
Remember me
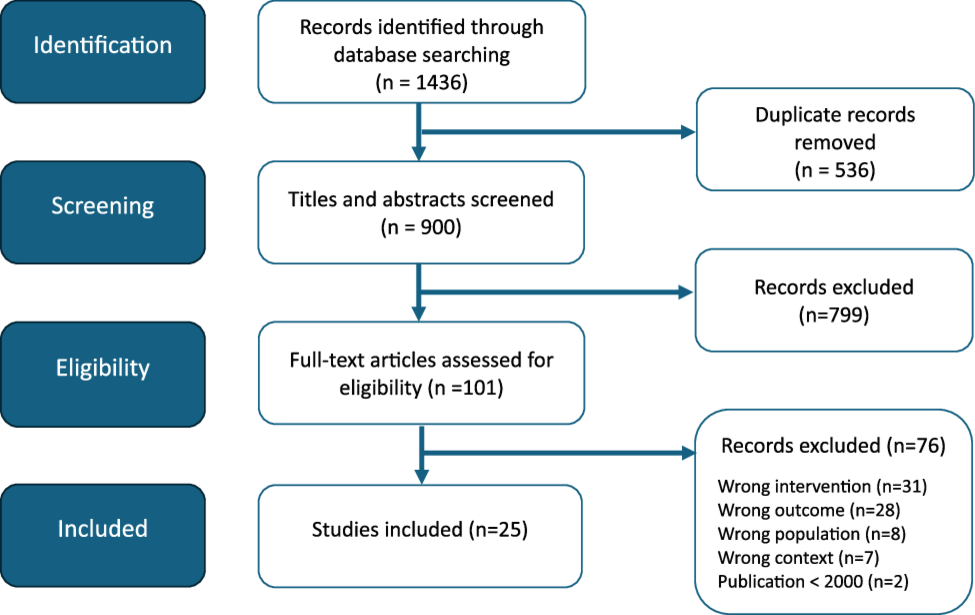






The search strategy yielded 1,436 articles, with 536 duplicates subsequently removed. Thus, 900 articles were screened by title and abstract, resulting in an initial selection of 101 studies. Eligibility assessment excluded 76 articles based on the established criteria. Studies with the wrong context (not addressing major neurocognitive disorders) or population (unable to distinguish caregivers in the results, general population, or healthcare providers) were not retained. Additionally, articles with interventions not included in the inclusion criteria (e.g., Do-Not-Resuscitate directive) or outcomes (e.g., caregiver’s experience, not addressing caregiver’s knowledge, attitudes, or representations) were excluded. Consequently, 25 articles were selected for analysis. The details of this selection process are presented in Fig. 1.
Fig. 1 Study characteristics
Study characteristicsThe selected articles were published between 2006 and 2022, most (n = 19) after 2016. The studies were conducted in the United Kingdom (n = 8), United States (n = 5), Canada (n = 4), Belgium (n = 3), Israel (n = 2), Brazil (n = 1), Netherlands (n = 1) and Italy (n = 1) (see Table 1). The research designs were predominantly qualitative (n = 17), with data collection methods primarily involving interviews (n = 14), focus groups (n = 1), a combination of those methods (n = 1) or nominal group technique (n = 1). Most studies had fewer than 60 participants (n = 16).
Table 1 Characteristics of included studiesParticipant characteristicsCaregivers made up the entire sample (n = 12) or a subgroup (n = 13) of the selected articles, totaling 1,545 participants (see Table 1). Of these, 73% were women. The average age of participants was 64 years, with a range from 20 to 92 years. The relationship between the senior with major neurocognitive disorders and the caregiver was primarily spousal (54%) or parent-child (38%).
Mapping of included studiesTable 2 presents a summary of the included articles, according to the concepts and subjects they explore. Most of the analyzed articles addressed multiple concepts and topics simultaneously. Specifically, knowledge, attitudes, and representations were covered in 48% (n = 12), 80% (n = 20), and 72% (n = 18) of the reviewed studies, respectively. In addition to the palliative care approach (n = 12), the selected articles explored various PEoLC practices, including advance care planning (n = 11), hospital transfer (n = 3), treatment withdrawal (n = 2), artificial nutrition and hydration (n = 4), continuous palliative sedation (n = 1), and medically assisted dying (n = 7). Since there is a lack of evidence regarding the benefits of artificial nutrition and hydration in the context of neurocognitive disorders, this intervention is considered in this review to be invasive, with assisted oral feeding by a third party as an alternative [18, 23].
