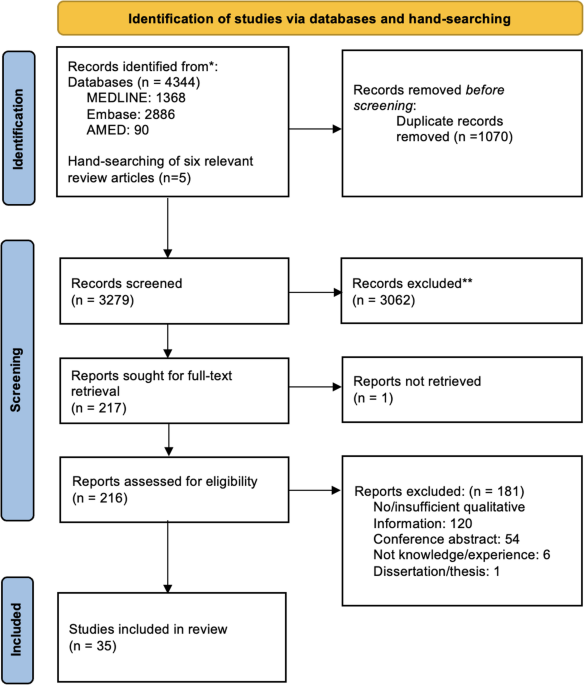
This narrative review primarily utilized scientific literature from databases such as PubMed, Medline Complete, and Cochrane. The search incorporated keywords including ‘colorectal cancer,’ ‘epidemiology,’ ‘diagnosis,’ ‘management,’ ‘adjuvant therapies,’ ‘neo-adjuvant therapies,’ ‘tumorigenesis,’ and ‘prevention strategies,’ using Boolean operators (e.g., “Colorectal cancer” AND “Diagnosis”). Most selected studies were published between 2014 and 2024, with some exceptions. Only English-language publications were included. Additional data were sourced from reputable organizations, including the WHO, GLOBOCAN, the National Cancer Centre, and Bowel Cancer UK. Guidelines from the National Institutes for Health and Care Excellence (NICE, UK) were also reviewed, and clinical trial data were retrieved from ClinicalTrials.gov.
Disease Presentation
In early-stage CRC, the disease is usually asymptomatic, but as it progresses, faecal blood may be visible, varying in color based on the bleeding site. This can lead to iron deficiency anemia, with symptoms such as weakness, fatigue, and paleness [9]. Advanced-stage symptoms include intestinal obstruction, causing abdominal cramps, distension, and vomiting, with large masses sometimes being palpable [9]. Bowel movement changes, such as constipation, diarrhea, and stool narrowing, may also occur. In late stages, systemic symptoms including weight loss and fatigue are common [2]. While these symptoms suggest CRC, their specificity varies. Rectal bleeding has a positive predictive value (PPV) of 4.0% and a specificity of 99.4%, yet lower abdominal pain and bloating are less specific and have a lower PPV [10].
DiagnosisHistory
Gathering a complete patient history is critical for identifying predisposing factors and symptoms that may indicate a high probability of CRC and require further investigations to confirm the diagnosis [11].
Abdominal Physical Examination
The next step in diagnosing CRC involves an abdominal physical examination, which can indicate the presence of a mass or obstruction in the gastrointestinal (GI) tract. In females, the vagino-recto-abdominal examination is additionally used to investigate for any vaginal metastasis. Additionally, a rectal examination is also considered to assess any masses in the rectum [12].
Laboratory Tests
Laboratory tests play a pivotal role in the diagnosis of CRC. A complete blood count is performed to detect anaemia, which can be indicative of chronic GI bleeding, and stool testing for occult blood is undertaken as it may indicate lesions in the GI tract. Additionally, liver and renal function tests are assessed to evaluate organ functionality [13].
