)