This investigation of UDS results among first-time arrestees in county jails across the United States analyzed a unique sample of arrestees who were screened and tested for drug use in a healthcare context based on the determination of withdrawal risk and voluntariness. Despite certain limitations in this selection process and reliance on routinely collected healthcare data, discussed in detail below, the reported findings are useful reflections of the prevalence rates and patterns of drug use as they are known to correctional healthcare providers (i.e., as they are documented in EHRs). This research also offers a unique opportunity to consider the current findings in the context of prior research on drug use in the general population and epidemiological jail studies.
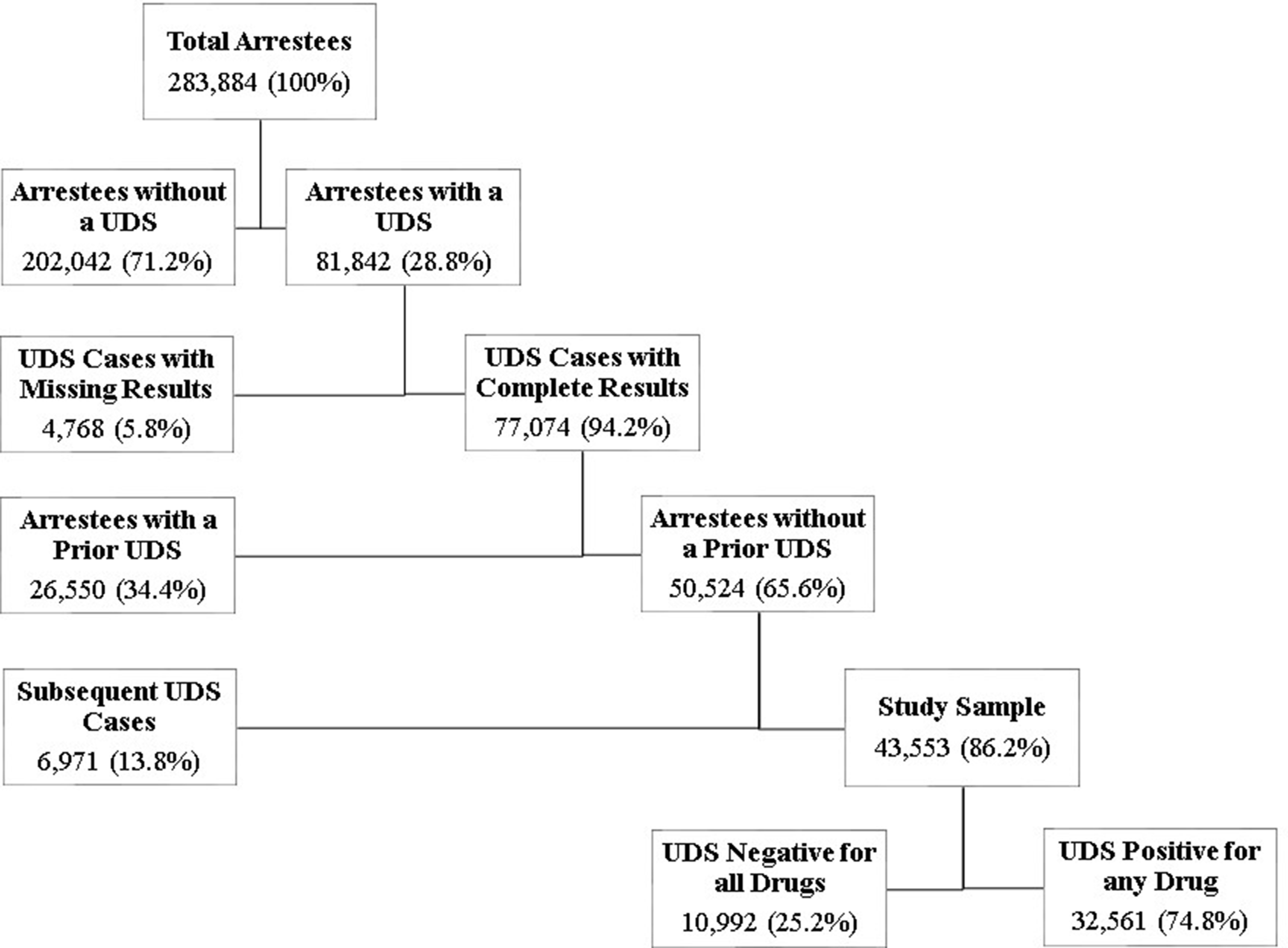
While 21.9% of the general population were estimated to have used drugs in the past year [19] and a range of 63–83% in jail settings were positive for drugs [22], almost one-third (28.8%) of arrestees in this study were deemed at risk for drug withdrawal and 74.8% of those tested positive for any drug. One can see that, although not operationally identical, the current results roughly correspond with these prior studies. Cannabis (marijuana) and stimulants were the most common drug types detected in the sample, which is consistent with the literature [24], and almost half of those testing positive for any drug tested positive for multiple drugs [23].