In cases where CRC is suspected, tumour biomarkers are measured to aid in diagnosis and disease monitoring. Carcinoembryonic antigen (CEA) is the most widely utilized biomarker for CRC, particularly for monitoring disease progression and response to treatment. Alpha-fetoprotein (AFP), while primarily associated with liver cancers, may occasionally be measured to evaluate for potential liver metastases. Additionally, CA125 is used in cases where ovarian or peritoneal metastases are suspected [13].
Imaging
Initial imaging techniques are crucial for the detection and evaluation of CRC. CT imaging is the preferred modality for assessing intra-abdominal metastases due to its superior sensitivity and detailed visualization of abdominal organs and lymph nodes. For rectal cancer, rectal MRI is the preferred imaging technique where available, as it provides superior anatomical detail and accurately assesses tumour depth and potential involvement of surrounding structures. Furthermore, barium gas double X-ray is employed to identify filling defects and mucosal degradation in the intestine [12].
Endoscopy, Biopsy and Histopathology
Following laboratory tests and initial imaging, endoscopic procedures are conducted to evaluate CRC in detail. These procedures included sigmoidoscopy, rectoscopy, and colonoscopy, which help assess tumor size, depth, location, infiltration, and morphology. During endoscopy, biopsies of any suspicious lesions are taken for histopathological examination, which is essential for confirming the diagnosis and guiding treatment plans [12, 14].
Although colonoscopy is an invasive procedure, less invasive alternatives, such as capsule endoscopy, have been developed to examine nearly the entire GI tract. This technique offers a more patient friendly option while still providing valuable diagnostic information [8, 15].
Genetic Testing
Several mutations in genes including APC, NRAS, KRAS, TP53 and BRAF contribute to CRC pathogenesis. While testing for these genetic mutations provides valuable information for guiding treatment strategies and assessing prognosis, it is not diagnostic of CRC. Testing for mismatch repair (MMR) protein expression or microsatellite instability (MSI) is often conducted to identify specific tumour characteristics and guide therapeutic decisions, such as the use of immunotherapy. Although research into chromosomal instability (CIN) and the use of microRNAs as prognostic or predictive markers is ongoing, these tools are not yet widely used in clinical practice [16].
Staging
The staging of CRC occurs in two phases. and follows the TNM classification system, which assesses tumour depth (T), lymph node involvement (N), and distant metastases (M). Patients are grouped into four stages (I-IV), each corresponding to a specific prognosis. Clinical staging is conducted after diagnosis and prior to initiating treatment. It uses imaging studies (e.g., CT, MRI, PET-CT) and, where needed, endoscopy to estimate the extent of the disease. This phase is critical for guiding pre-treatment decisions, such as the use of neoadjuvant therapy. Pathological staging is performed after surgical resection to provide a definitive assessment of the primary tumour, lymph nodes, and metastatic involvement through histopathological evaluation [7].
For patients undergoing neoadjuvant therapy, post-treatment staging assesses tumour response and refines subsequent treatment decisions. While less frequently used, the Modified Astler-Coller and Dukes systems may also be referenced. Ultimately, treatment decisions consider not only the cancer stage but also patient comorbidities and preferences [7].
Diagnosis of Complex Gastrointestinal Cases
In complex GI cases where diagnosis is challenging, investigative approaches may include the use of open surgery and laparoscopic exploration. Additionally, surgical intervention may be necessary in instances of suspected bowel perforation, intestinal obstruction or significant GI hemorrhage [6, 17].
