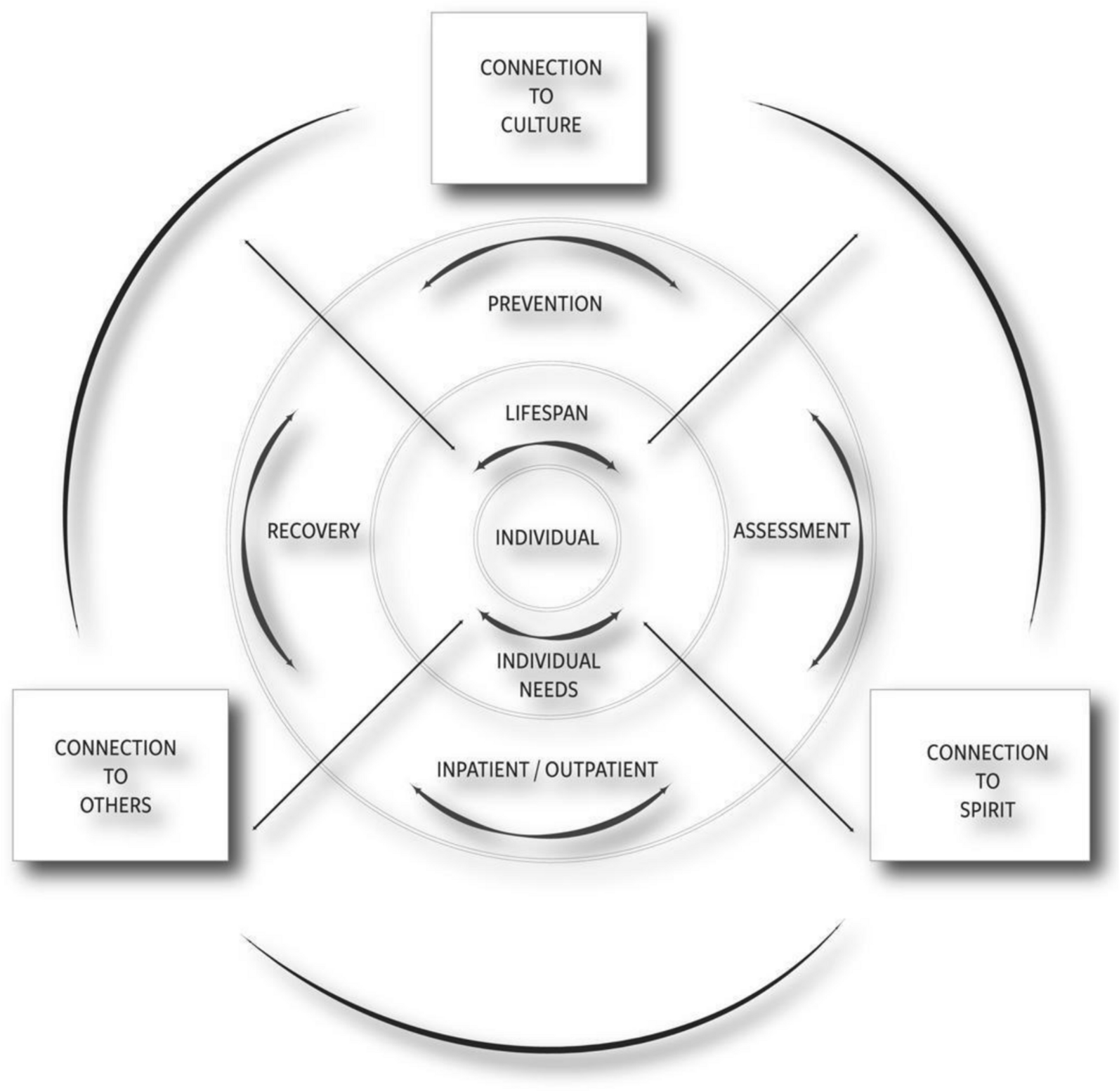
The 27 Indigenous research participants who were accessing a Syringe Services Program in a rural tribal Nation in Minnesota had clear ideas on what would impede or support seeking MOUD treatment. Participants described several themes that mapped onto various levels of the circular Aanji’bide Model of Opioid Recovery and Change. These themes focused on connection to others, flexibility of services, and needs that are grounded in social determinants and serve as barriers to seeking and receiving care. To our knowledge, this is the first study done with Indigenous participants who were accessing a Syringe Services Program to learn their perspectives on barriers and facilitators to opioid treatment.
