Molecular profiling has shown that BTCs are genetically heterogeneous tumors, with distinct mutation profiles depending on anatomical subtype and etiological background. Overall, approximately 40% of BTC patients harbor genetic alterations that are potentially actionable with targeted therapies [4]. This fraction is relatively high compared to other gastrointestinal malignancies and underscores the importance of routine genomic testing in BTC. However, the frequency of specific mutations varies markedly between iCCA, eCCA, and GBC:
Intrahepatic cholangiocarcinoma (iCCA): Among BTC subtypes, iCCA (arising in the liver) has the highest prevalence of targetable genetic alterations. Two of the most common are Isocitrate dehydrogenase 1 (IDH1) mutations and fibroblast growth factor receptor 2 (FGFR2) gene fusions or rearrangements, which are found in roughly 15–20% and 10–15% of iCCA cases, respectively. First, IDH1 mutations and FGFR2 fusions are largely confined to iCCA and are mutually exclusive—tumors almost never have both alterations. These mutations tend to occur in the small-duct subtype of iCCA and are virtually absent in the extrahepatic type. Other actionable alterations in iCCA include BRAF V600E mutations, although these are less frequent (BRAF V600E in ~3–6%); iCCA also commonly exhibits mutations in genes such as KRAS and TP53, but those are not currently targetable and are more associated with large-duct iCCA or fluke-related etiologies [5].
Extrahepatic cholangiocarcinoma (eCCA): Extrahepatic bile duct cancers frequently harbor mutations in KRAS (up to ~30%) and TP53 (~40%), as well as alterations in tumor suppressors, e.g., SMAD4 and CDKN2A/B. Targetable alterations are comparatively less common in eCCA. Notably, HER2 (ERBB2) amplification or overexpression is found in an important subset of eCCA (approximately 5–15% of cases). IDH1 mutations and FGFR2 fusions are rare or absent in eCC. Microsatellite instability-high (MSI-High) due to mismatch repair deficiency is rare in eCCA (on the order of a few percent or less), similar to iCCA [6].