Emerging Technologies
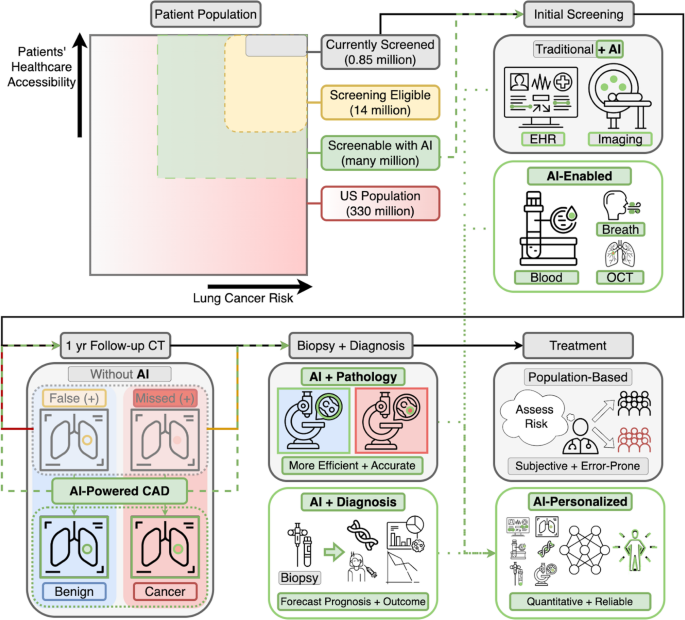
Emerging technologies are increasingly incorporating artificial intelligence (AI) into different areas of healthcare. AI can gather and analyze public data for digital epidemiology, assisting clinicians in early disease detection and health surveillance. Furthermore, AI can enhance the diagnostic process of CRC by improving imaging techniques, allowing faster image interpretation, and minimizing artefacts. Moreover, AI can play a crucial role in the detection and classification of CRC based on histopathology [18].
Epidemiology
CRC was the third most common cancer globally in 2020, impacting individuals of all genders and ages [19].
Incidence
In 2022, the global age-standardized incidence rate (ASIR) for CRC was 19.7 per 100,000 individuals. Marked regional differences were observed, with Europe and Oceania reporting the highest ASIRs, ranging between 30 and 36 per 100,000, followed by North America, where the rate was approximately 26–30 per 100,000. Latin America, the Caribbean and Asia had intermediate rates, estimated between 12 and 20 per 100,000. The lowest incidence was recorded in Africa, with an ASIR of approximately 5 to 9 per 100,000. Notably, the ASIR was higher in males (22.0 per 100,000) compared to females (15.2 per 100,000) [19].
Prevalence
In 2022, the global 5-year prevalence of CRC was approximately 73.2 per 100,000 individuals. Regional disparities were evident, with Central Europe exhibiting prevalence of 90–100 per 100,000 and North America 80–95 per 100,000 individuals [19].
Survival
According to global cancer survival estimates reported by the CONCORD-3 study and other international sources, the overall global 5-year survival rate for CRC varies widely by region but is estimated to be 60% for all stages. Survival rates differ significantly depending on the stage at diagnosis, emphasizing the crucial role of early detection. The global 5-year relative survival rate for localized (stage I) CRC is approximately 90%, while for regional (stage II and III) CRC, it drops to about 70–75%. For distant (stage IV) CRC, the 5-year relative survival rate decreases dramatically to around 15% [20].
Mortality
CRC ranked the third leading cause of cancer-related deaths worldwide in 2022, accounting for approximately 1,050,000 deaths globally [19]. The global age-standardized mortality rate (ASMR) for CRC was around 10.0 deaths per 100,000 population. Colon and rectal cancers contributed approximately 6.0 and 4.0 deaths per 100,000, respectively. Regionally, the highest mortality rates were observed in Asia, with an ASMR of about 11.5 deaths per 100,000, representing roughly 55% of global CRC deaths. Europe followed with an ASMR near 14.0 deaths per 100,000, while Latin America and the Caribbean reported rates around 7.0 deaths per 100,000 [19].
CRC is expected to escalate, with an estimated 3.2 million new cases and 1.6 million deaths by 2040. This projection indicates that the global impact of CRC will significantly increase. Notably, highly developed countries are anticipated to have most of these cases [21].