Table 2 Overview of scientific articles on caregivers' knowledge, attitudes, and representations of palliative andend-of-life careRegarding the palliative care approach, this was frequently analyzed from the perspective of representation, mostly in terms of perception and understanding (n = 10). Among the PEoLC practices, knowledge (n = 7) and attitudes (n = 7) regarding advance care planning, as well as attitudes towards medically assisted dying (n = 6), were the most studied topics. In contrast, knowledge about artificial nutrition and hydration (n = 1) and medically assisted dying (n = 1), attitudes towards continuous palliative sedation (n = 1), and representations of hospital transfers (n = 1) were the least studied themes. Additionally, the included studies did not address knowledge and representation of treatment withdrawal and continuous palliative sedation, as well as knowledge about hospital transfers.
Content analysis of caregivers’ knowledge, attitudes, and representations of PEoLCTo better understand caregivers’ perceptions of PEoLC, a content analysis was conducted to explore and analyze their knowledge, attitudes, and representations in the included studies.
KnowledgeThe reviewed articles indicated that caregivers had a general understanding of the palliative care approach but limited knowledge of specific PEoLC practices. More specifically, two studies reported that most caregivers (62–85%) declared they had partial or good knowledge of the subject [24, 25]. In contrast, Gabbard et al. (2020) found that only 34% of participants considered their knowledge to be adequate [26].
Regarding caregiver’s knowledge of PEoLC practices, Pei et al. (2022) found a low level of knowledge about the use of tube feeding, while Vilela and Carameli (2009) reported that only 25% of participants could correctly define euthanasia [27, 28]. Studies on advance care planning revealed a lack of knowledge on the subject, with most participants being unfamiliar with the term “advance care planning” or its purpose [29,30,31,32]. Furthermore, Moss and al. (2018) noted that participants struggled to differentiate an advance directive from wills, as both were associated with documenting wishes and preferences, whether health-related or not [33].
AttitudesWithin studies addressing caregivers’ attitudes towards PEoLC practices, one study reported a certain consensus among participants concerning palliative sedation. Indeed, 69% of caregivers were supportive of this practice if it was provided to a terminally ill person with major cognitive disorders experiencing evident suffering, with the goal of alleviating that suffering [34].
Otherwise, articles examining caregivers’ attitudes towards EoLPC practices reported more divided perspectives regarding palliative care approach, advance care planning, artificial nutrition and hydration, hospital transfers, medically assisted dying and treatment withdrawal. More precisely, caregivers’ attitudes toward care goals varied across studies, with the preference for comfort care over life-prolonging treatments ranging from 40 to 90% [24, 25, 35, 36].
Most studies addressing advance care planning highlighted a positive attitude towards this practice, emphasizing that caregivers acknowledged the importance of documenting patient preferences [31, 33, 37, 38]. However, Sussman et al. (2021) and Van Rickstal et al. (2022) observed that participants did not consistently initiate these discussions with their loved ones [31, 38]. Additionally, Gabbard et al. (2020), Poole et al. (2018) and Van Rickstal et al. (2019) reported a more divided stance on advance care planning among participants [26, 32, 39]. In these studies, caregivers expressed varying opinions regarding the significance and usefulness [32, 39], while 43–45% of caregivers said that there was no need to discuss goals of care with the physician [26].
Variation in caregiver’s attitudes toward artificial nutrition and hydration were observed. In Rurup et al. (2006), 65% of participating caregivers agreed with the statement: “When a patient in the advanced stages of dementia refuses to eat and/or drink, this should be respected at all times” [40]. Conversely, in studies examining attitudes toward tube feeding in the context of difficulty eating and drinking, authors found that 33–35% of participants opted for tube feeding, while 24–33% preferred oral feeding by another person. Additionally, 33–41% remain neutral or did not take a position [27, 35]. For their part, Thuné-Boyle et al. (2010) reported that many participants thought that tube feeding should be offered as long as patients are comfortable [41].
Regarding hospital transfers, Poole et al. (2018) reported that all caregivers surveyed preferred end-of life care to be provided in their loved one’s current living environment, regardless of the type of setting, rather than opting for a hospital transfer [39]. Hochwald et al. (2021) reported that 74% of caregivers whose loved one received standard home care favored hospital transfer compared to 20% of those whose loved one received palliative care at home [35].