Geographic patterns of positive UDS results among arrestees in this study were inversely related between jail locations in the West and South, with a greater likelihood of cannabis and stimulants in the West; a greater likelihood of cannabis and sedatives in the South; and with predominate use of cannabis in the Midwest. The higher rate of positive UDS results in the West, mostly cannabis and stimulants, was consistent with the findings of the ADAM II project in Sacramento and San Diego [24]. The greater likelihood of testing positive for opioids and stimulants in medium-sized jails and more cannabis and sedatives in mega jails is new to the literature and may reflect emerging trends in rural (medium) versus urban (mega) jurisdictions not previously captured by large-scale research projects. Future research can explore this more directly.
Among the arrestee demographic findings, males and females did not differ in overall drug positivity, consistent with ADAM II in San Diego [24]; however, findings from this study revealed sex differences when analyzed at the drug type level. Female arrestees were less likely to test positive for cannabis, opioids, and stimulants than males and more likely to use sedatives. This finding is possibly linked to greater use of medications [44, 45] for psychiatric conditions [46, 47] among females, a hypothesis to be tested in future studies. White arrestees were more likely to test positive overall and for sedatives, opioids, and stimulants than other races while Black arrestees consenting to UDS were more likely to test positive for cannabis. Regarding age, younger arrestees (i.e., adolescents and young adults) were more likely to test positive for cannabis but less likely to test positive for other drug types. Adults were at the greatest risk for UDS results indicating the use of sedatives and stimulants, while seniors were at a greater risk of results positive for sedatives. Adolescents were less likely than expected to test positive for opioids, sedatives, or stimulants. Combined, and in the context of voluntary UDS, findings suggest ethnicity, race, and age may be important cultural and demographic factors to incorporate into a model of drug use assessment and treatment [48, 49] in this population.
Finally, this study found half of the arrestees undergoing UDS were positive for more than one drug. Combinations of cannabis and stimulants, opioids and stimulants, and cannabis, opioids, and stimulants were the most common, with stimulants intriguingly present in each combination. Additionally, stimulants and opioids were rarely positive alone and, rather, were more commonly detected in various combinations with other drug types. This could be explained by the practice of “speedballing,” or combining stimulants and opioids to experience the intense high of the stimulant while offsetting the negative effects with an opioid (or cannabis), or the unintentional use of an opioid, such as fentanyl while using stimulants, which could result in dangerous consequences such as heart failure, overdose, or death.
Limitations and future directions
This study addresses certain concerns with existing research of drug use among arrestees by analyzing a sample of arrestees in 2023, including both males and females, utilizing objective immunoassay point-of-care measures of drug use, relying on a larger and more representative sample of disparate jail locations and jail sizes across the United States, examining drug use at the level of individual drugs and an exploration of multiple drug use patterns, and characterizing drug use within a naturalistic healthcare context to inform screening, treatment, and prevention of negative drug-related outcomes including overdose and death in jails. Despite these myriad strengths, the limitations of the present study should be considered.