PathophysiologyAnatomical Location of CRC
CRC can develop anywhere along the colon and rectum, from the cecum to the rectum. The distribution of CRC varies by anatomical site. A study involving 3,058 cases of CRC found the following distribution: sigmoid colon 24.5%, ascending colon 20.7%, rectum 17.3%, cecum 15.5%, transverse colon 8.2%, descending colon 7.2%, and rectosigmoid junction 6.6%. Additionally, 7.1% lacked anatomical location information and were censored at the time of diagnosis [22].
Histological Types of CRC
Pathological histological types of adenocarcinomas include papillary adenocarcinoma, mucinous adenocarcinoma, adenosquamous carcinoma, tubular adenocarcinoma, signet-ring cell carcinoma, undifferentiated carcinoma, carcinoid carcinoma, and squamous cell carcinoma [9, 23,24,25].
Development of CRC
The development of CRC typically begins with hyperplasia, characterized by an increased proliferation of normal cells. Over time, hyperplasia can progress to dysplasia, which involves abnormal cellular architecture and atypical growth, marking a precancerous stage. Dysplastic changes may further advance to the formation of adenomas, some of which can eventually transform into invasive cancer. Chromosomal instability, genetic mutations, and hypermethylation of CpG islands in gene promoter regions are three well-established molecular mechanisms associated with CRC pathogenesis [16].
Theories for the Development of CRC
Several theories have emerged to explain the development of CRC.
The Adenoma-Carcinoma Sequence
The adenoma-carcinoma sequence is a well-established theory, describing the progression of morphological changes from hyperplasia to dysplasia leading to the formation of malignant, invasive tumours. This process is primarily characterised by failure in the regulation of cell proliferation [16, 26, 27]. The conventional pathway begins with mutations in the adenomatous polyposis coli (APC) gene, which promotes increased cell proliferation and the development of a polyp. This is followed by sequential mutations in the genes KRAS and DCC, leading to further proliferation and increasing the size of the polyp. Furthermore, the mutation in the TP53 tumour suppressor gene contributes to carcinogenesis, and the malignant tumour formed spreads to the tissue surrounding it and to the distant organs [16, 28, 29].
The Mutator Pathway
The mutator pathway suggests that certain genetic syndromes which strongly elevate the risk from CRC, result from inherited genetic mutations [16, 30]. These syndromes include the Familial Adenomatous Polyposis (FAP) syndrome (which is associated with a mutation in the APC gene), the Lynch syndrome (LS), the Peutz-Jeghers syndrome, hereditary mixed polyposis, juvenile polyposis, and MUTYH-associated polyposis [16, 31, 32].
The Serrated Pathway
The serrated pathway involves hyperplastic polyps and a subgroup of serrated polyps as precursors to CRC [16, 30]. It is characterized by cytosine hypermethylation in CIMP lesions, BRAF mutations, promoter methylation, and microsatellite instability (MSI) [16, 35]. Sessile serrated adenomas/polyps linked to this pathway are significant CRC precursors. Serrated polyposis syndrome, characterized by numerous large, serrated polyps, is also a risk factor for CRC [16, 33, 34].
Genetic and Epigenetic Mutations Associated with CRC
CRC is a cancer characterized by genetic and epigenetic mutations. Mutations in the KRAS oncogene is among the most significant somatic mutations, found in approximately 50% of CRC cases [9, 35]. Allelic losses of tumor suppressor genes are common in CRC, including losses of chromosome 5q in 20%-50% of cases, chromosome 17p in over 75%, and chromosome 18q in more than 70% of CRCs [9, 35]. Mutations in the TP53 gene may provide a selective growth advantage, promoting tumor progression. Early in colorectal tumorigenesis, DNA methylation loss contributes to genomic instability. CRC is also associated with increased C-MYC expression, elevated tyrosine kinase activity, and altered glycoconjugate expression [9, 35].