Moreover, caregiver’s perspectives and levels of acceptance regarding medically assisted dying varied across studies. Bravo et al. (2018; 2019; 2021) found that 50% of caregivers supported medical aid in dying at an advance stage and 72% at a terminal stage of illness [34, 42, 43]. In contrast, many participants in the study by Tomlinson et al. (2015) expressed discomfort with assisted dying [44] and 78% opposed euthanasia in the study by Vilela and Caramelli (2009) [28].
Support for medical aid in dying among caregivers for individuals with major neurocognitive disorders who had written advance directives ranged from 68 to 91% [34, 40, 42, 43]. Conversely, Tomlinson et al. (2015) indicated that all participants supported the view that individuals with major neurocognitive disorders should receive medically assisted dying while they are still capable of giving consent, although this may lead some people to request assisted dying earlier than they would wish in order to avoid being ineligible later on [44].
Caregivers’ attitudes towards treatment withdrawal were examined in the context of health deterioration in individuals with major neurocognitive disorders requiring antibiotics [43]. Some caregivers expressed ambivalence towards treatment withdrawal, with an acceptability ranging from approximately 30–45% at an advance stage and 23–58% at the terminal stage of illness [43]. In the study by Thuné-Boyle et al. (2019), participants considered the use of antibiotic important, with 95% agreeing that individuals with neurocognitive disorders should always receive antibiotics for infections such as pneumonia [41].
RepresentationsWhile caregivers shared some consensus on what defines quality palliative care, their beliefs varied regarding the palliative care approach and PEoLC practices. Authors identified elements that caregivers considered essential in providing quality palliative care for their loved one. Participants emphasized that palliative care should prioritize respecting the individual’s identity and uniqueness beyond their illness [29, 33, 39, 45,46,47]. This involved addressing basic needs, supporting social and recreational activities, ensuring physical and psychological comfort, and respecting the cultural beliefs of individuals with major neurocognitive disorders [29, 31, 33, 37, 39, 45,46,47]. Palliative care was ideally provided by trained, respectful, and compassionate professionals, preferably in the home or a comparable setting [31, 33, 37, 39, 45,46,47]. However, Gabbard et al. (2020) and Hill et al. (2017) highlighted that caregivers acknowledged cognitive decline can hinder engagement in leisure activities and the incorporation of cultural beliefs at end-of-life [26, 37].
Some authors highlighted variations in caregivers’ beliefs about the palliative care approach. While 43% of participants associated palliative care with oncology patients or those at end of life [25], 10% believed it hastened death, and another 10% perceived comfort care as a form of abandonment [24].
About artificial nutrition and hydration, some caregivers considered this practice as a “basic” life-prolonging measure that should be accessible to everyone, including those with major neurocognitive disorders [35, 41]. From this perspective, withholding a feeding tube was considered unacceptable or even criminal [35, 41]. Conversely, other participants viewed tube feeding as a violent act of forced-feeding a vulnerable person [35] and that forgoing artificial nutrition and hydration was almost always followed by a peaceful death [40].
Moreover, Poole et al. (2018) noted that participants perceived hospital transfers as distressing and disruptive for individuals with major neurocognitive disorders, given the unfamiliar environment and the presence of strangers [39].
In the Kermel-Schiffman and Werner (2020) study, some participants viewed advance care planning as means of maintaining decision-making autonomy and responsibility for end-of-life care in the event of incapacity [48]. It was also viewed as means of avoiding pain, excessive intervention, and prolonging a meaningless life [48]. Other caregivers voiced doubts regarding the extent to which advance care planning can ensure control, viewing it instead as a process lacking clear outcomes and subject to potential misinterpretation by healthcare professionals [47]. Furthermore, Sussman et al. (2021) and Van Rickstal et al. (2019) observed that some caregivers perceived future planning discussions as potentially harmful, as they could confront the senior with major neurocognitive disorders with anticipated losses [32, 38]. As a result, avoiding advance care planning discussions was seen as a way to protect their loved one [38].
Studies found some consensus among participants regarding the right to choose one’s own death for all individuals, including those with neurocognitive disorders [34, 40, 43, 44]. From this perspective, several caregivers in the Dening et al. (2013) study felt that medically assisted dying was a way of maintaining control [47]. However, in the Tomlinson et al. (2015) study, some participants viewed assisted dying as meaning that the life of a loved one with major neurocognitive disorders was no longer valued [44]. Additionally, some participants viewed this practice as contrary to the principles of care that prioritize the preservation of life, believing that death should be accepted rather than controlled. Treatment withdrawal was also perceived as a form of euthanasia [44].
Comments (0)