First, results cannot be interpreted as reflecting accurate population rates of types of drug use as might be found in an epidemiological or prevalence estimate study. Arrestees’ data used for this study were obtained within a healthcare delivery context in jails and not from a random or proportion/stratified sampling procedure. As such, the findings are limited to a subsample of arrestees who were identified to be at risk for negative drug use consequences determined by self-report and/or observation and who voluntarily submitted to a UDS, thereby excluding arrestees reluctant to disclose or endorse drug use risk criteria due to concerns about stigma, confidentiality, retribution, or other reasons. Despite this, the findings from this study characterize a real-life clinical context in jails and likely underestimate the actual extent of the problem. Strategies and policies designed to more accurately, economically, and confidentially detect drug use among all arrestees should be investigated. Additionally, individuals with prior arrests were excluded to focus on first-time arrestees, which prevented analysis of the impact of repeat arrests or changes in UDS results over time.
Second, drugs of abuse only, not alcohol, were analyzed for this study. Alcohol is likely the most prominent intoxicant among arrestees [50] and is associated with serious - even fatal - withdrawal symptoms [51]. Although there is value in understanding trends in alcohol intoxication among arrestees, we omitted this research question because observed or self-reported use of alcohol in this database was not consistent or reliable enough to confidently analyze, and archived immunoassay test results did not include alcohol. Given the prevalence of alcohol use and the importance of identifying arrestees at risk for alcohol withdrawal symptoms and the relative ease of alcohol testing, future research should focus on reliable alcohol use assessment, including saliva or breathalyzer tests to ascertain blood alcohol content and alcohol withdrawal risk measures to prevent negative alcohol-withdrawal related outcomes in jail.
Third, the assessment of drug types used was determined by point-of-care immunoassay tests only. Point of care or screening tests are designed to test for the absence of a drug or a presumptive presence or positivity of a drug and fail to provide additional discriminatory information. For example, UDS testing does not discriminate between illicit or legitimately prescribed drugs, discern inadvertent use of a drug (e.g., adulterated substances), provide a quantitative measure, measure prolonged use or tolerance, detect brief drug use or metabolized drugs, or meet SUD criteria for diagnosis. Furthermore, UDS cannot determine whether drugs were taken simultaneously or within the same use session, as some substances remain detectable in urine for days after use. However, research on people who use drugs and drug surveillance data indicate that drug combinations are common. Despite this, it is important to acknowledge this limitation when interpreting the findings. Moreover, while UDS is effective at detecting common drugs of abuse, it may not identify novel psychoactive substances emerging in the unregulated drug market, including certain fentanyl analogs [52]. Policies and investigation of the practical implementation of both quantitative and qualitative assessment strategies to provide sufficient information for an informed treatment response are needed.
Fourth, while UDS tests used for this study were designed to detect unique metabolites of specific drugs with unique reagents, a presumptive positive outcome is likely to lack specificity and risk cross-reactivity between drugs tested than a negative result. We found significant cross-reactivity between amphetamine and methamphetamine, necessitating combining the two drugs. Point-of-care immunoassay testing is still an economic and practical detection strategy that would likely be enhanced by the addition of confidential structured self-report techniques, questions of incremental validity and utility for future studies to examine.
Fifth, for the first look at these data, drugs were grouped into four types (cannabis, opiates, sedatives, and stimulants) instead of looking at each drug separately for ease of descriptive and statistical comparisons by jail characteristics and arrestee demographics. While the message is still clear and the findings useful, future investigations of specific drugs and drug combinations, like fentanyl and methamphetamine, may provide more sensitive and specific information about their unique contribution and impact on withdrawal management, maintenance treatment, and overdose risk.
Finally, while the exclusion of individuals with arrests from 2020 to 2022 was intended to control for multiple arrests, this period coincided with significant shifts in law enforcement practices, court operations, and crime trends [53]. The pandemic led to changes in arrest patterns, including decreases in drug-related offenses and property crimes due to altered policing strategies, as well as increases in substance use and domestic violence. Given these factors, it is possible that the 2023 first-time arrestee population differs from pre-pandemic cohorts in ways that were not explicitly considered.








Comments (0)