Local Invasion and Metastasis
Four primary pathways facilitate the spread of CRC including local invasion, lymphatic metastasis, hematogenous metastasis, and implantation/metastasis. Local invasion entails tumour infiltration into surrounding tissues, while lymphatic metastasis involves the spread of cancer cells to regional lymph nodes via the lymphatic system. Hematogenous metastasis occurs when cancer cells travel through blood vessels, often targeting the liver and lungs. Implantation/metastasis involves detached cancer cells implanting in the abdomen and pelvic peritoneum, forming metastatic foci [9].
Management
A key determinant of management strategy is staging, which is used to apply the appropriate therapy protocol that significantly varies based on the stage of the disease at the time of diagnosis [7]. The evolving landscape of CRC treatment underscores the importance of tailoring interventions based on tumor biology, offering a promising avenue for improving outcomes in the complex journey of combating CRC [8].
Surgery
Surgery is fundamental in managing stage I-III colon and rectal cancer, requiring meticulous dissection to remove tumours and their primary lymphatic zones. Pre-operative considerations include patient age, tumour stage and tumour location [36].
Colon Cancer Surgery
In colon cancer management, laparoscopic surgery is a safe alternative to open surgery, with laparoscopic resection recommended when appropriate. The decision depends on tumour characteristics, surgical risks/benefits, and the surgeon’s experience [8, 36].
Ostomies—such as loop ileostomy, loop colostomy, or permanent colostomy—are created to manage bowel obstruction, protect healing tissues after surgery, or prevent complications such as anastomotic leakage, especially after preoperative radiation for rectal cancer. Temporary ostomies provide faecal diversion to support healing, while permanent colostomies are used when bowel restoration is not feasible. The choice of ostomy depends on the tumour location, disease extent, and patient needs [8, 36].
Rectal Cancer Surgery
For rectal cancer, treatment strategies vary by stage. Early-stage rectal cancer can utilize minimally invasive techniques, such as trans-anal endoscopic microsurgery, to avoid abdominal scars and stomas. Advanced tumours may require total mesorectal excision, especially after neoadjuvant therapy [8]. According to NICE guidelines, surgical treatment is tailored to the disease stage, with options including transanal excision and other minimally invasive techniques. While laparoscopic surgery is preferred, open surgery may be necessary for more complex cases. Robotic and transanal total mesorectal excision is advised within specialized settings, and extensive surgeries including multi-visceral resections may be required for advanced cases [36].
Adjuvant and neo-adjuvant TherapiesNeoadjuvant Chemotherapy (NACT)
NACT involves the administration of anti-cancer drugs before the primary treatment, usually surgery to shrink the tumour and facilitate its removal [37]. Common NACT regimens include FOLFOX (folinic acid, fluorouracil, oxaliplatin) and CAPOX (capecitabine, oxaliplatin), which are primarily used for tumours without high microsatellite instability (MSI-H) or mismatch repair deficiency (dMMR) [37].
For MSI-H/dMMR tumours, immune checkpoint inhibitors such as dostarlimab and pembrolizumab (both PD-1 inhibitors) are recommended based on their efficacy in these biomarker-defined subgroups. FOLFIRI (folinic acid, fluorouracil, irinotecan) and TAS-102 (trifluridine and tipiracil), while valuable in metastatic or refractory settings, are not standard NACT regimens in the non-metastatic context [37].
NACT offers the advantage of targeting occult micrometastatic disease early, improving surgical outcomes by reducing tumour size and enhancing resection success. Treatment regimens are tailored to individual patient and tumour characteristics, including biomarker status, tumour location, and disease stage [37].
Neoadjuvant Radiotherapy (NART)
NART is crucial in rectal cancer treatment, especially for stage II-III cases, by shrinking tumours and improving surgical outcomes with clearer margins and reduced recurrence risk. Its use in colon cancer is rare and typically considered only for large tumours or those involving adjacent organs. Recently, combining NART with NACT, termed total neoadjuvant therapy (TNT), has become standard for locally advanced rectal cancer [37, 38].