Gallbladder cancer (GBC): Gallbladder carcinomas have the highest prevalence of HER2 amplification among BTCs—reported in approximately 10–20% of cases. Indeed, HER2 is often the only clear targetable driver identified in advanced GBC, as other actionable mutations are. GBC shares some molecular features with eCCA, including frequent TP53 mutations (> 50%) and KRAS mutations (~10%), while IDH1 mutations and FGFR fusions are extremely rare [7].
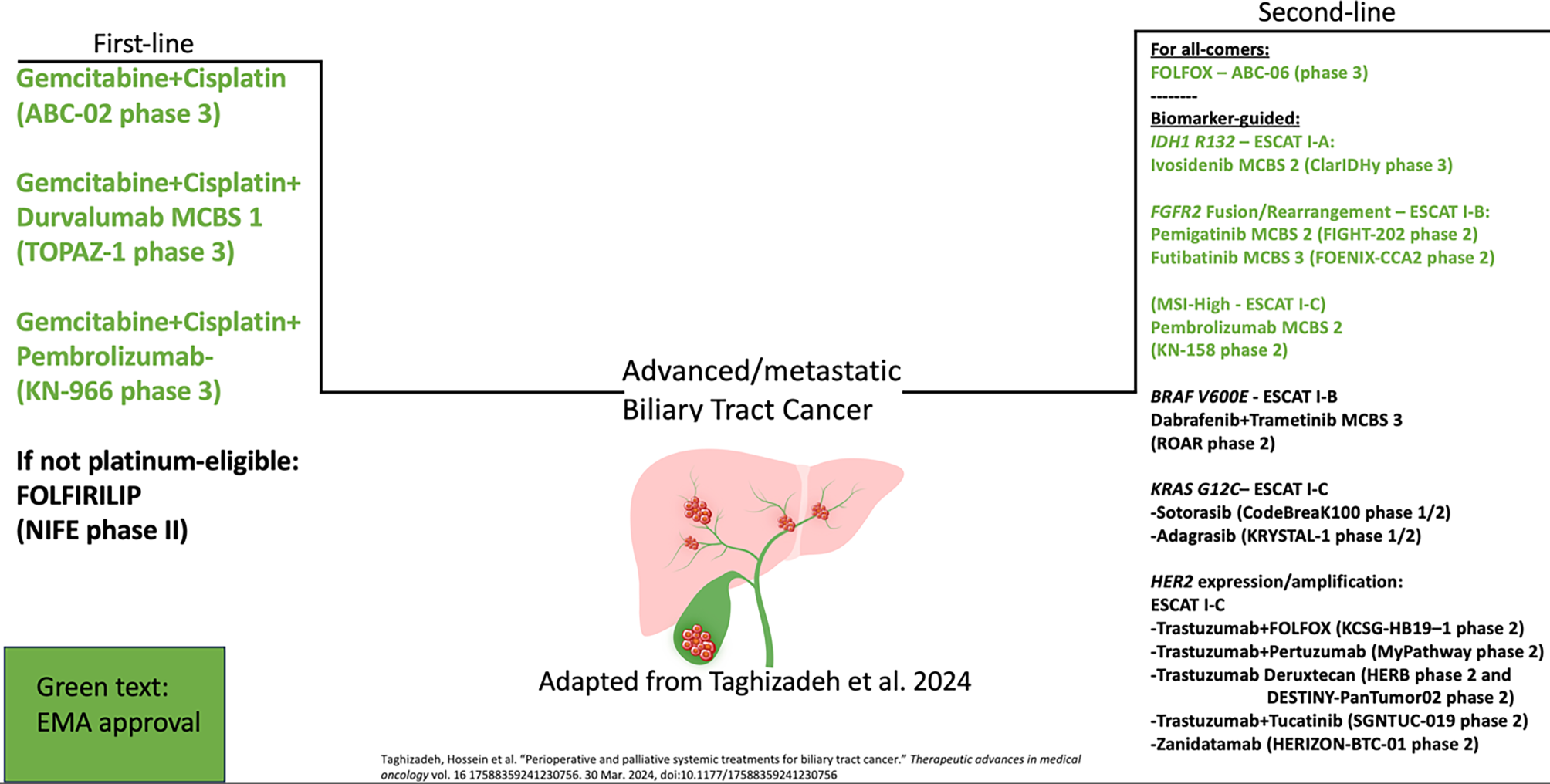
Many of the common mutations in BTC (such as KRAS, TP53, SMAD4) currently lack approved targeted treatments, highlighting the fact that only a subset of patients will have actionable findings. Nonetheless, the discovery of these targetable alterations and the development of matching therapies have already begun to improve outcomes. These therapies are generally indicated in the second-line or later setting (after progression on standard chemotherapy), and their use is predicated on the identification of the matching biomarker via molecular profiling.
FGFR2 fusions—FGFR inhibitors
Fusions or gene rearrangements of FGFR2 are oncogenic drivers that result in constitutive activation of FGFR2 signaling, promoting tumor cell proliferation [8].
Two FGFR kinase inhibitors have gained approval for previously treated FGFR2 fusion-positive cholangiocarcinoma: pemigatinib and futibatinib. Pemigatinib was the first to be approved (by the US Food and Drug Administration [FDA] in 2020 and the European Medicines Agency [EMA] in 2021) after demonstrating clinical benefit in the phase II FIGHT-202 trial. In FIGHT-202, pemigatinib achieved an objective response rate (ORR) of 35.5% (95% CI: 26.5–45.4%) in patients with FGFR2 fusion-positive CCA, whereas no responses were seen in patients without FGFR2 alterations. The median progression-free survival (PFS) was 6.9 months in the FGFR2 fusion cohort [8].
Subsequently, the irreversible covalent pan-FGFR inhibitor futibatinib (TAS-120) showed even higher efficacy in a similar population. In the FOENIX-CCA2 trial, futibatinib achieved an ORR of 42% in previously treated FGFR2-rearranged iCCA, with a median PFS of 8.9 months [9].