Theme 1: connection to others
One of the central findings was that connection served as an important facilitator for seeking care. The topic of connection arose in several ways: connection to others (usually family), connection to providers, and connection to community. Consistent with what participants shared about connection to family as a motivator for seeking treatment, a systematic review of five randomized controlled trials on the relation between social support networks and improved MOUD treatment outcomes found that among partner, family, and peer networks, the family social support network had a particularly positive influence [15]. An analysis of responses among American Indian youth (n = 19,067) from the New Mexico 2000–2019 Youth Risk Resiliency Survey established that reporting more social support was associated with lower opioid use [1]. This study also showed that for youth who were using opioids, social support was associated with lower odds of having made a past suicide attempt.
Participants also indicated that connection to providers facilitated care [2]. They emphasized the benefits of communication that was nonjudgmental and accepting. The importance of exhibiting a nonjudgmental attitude when working with people living with stigmatized behaviors, such as opioid use, is well established in the literature as an important mechanism for delivering effective therapeutic care. Many of the findings in this study can resonate with people with OUD as a whole, not just for AI/AN individuals. Being accepting of where people are in terms of readiness to change is a core component of motivational interviewing, an evidence-based therapy for multiple forms of substance use and other behaviors, for example [20]. A study to reduce alcohol and drug use among AI/AN youth combined motivational interviewing with traditional practices [9] and asked about participants’ perceptions of this combined intervention model. Youth especially noted a high acceptability for the collaborative model that elicited their perspectives [9].
Another study used focus group discussions to gather feedback from AI/AN providers and community members about adapting motivational interviewing and communication for changing substance use behaviors [28]. Community members talked about several traditional ways of communicating for change—for example, focusing on strengths and using positive framing—that aligned well with motivational interviewing principles and techniques. AI/AN providers found the principles of motivational interviewing to be aligned with their cultural framework and experiences [28].
A study in Canada with Aboriginal and non-Aboriginal youth in residential treatment programs for substance use measured initial therapeutic alliance and treatment engagement [7]. They found that reporting a stronger alliance was associated with better engagement with treatment. However, a discrepancy between predominantly white practitioners’ assessments of having a strong positive alliance with all clients and Aboriginal youth’s less favorable assessment of alliance was present. While these studies align with this study’s findings, more research on therapeutic alliance and communication among practitioners and AI/AN clients in opioid use harm reduction and treatment settings is needed. Utilizing peer support specialists with lived experience can address concerns about counselors not having relatable drug use experience.
Theme 2: flexibility of services
An important identified facilitator centered around flexibility of services. Specifically, participants suggested that increasing availability of immediate medication initiation and flexibility of intake assessment times can reduce barriers to MOUD. These suggestions, among others, were also delineated in the scoping review by Bozinoff et al. [5] who found that longer prescriptions, streamlined referral processes, bridging inpatient and outpatient treatment programs, waiving prescriber and recipient requirements for prescribing and receiving MOUD, among others factors that increased flexibility, increased retention and engagement in MOUD. Implementing flexible service delivery models for MOUD care has been identified as a facilitator to care by others who work in low-resource settings in the US [6]. A systematic review of 38 studies that examined barriers from clients’ perspectives found lack of flexibility to be a major theme across studies [10].
Among AI/AN populations, implementing service delivery models that can flexibly address the needs of a population facing inequities in access to substance use care can provide a community-based approach that more accurately reflects the needs of AI/AN clients. One possibility to enhance flexibility further might be to make intake or follow-up assessments available via telehealth. A study done with Alaska Native clients compared 103 people receiving telepsychiatry with 103 others who were receiving usual care. They found that while those receiving telepsychiatry had higher rates of legal challenges, post-traumatic stress disorder, having children in outside custody, and a history of violence, they were more likely to complete treatment and less likely to discharge from services against provider advice [16]. Future research should explore other creative solutions that will enhance service delivery flexibility and reduce barriers to care.
Theme 3: social determinants needs as barriers to care
Another core finding was that individual needs rooted in social determinants of health played a significant role in participants’ ability and willingness to seek care. For instance, in this rural area, participants overwhelmingly cited unmet transportation needs. Similar social determinants of health concerns were also highlighted by Bozinoff and colleagues [5] who found that facilitating transportation, verifying that treatment programs and MOUD options were covered by insurance companies, and ensuring basic needs (food, water, housing) were met were associated with higher engagement in MOUD. Having health insurance reimburse clients for transportation costs could mitigate some of the burden related to transportation, especially in rural areas.
Examples of programs developed by tribal communities to address these barriers/facilitators
Tribal Nations have implemented innovative treatment approaches to increase access to MOUD services [19, 30, 35,36,37]. Elements of these programs often align with each of the three themes identified in this research to help mitigate barriers to MOUD.