Adjuvant Chemotherapy
Adjuvant chemotherapy is administered post-surgery to eliminate remaining cancer cells and reduce recurrence risk [39]. For CRC, particularly in stage II-III, common regimens include CAPOX and FOLFOX, with the choice influenced by tumour histopathology, patient condition, and preferences (NICE, 2020). These regimens, focusing on microscopic disease, are critical for improving patient outcomes [7, 36, 40].
Adjuvant Radiotherapy
Adjuvant radiotherapy, used primarily in rectal cancer, targets residual cancer cells post-surgery to prevent recurrence [39]. In high-risk colon cancer, it may be considered if there is a significant local recurrence risk. It aims to target any remaining microscopic disease [8].
Immunotherapy
Immunotherapy focuses on using the immune system to fight cancer. Immune checkpoint inhibitors (ICIs), modulate interactions among T cells, antigen-presenting cells, and tumor cells. ICIs have shown significant efficacy in treating patients with metastatic CRC (mCRC) exhibiting deficient mismatch repair (dMMR) or high microsatellite instability (MSI). The FDA has approved nivolumab and pembrolizumab, alone or with ipilimumab, for such cases based on their demonstrated efficacy in clinical trials. These immune checkpoint inhibitors have shown significant and durable response rates in patients with advanced or metastatic CRC. For instance, pembrolizumab achieved an overall response rate (ORR) of 40%, with some patients experiencing sustained responses lasting over two years in clinical studies. Similarly, nivolumab, when used alone or with ipilimumab, has demonstrated durable disease control and progression-free survival benefits in this biomarker-defined subgroup [41]. The challenge remains to extend these benefits to the majority of mCRC patients with MMR-proficient and low MSI tumours, as these often lack sufficient mutated antigens for immunotherapy to target effectively [42].
Targeted Therapy
Targeted therapy for CRC employs drugs or substances that precisely attack cancer cells, usually by interfering with specific molecules involved in tumour growth and progression. Unlike traditional chemotherapy, which can affect both cancerous and healthy cells, targeted therapy aims to minimize damage to normal cells by focusing on specific cellular targets associated with cancer [39].
PARP Inhibitors
Poly ADP-ribose polymerase (PARP) is an enzyme essential for repairing single-strand breaks in DNA. PARP inhibitors (PARPi) have shown marked efficacy in cancers with BRCA1/2 mutations, such as ovarian and breast cancers, and are FDA-approved for these indications. However, their role in CRC is limited due to the low prevalence of BRCA1/2 mutations in these tumours. Current research is investigating their use in CRC with other DNA repair deficiencies, such as homologous recombination deficiency (HRD), and in combination with other therapies, though clinical evidence in this context remains nascent [43, 44].
Kinase Inhibitors
Kinases are enzymes essential for cell signalling, growth, and survival with abnormal activity leading to uncontrolled cell growth, cancer cell proliferation and survival. Kinase inhibitors target this dysfunction to disrupt cancer progression. In metastatic colorectal cancer (mCRC), regorafenib and fruquintinib are approved tyrosine kinase inhibitors used as third-line therapies when the disease has progressed. Regorafenib, an oral multi-kinase inhibitor, impedes angiogenesis, tumour growth, and the tumour microenvironment by inhibiting multiple signalling pathways, thus curtailing tumour advancement [45].
Management of Metastatic CRC
Metastatic CRC is managed through a combination of chemotherapy and targeted therapies. Monoclonal antibodies that inhibit the epidermal growth factor receptor (EGFR), such as cetuximab and panitumumab, are used in patients with KRAS wild-type tumours, particularly in left-sided CRC. Additionally, bevacizumab, which targets vascular endothelial growth factor (VEGF), is employed to suppress angiogenesis and limit tumour progression. For cases amenable to surgical resection, especially in the liver, removing isolated metastases significantly improves outcomes, with a notable 5-year overall survival rate of approximately 20%. Surgical intervention for liver metastases broadens the therapeutic options available [









Comments (0)