IDH1 mutations—IDH inhibitor
Mutations in IDH1, typically the R132C or R132L substitutions, occur in about 15% of intrahepatic cholangiocarcinoma cases. These IDH1 mutations result in the production of an oncometabolite (2-hydroxyglutarate) that drives epigenetic dysregulation and cholangiocarcinoma development. Ivosidenib is an oral IDH1 inhibitor that became the first molecularly targeted drug approved for cholangiocarcinoma (FDA 2021, EMA 2023). Approval of ivosidenib was based on the phase III ClarIDHy trial, which enrolled patients with advanced IDH1-mutated cholangiocarcinoma who had progressed on prior therapy. Ivosidenib significantly prolonged PFS compared to placebo: median PFS 2.7 months vs. 1.4 months, respectively (hazard ratio [HR]: 0.37, P < 0.0001). Although the objective response rate was low (approximately 2% with ivosidenib vs. 0% with placebo), a large proportion of patients achieved stable disease, leading to a disease control rate ~51%. Importantly, there was a trend toward improved overall survival (OS). In the final analysis adjusting for crossover, ivosidenib was estimated to improve median OS from 5.1 months on placebo to 10.3 months, roughly halving the risk of death (HR: ~0.49; [10]).
HER2 amplification/overexpression—HER2-targeted therapies
While no HER2-targeted agent has received broad formal approval yet, specifically in BTC, clinical trials and real-world studies have shown clear benefit, and treatment guidelines recommend HER2-directed therapy for advanced BTC that overexpresses HER2. One approach is to use combinations of monoclonal antibodies against HER2. The phase II MyPathway basket study evaluated dual HER2 blockade (trastuzumab + pertuzumab) in patients with HER2-altered BTC. In that trial, among 39 BTC patients the ORR was 23% with a median PFS of 4.0 months [11].
A more potent strategy has been the use of antibody–drug conjugates (ADCs) targeting HER2. Trastuzumab deruxtecan (T-DXd), an ADC comprising an anti-HER2 antibody linked to a topoisomerase inhibitor payload, has demonstrated robust activity in HER2-expressing BTC. In the single-arm HERB trial from Japan, T‑DXd was given to patients with advanced, refractory BTC who were HER2-positive (IHC 3+ or IHC 2+ with gene amplification). The results showed an ORR of 36.4% in HER2-positive BTC. Median PFS was about 5.1 months in the HER2-positive group. Moreover, the global phase II DESTINY-PanTumor02 study recently reported an ORR of 56.3% in HER2 3+ BTC treated with T‑DXd, with a median PFS of 7.4 months [12].