For example, programs developed by Tribal Nations have emphasized connection to others (Theme 1) by offering clinical services with multiple sources of clinical support (e.g., traditional healers, psychiatrists, therapists/counselors, social workers), training tribal members to act as post-overdose peer support specialists, incorporating tribal elders and other community members in the treatment setting (e.g., as greeters), and sharing meals and other culturally meaningful moments of connection. They have focused on addressing individual needs (Theme 2) by coordinating and providing transportation to treatment facilities, providing childcare while patients are in treatment facilities, finding ways to reduce financial burdens associated with getting treatment, offering telephone assistance to support patients remotely when needed, and operating transitional housing and shelters. They have aimed to increase the flexibility of services (Theme 3) by removing punitive sanctions for people who use drugs while in treatment, implementing harm reduction approaches to “meet individuals where they are at,” educating patients, substance use disorder treatment clinicians, and other healthcare workers (e.g., emergency medical services workers) to maximize harm reduction practices and accept harm reduction goals, and fostering relationships with other community groups to reduce stigma associated with OUD and MOUD and to increase acceptance of treatment approaches (MOUD, harm reduction, etc.).
How Tribal Nation Behavioral Healthcare has changed as a result of the research
This research was conducted in March of 2022, just after the height of the COVID-19 pandemic. The Tribal Nation behavioral health system is characterized by its willingness to try new things to better serve Anishinaabe clients/relatives, and its commitment to creating sustainable models of healthcare. In addition, because of the close CBPR working relationship between the University and Tribal Nation members, in which the Community Action Board and other members of the Tribal Nation weigh in on the research and help steer its direction, the initial research findings were iteratively shared with the CAB, as they unfolded. The CAB Board met with the research team between the first and second week of data collection to hear about the first week of research and inform the next week of questions and data collection. Additional meetings have followed. Thus, some of the barriers described in this paper have been addressed by the Tribal Nation’s Behavioral Healthcare system since the time of the interviews, and some facilitators have been noted and enhanced. This was facilitated by having individuals on the CAB who are in leadership roles in the Tribal Nation (e.g., tribal government, director of services department, clinical leadership roles), and had the ability to influence these changes. This is one method to translate research findings into action.
Since the research study, the Tribal Nation has prioritized hiring more drivers to make transportation easier for MOUD program clients. The number of transportation staff has increased two-to-three times, though there are still some unfilled positions for drivers. Additionally, it is now easier to access and start treatment. Previously, clients had to complete a state-mandated Rule 25 assessment before starting Suboxone. Same day appointments were not always available. Now, clients do not have to wait for a state-mandated intake assessment to begin buprenorphine. This reflects a combination of tribal-level and state-level changes to make treatment access easier. On June 30, 2022, a few months after the research interviews were completed, the state moved from the Rule 25 assessment to a comprehensive assessment. In conjunction with these changes, the Tribal Nation Behavioral Health Division has built programming that prioritizes ease of access. Individuals have the option to complete a same-day medical intake assessment with an intake provider. The consent is all on one page. A more formal comprehensive assessment is still completed but not required immediately. Additionally, peer support staff are able to administer the comprehensive assessment.
Building on the flexibility aspect, clients can also be granted a special request to take home doses of buprenorphine, so they may not need to dose at the clinic every day. Cultural activities are now available almost daily. The clinic also made the reception area more welcoming, including having smudge and other traditional medicines available. Clinic staff have made efforts to destigmatize buprenorphine across the health system (e.g., addressing beliefs that one cannot be “sober” or achieve “recovery” while receiving MOUD). Clinical leaders within the health system continue to explore several other ways to reduce barriers to MOUD for people in the community (e.g., exploring ways to reduce barriers related to mandated assessment requirements, the lack of methadone treatment options within the area).
Strengths and limitations
This was one of the first studies to ask clients at a Syringe Service Programs about barriers and facilitators to opioid care in a rural, Indigenous setting. There exists ongoing partnerships between tribal members and the university team. This has allowed the involvement of those with lived experience. These individuals led the development of questions and assisted with formulating other protocols for this study. Interviews were facilitated by a non-Native research partner from outside of the community and data analysis was conducted by a diverse team (individuals identifying as AI/AN, white, different age groups and backgrounds, etc.). While it was attempted to avoid bias by gathering multiple perspectives, these factors could have influenced the way clients responded and analyses were carried out. Additionally, the brief length of the interviews and subsequent excerpts included above could be a limiting factor. The average length was eight minutes.
Conclusion
Participants in this study identified several barriers and facilitators related with three main themes that mapped onto domains of the Aanji’bide Model of Opioid Recovery and Change: connection to others, flexibility of services, and social determinants needs that are barriers to seeking and receiving care. Connection to others focused on connections with family, which most discussed as a facilitator, connection with providers as imperative for wellness, and connection with community. Flexibility of services emerged as an important facilitator, especially as it related to the ability to start MOUD when interested. Several barriers associated with individual needs, particularly transportation, also were important to MOUD treatment-seeking and care. Tailoring services to address identified barriers and leverage facilitators of connection and flexibility will enhance care.








Comments (0)