Another novel agent is zanidatamab, a bispecific antibody that binds two distinct HER2 epitopes. In the phase IIb HERIZON-BTC-01 trial, zanidatamab showed an ORR of 41% in previously treated HER2-positive BTC, with a median PFS of 5.5 months [13].
BRAF V600E and KRAS G12C mutations—KRAS/BRAF/MEK inhibition
The efficacy of dabrafenib + trametinib in BTC was shown in the ROAR basket trial, which included 43 patients with BRAF V600E-mutated biliary tract cancers. Among these patients (most of whom had iCCA), the ORR was 51% (95% CI: 36–67%), with durable responses. The median PFS was around 9.0 months, and 30% of patients remained progression-free at 1 year. Median overall survival was ~14 months [14].
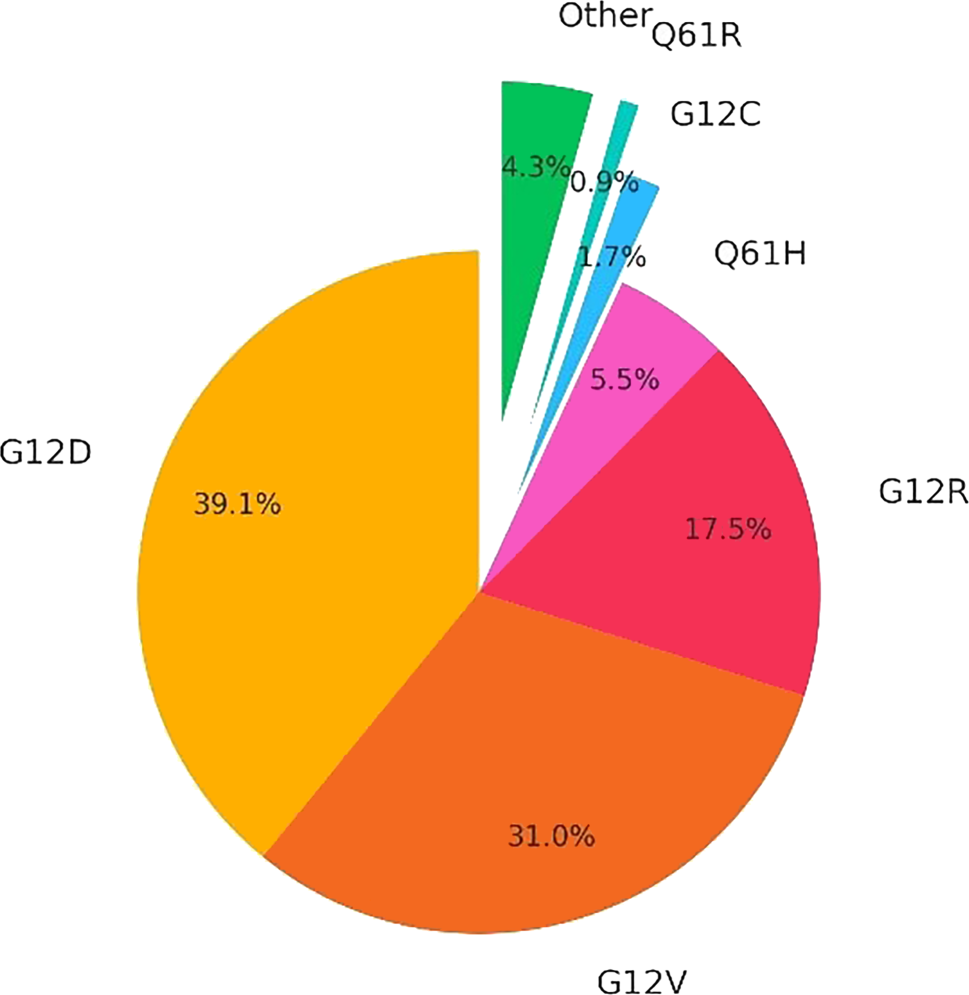
KRAS G12C is also an interesting target for targeted therapy, actionable by sotorasib and adagrasib [15, 16].
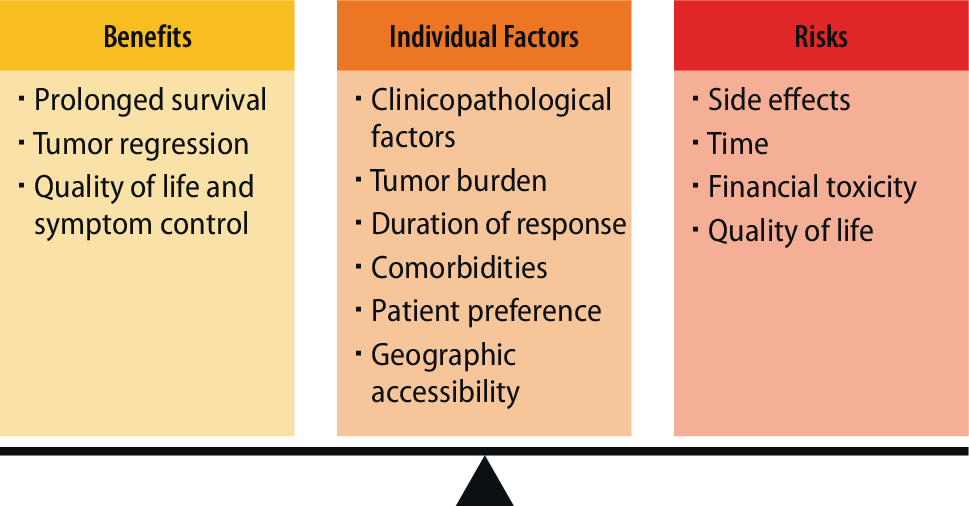
Integrating molecular profiling into routine BTC care can benefit from a proactive and structured approach. The following recommendations may help optimize its implementation:
Early and broad testing: It is advisable to initiate comprehensive genomic profiling (e.g., next-generation sequencing) at the time of advanced BTC diagnosis to ensure timely availability of molecular data to inform second-line treatment decisions or clinical trial eligibility [17].
Inclusion of fusion detection: It is important to ensure that the testing platform includes the capability to detect gene fusions, particularly FGFR2. If DNA-based assays are used, complementing them with RNA-based fusion panels may be recommended to improve sensitivity for detecting fusions and rearrangements [17].
Liquid biopsy as an alternative: When adequate tissue samples are unavailable, circulating tumor DNA (ctDNA) testing may be a viable option. Positive results (e.g., FGFR2 fusion detection) can help guide treatment decisions. However, negative results should be interpreted cautiously due to the lower sensitivity of liquid biopsy [17].





Comments (0)